
Abstract
A 48-year-old woman presented with fatigue and vaginal spotting and was subsequently diagnosed with squamous cell cancer of the cervix. Computed tomography and positron emission tomography scans suggested widespread disease including possible involvement of the right ventricle. A 2D echocardiogram with Doppler showed a large right ventricular mass obstructing the tricuspid valve inflow. This report demonstrates the use of echocardiography and Doppler ultrasound in the diagnosis of a rare case of cardiac metastasis from cervical cancer.
Introduction
Cervical cancer with metastasis to the heart is a rare occurrence and associated with a poor prognosis. 1 Patients may present with symptoms of heart failure, lower extremity edema, or an abnormal electrocardiogram showing myocardial infarction pattern. Although there are a number of imaging methods for demonstrating cardiac involvement with tumors such as magnetic resonance imaging (MRI), computed tomography (CT), and positron emission tomography scan (PET), echocardiography remains an excellent bedside tool for providing detailed anatomic and hemodynamic information in these cases.1–5
Case Report
A 48-year-old female was referred to our facility for evaluation of squamous cell cervical carcinoma. She reported a 2-year history of fatigue and vaginal spotting with a normal Pap smear. One year later, she underwent a cervical biopsy that revealed an invasive poorly differentiated, large cell, non-keratinizing squamous cell carcinoma with extensive necrosis. At the time, she was being considered for external beam radiation and high dose brachytherapy for the management of stage IIB cervical cancer. However, further workup with a CT scan of the chest, abdomen, and pelvis revealed a cervical mass with involvement of the uterus and bladder suggesting more widespread disease. Subsequently, she underwent a positron emission tomography scan from the skull to midthigh. The findings included an incidentally noted area of increased focal activity of fluorodeoxyglucose (18-FDG) uptake corresponding to the right ventricle adjacent to the septum. The possibility of a metabolically active right ventricular mass was considered. As a result, she underwent a course of radiation implants, external beam radiation, and chemotherapy.
The patient returned to the gynecology clinic 6 months later with a 4-5 week history of lower extremity edema, and a repeat CT scan demonstrated a large right ventricular mass. An echocardiogram was performed using a Philips Sonos 5500 with S3 transducer (Philips Medical Systems, Andover, MA). The machine settings, including 2D gain, time gain compensation, and depth were optimized for each view throughout the study. The echocardiogram showed a large heterogenous mass (5 cm × 4 cm) involving the RV inflow, the trabecular portion of the RV, and extending to the RV outflow tract (Figure 1). The mass appeared to be broadly attached to the right ventricular wall, displacing the entire tricuspid valve apparatus and producing severe right ventricular inflow stenosis (Figure 2). The inferior vena cava (IVC) was dilated, indicating an increased right atrial (RA) pressure. A calculated mean gradient across the tricuspid valve was measured at 8 mmHg, consistent with severe stenosis (Figure 3). There was no evidence of mass in the right atrium or inferior vena cava, though a small pericardial effusion was seen. Pulsed wave spectral Doppler showed flow reversal in the hepatic veins in early diastole, suggesting constrictive physiology.
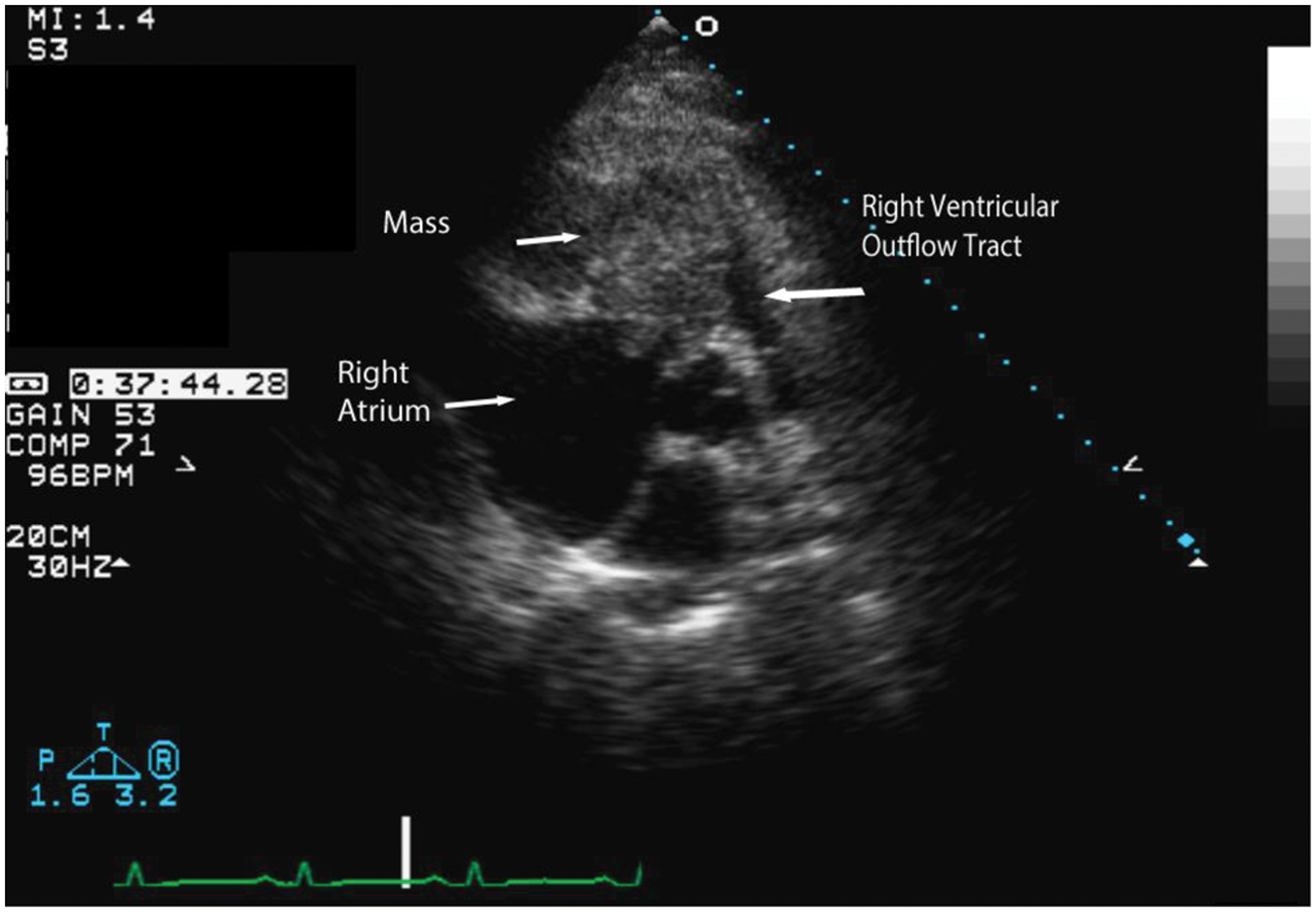
Large heterogenous mass involving the right ventricular (RV) inflow and extending to the RV outflow tract seen in the parasternal short axis at the aortic valve level.
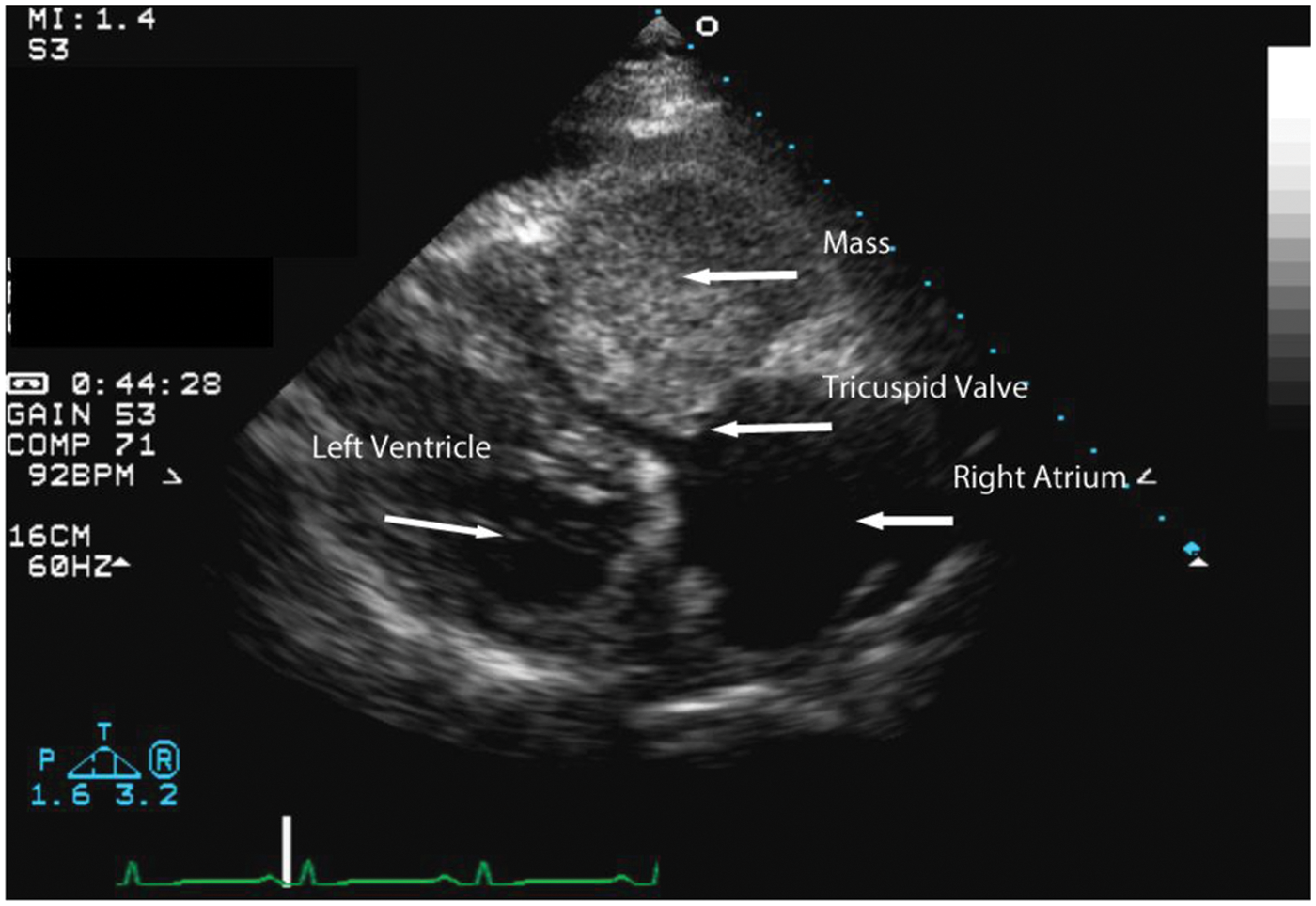
In the right ventricular inflow view the mass filled the entire right ventricular cavity leaving only a small inflow tract. The tricuspid valve showed severely restricted motion due to encroachment by the mass.
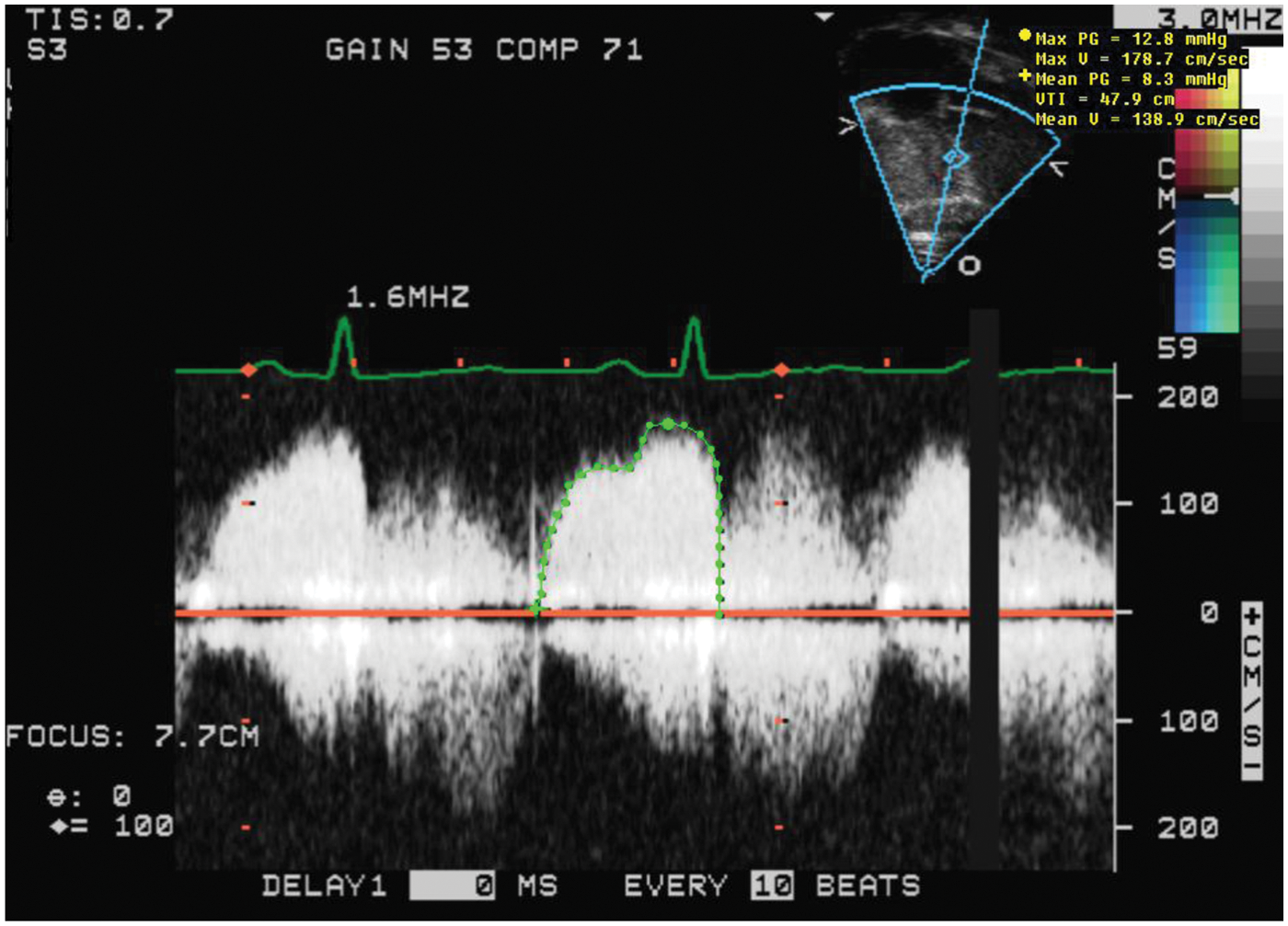
Continuous wave Doppler from the apical 4 chamber view enabled a calculated mean pressure gradient across the tricuspid valve of 8 mmHg.
Based on these findings, a percutaneous biopsy of the right ventricular mass was performed using ultrasound guidance. The biopsy showed metastatic squamous cell carcinoma. The patient was started on a course of chest radiation in addition to chemotherapy. A follow-up echocardiogram was performed one month later, which showed the mass to be diminished in size. A subsequent CT scan demonstrated the presence of a left renal vein thrombosis extending to the IVC. She was treated with enoxaparin and warfarin and received chemotherapy but expired 3 months later.
Discussion
Every year in the United States, about 12,000 women are diagnosed with invasive cervical cancer. 6 Half of these women are under 55 years of age. Although there are a number of clinical factors that increase the risk for cervical cancer, infection with human papillomavirus (HPV) appears to be the main determinant. Other factors increasing the risk include lack of regular Pap tests, smoking, and a weakened immune system. 6
Squamous cell cancer of the cervix originates in the cells on the surface. These cells may break away from the original tumor and enter the lymph vessels that branch into all the tissues of the body where they can produce metastatic lesions. Cervical cancer spreads most often to nearby tissue in the pelvis, lymph nodes, or the lungs, but may also involve the liver or bones. In rare cases, metastases to the heart may occur. A 1999 review of the literature disclosed only 14 cases of uterine cervical carcinomas with right intraventricular metastasis, confirming the rarity of this diagnosis. 2 Reported cardiac involvement has been universally right ventricular with the exception of a 2006 report of an intra-atrial tumor extending through the inferior vena cava from the site of a para-aortic lymph node metastasis. 3
Patients may present with signs and symptoms of lower extremity edema, heart failure, chest pain, or abnormal EKG. An echocardiogram can provide detailed information regarding the presence or absence of tumor, IVC involvement, and cardiac function with little discomfort to the patient. The evaluation of symptomatic gynecologic cancer patients should always include careful cardiac imaging with particular attention to the pericardium, the right heart, and cavae to look for obstruction or metastases. As in our case, multiple imaging modalities such as MRI, CT, and PET may also play important roles in the diagnosis and evaluation of these patients.1–4
In all the cases reviewed and reported, confirmation of the tumor type was made by either biopsy in the catherization lab or by direct surgical removal.1–4 Although multimodality treatment has been shown to provide some palliative benefit and prolonged survival, cervical cancer with metastasis to the heart continues to carry a poor prognosis, with a mean survival time from diagnosis of 4 months. 4
Conclusion
Although cardiac involvement remains uncommon, it should be suspected in women with a history of cervical cancer. 5 Echocardiography can be performed easily with little discomfort to these patients providing detailed information regarding the size and location of the tumor as well as hemodynamic information, yielding important prognostic information. In the case presented, echocardiography confirmed the presence of the cardiac tumor with inflow stenosis and provided guidance for the performance of the percutaneous right ventricular biopsy of the mass.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.