
Abstract
The liver is one of the principal organs in the body and is involved in over 500 physiological functions related to metabolism, digestion, immunity, and storage of nutrients. Given that there are a number of approaches to measure liver length through diagnostic 2D sonography, this work was undertaken to determine the most accurate measurement of this organ. Cadaveric specimens (n = 21) were employed to assess measurements in the midclavicular line (MCL) and the midaxillary line (MAL). Each measurement was calculated in anteroposterior (AP) and craniocaudal (CC) planes. In addition, in situ measurements were obtained by accessing the organ through the anterior thoracoabdominal wall. Statistical differences were detected between MCL and MAL measurements (P < .05), and a positive correlation between MAL CC and in situ anterior measurements were noted (r = 0.97). Liver size, as assessed through in situ measurements, varied as a funtion of BMI and waist circumference (P < .05). It is concluded that the craniocaudal measurement of the right lobe of the liver in the midaxillary line, from the uppermost right hemi-diaphragm to the inferior tip of the right lobe through a horizontal line parallel to the anterior liver wall, is the most accurate measurement of the organ by sonography.
Introduction
Accurate measurement of the liver by sonography is particularly relevant when hepatic disease is suspected. As a noninvasive and inexpensive method when compared to other methods,1–3 diagnostic sonography is useful to evaluate liver size and texture. In recent years, diagnostic sonography has shown specificity and positive predictive value in assessing the liver and its various diseases.4–6 However, according to a number of validated sources, measurement of liver length still varies greatly across modalities and techniques used by the operator.7–12 It is clear that liver disease alters the texture of the organ and sometimes its size as well. 13 Therefore, it becomes an important issue to use the most accurate measure of liver size in the hope of detecting gradual changes in organ size. In addition, it would be clinically advantageous to establish the range for normal liver sizes according to anthropometry and sex of the patient.
The liver occupies 5% of the mature fetus’s body cavity, and it constitutes 2.5% of the adult body weight. 13 Liver weight in the adult male is approximately 1400 to 1500 g, and it serves over 500 physiological functions related to metabolism, digestion, immunity, and storage of nutrients.14–18 Access for accurate measurements of the liver through imaging techniques is not always possible, which produces a wide range of measurements across techniques. This is partly due to variations in shape and inherent limitations of imaging techniques to capture the appropriate anatomical boundaries of the organ. 19 Therefore, it is of interest to address this significant issue in the field by contrasting several measurement techniques for the right lobe of the liver (RLL) using ultrasonography with direct anterior in situ measurements of the organ from cadaveric specimens.
Materials and Methods
Specimens
Cadaveric specimens were obtained from the Pathology Laboratory, Puerto Rico Institute of Forensic Science (IFS-PR), and the Department of Anatomy and Neurobiology, School of Medicine, University of Puerto Rico (SoM-UPR) and were evaluated over a one-month period in June 2013. Approval of the study protocol was obtained from the Anatomical Donation Board (ADB), Medical Science Campus, UPR. Sonographic liver measurements were obtained from 27 fresh cadaveric specimens without any evidence of right upper quadrant trauma. Six cadavers ultimately were excluded from the study because in situ measurements were not done. Although an effort was made to include specimens from both sexes, the final sample consisted of 18 male and 3 female cadaveric specimens. Data on patient age, sex, weight, and height for each specimen were obtained from the Institute of Forensic Science or Anatomical Donation Board records. Body mass index (BMI) was calculated in the normal fashion by BMI = weight (kg) / height (m)2. The BMI values were classified according to: underweight (BMI ≤ 18.5 kg/m2), adequate weight (BMI = 19.0-24.9 kg/m2), overweight (BMI = 25-29.9 kg/m2), and obese (BMI ≥ 30 kg/m2).20,21 Cadavers were placed in the supine position for measurement of waist circumference (WC) in centimeters at the level of the navel. Given that 18 out of 21 specimens were males, waist circumference was categorized by using 102 cm as the cutoff reference value for a typical male waist circumference.20,21 The images shown in Figure 1 are typical examples of the measurements taken.
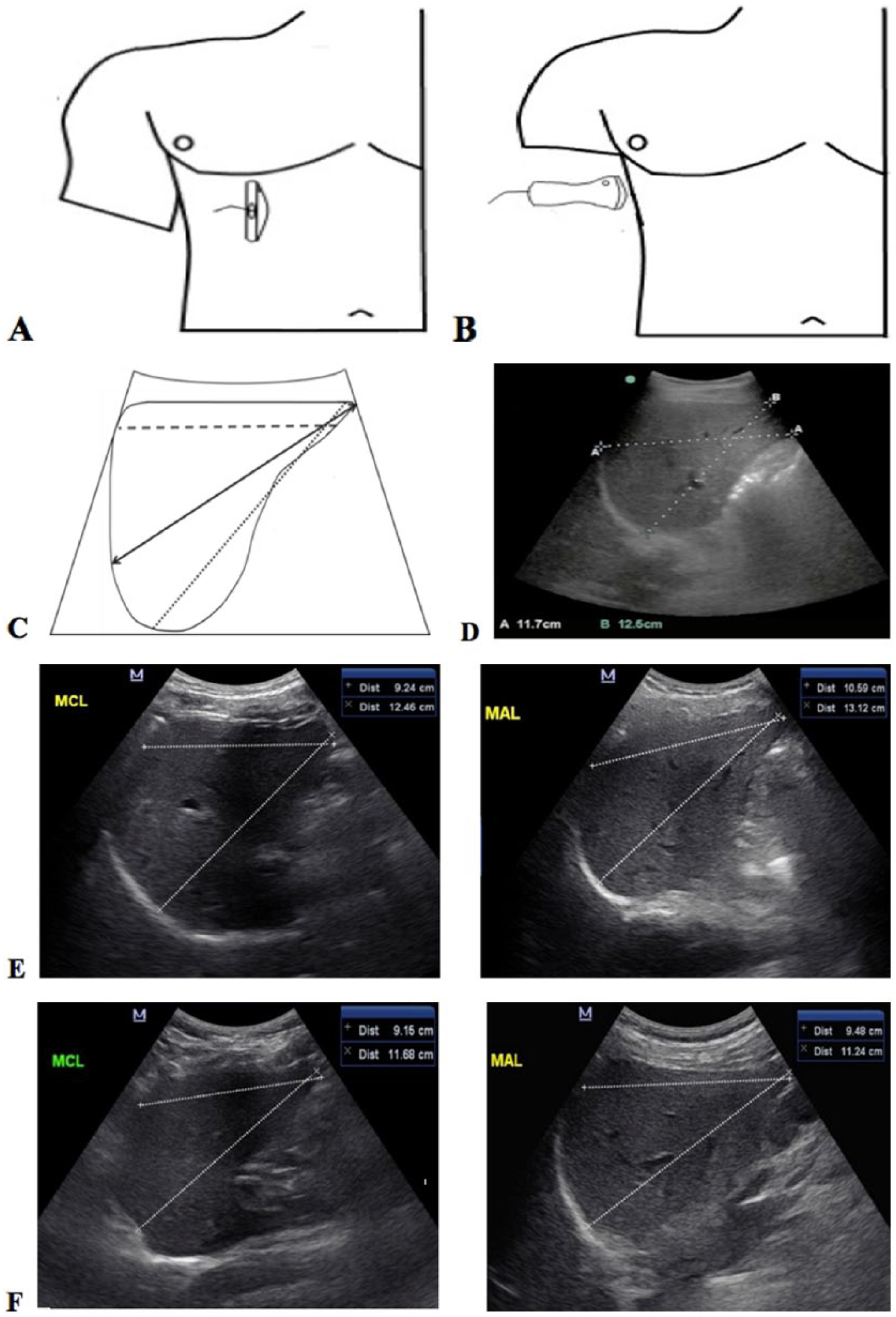
Sonographic techniques for measurement of the length of the right lobe of the liver (RLL). (A) Diagram shows the position of the transducer using the midclavicular line. (B) Diagram shows the position of the transducer using the midaxillary line. (C) Diagrammatic representation of RLL measurements. The solid line and round dotted line are usually termed a craniocaudal plane, but the line drawn for the measurement is oblique. The dashed line represents a craniocaudal measurement taken from the uppermost right hemi-diaphragm to the inferior tip of the right lobe through a horizontal line parallel to the anterior liver wall. (D) Sonographic image of the right lobe of the liver taken using the midaxillary line. The craniocaudal (A: 11.7cm) and oblique (B:12.5cm) measurements are shown. Note that in this image: (i) the inferior tip of the liver is not visible, and (ii) a rib overshadows part of the diaphragm dome. (E) and (F) Sonographic images of the liver of two normal volunteers that show the craniocaudal and oblique measurements of the entire RLL in the midclavicular line and midaxillary line planes. Each panel shows these measurements for the same patient.
Sonographic Examination and Data Acquisition
Sonographic scans were obtained using a SonoSite M-Turbo machine (SonoSite, Inc., Bothel, WA) with a 2.5 to 5.0 MHz curved transducer, provided by Diagnostic Imaging Supplies and Services (DISS-Puerto Rico). All sonographic images were obtained by a single author (B.L.R.C.) with 12 years of experience in sonographic examination and 8 years of experience as a sonography professor. In addition, images were independently evaluated and supervised by a second author (W.R-M.), the Director of Ultrasound at SoM-UPR since 1981. Sonographic images of the liver were obtained with the cadaver in a supine position. The right arm of each cadaver was placed above the head to facilitate access to the right upper quadrant. The first measurement was done in the right midclavicular line (MCL). Liver longitudinal diameter was measured craniocaudally (MCL CC) from the uppermost right hemi-diaphragm to the inferior tip of the right lobe (whenever visible) or to the most inferior boundary of the lobe through a horizontal line parallel to the anterior liver wall. In addition, liver measurements were obtained obliquely for anteroposterior measurements (MCL AP). Each cadaveric specimen was then placed in a left oblique position (15°–20°) for right midaxillary line measurements (MAL CC and MAL AP), using the approach described previously.
Figure 1 shows the approach taken to obtain 2D sonography measurements. Panels A and B show the positioning of the transducer for the MCL and MAL approaches, respectively. Panel C shows a diagrammatic representation of the ultrasonographic measures that are typically taken to assess liver size as well as those that were investigated in this study. The craniocaudal and oblique measurements of the liver in the MAL plane are shown in Panel D where the inferior tip is not visible. Panels E and F show the techniques for craniocaudal and oblique measurements of the entire RLL in the MCL and MAL planes, respectively, for two normal volunteers.
After sonographic imaging, the anterior thoracoabdominal wall of each cadaver was dissected by incising the wall with three cuts following a “Y” shape from the level of the first rib to dermatome T-12. The anterior portion of the diaphragm was dissected for better visualization of the liver without reaching the triangular or coronary ligaments. In situ measurements of the RLL along the anterior and anterolateral margins were obtained from the top to the bottom edge of the lobe.
Statistical Analysis
Data were expressed as mean ± standard deviation. The Shapiro-Wilk test for normality was employed to assess data distribution. 22 Two-tail paired t tests were used to compare liver measurements. One-way ANOVA and Tukey post hoc test were used to assess the effect of anthropometric measures and BMI on liver length. Statistical significance was considered to be a P value ≤ .05. All statistical analyses were performed using the statistical software program R3.0.2 (R Foundation, Vienna, Austria; free download available at http://cran.r-project.org).
Results
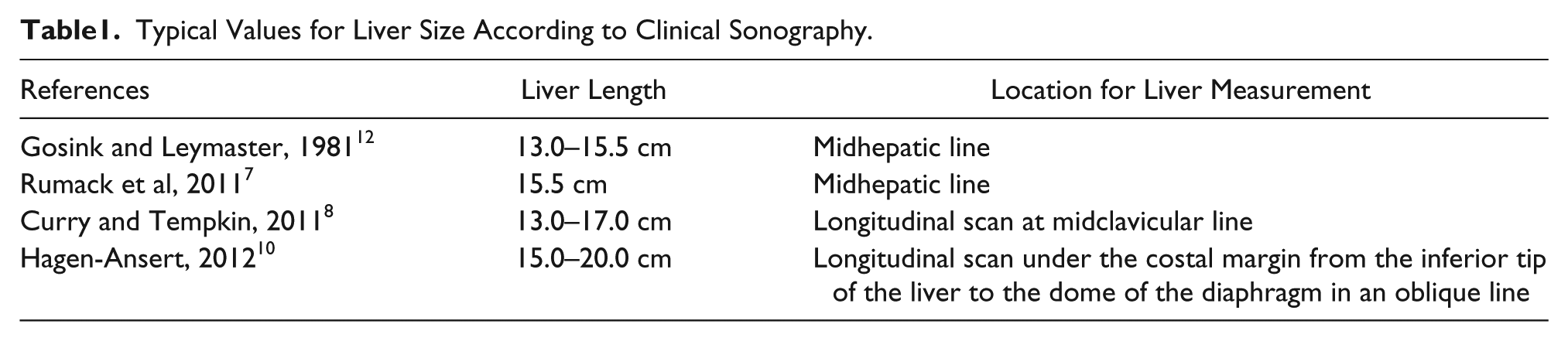
Cadaveric specimens were between 18 and 98 years of age at the time of death (55 ± 21 years). Table 1 shows reported typical values for liver size according to clinical sonography and radiology textbooks. Individual values found in this study of 21 cadaveric specimens for each measurement, with their mean and standard deviation values, are shown in Table 2. The Shapiro-Wilk test showed that the data in this study were normally distributed (analysis not shown). The average liver size according to direct anterior in situ measurement was 12.7 ± 1.44 cm (n = 21). It was not possible to obtain accurate MCL measurements from six cadaveric specimens due to poor visualization of the organ. It was possible to obtain accurate measurements from all cadaveric specimens in the MAL.
Typical Values for Liver Size According to Clinical Sonography.
Cadaveric Specimen Characteristics and Liver Measurements.
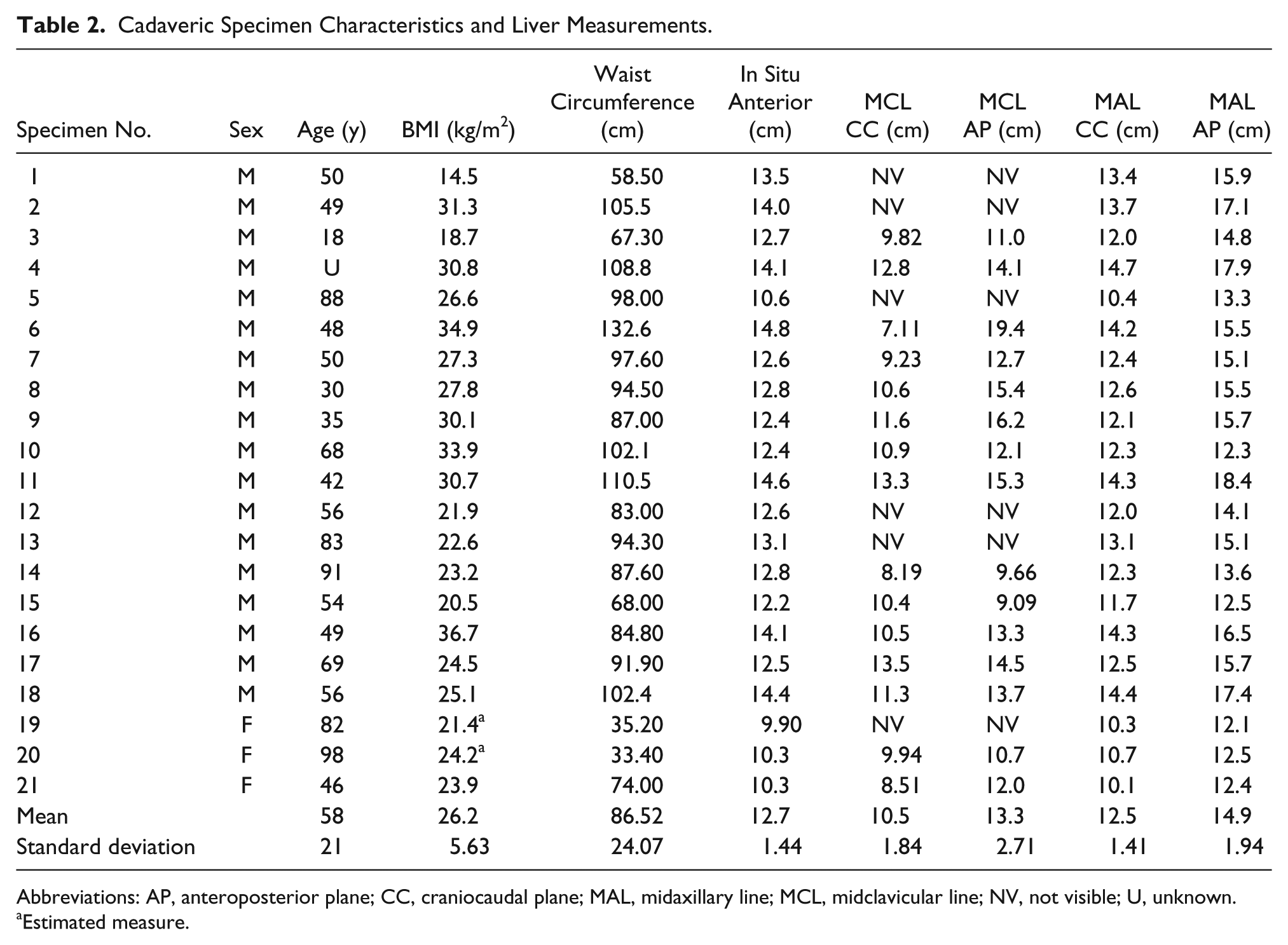
Abbreviations: AP, anteroposterior plane; CC, craniocaudal plane; MAL, midaxillary line; MCL, midclavicular line; NV, not visible; U, unknown.
Estimated measure.
MCL and MAL Measurements
The craniocaudal and anteroposterior measurements were statistically different from each other for MCL (P = .004) and MAL (P < .001) (Table 2). Correlation analysis for MCL and MAL showed low correlation between these measurements as well (Table 3). The correlation between sonographic measurements for MCL versus in situ anterior measurements showed low correlation, while the correlation between MAL and in situ anterior measurements was higher than the one obtained with MCL (Figure 2, Table 3). The strongest correlation was observed between MAL CC and in situ anterior measurements (Figure 2B).
Statistical Analysis for Measurements of the Right Lobe of the Liver.
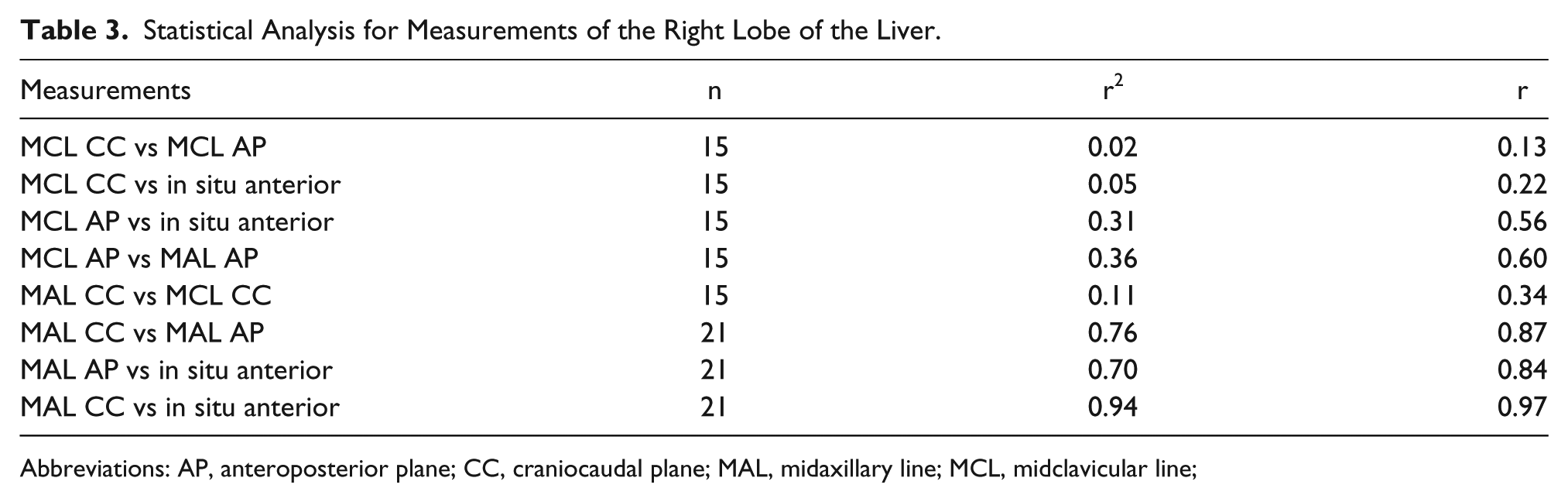
Abbreviations: AP, anteroposterior plane; CC, craniocaudal plane; MAL, midaxillary line; MCL, midclavicular line;
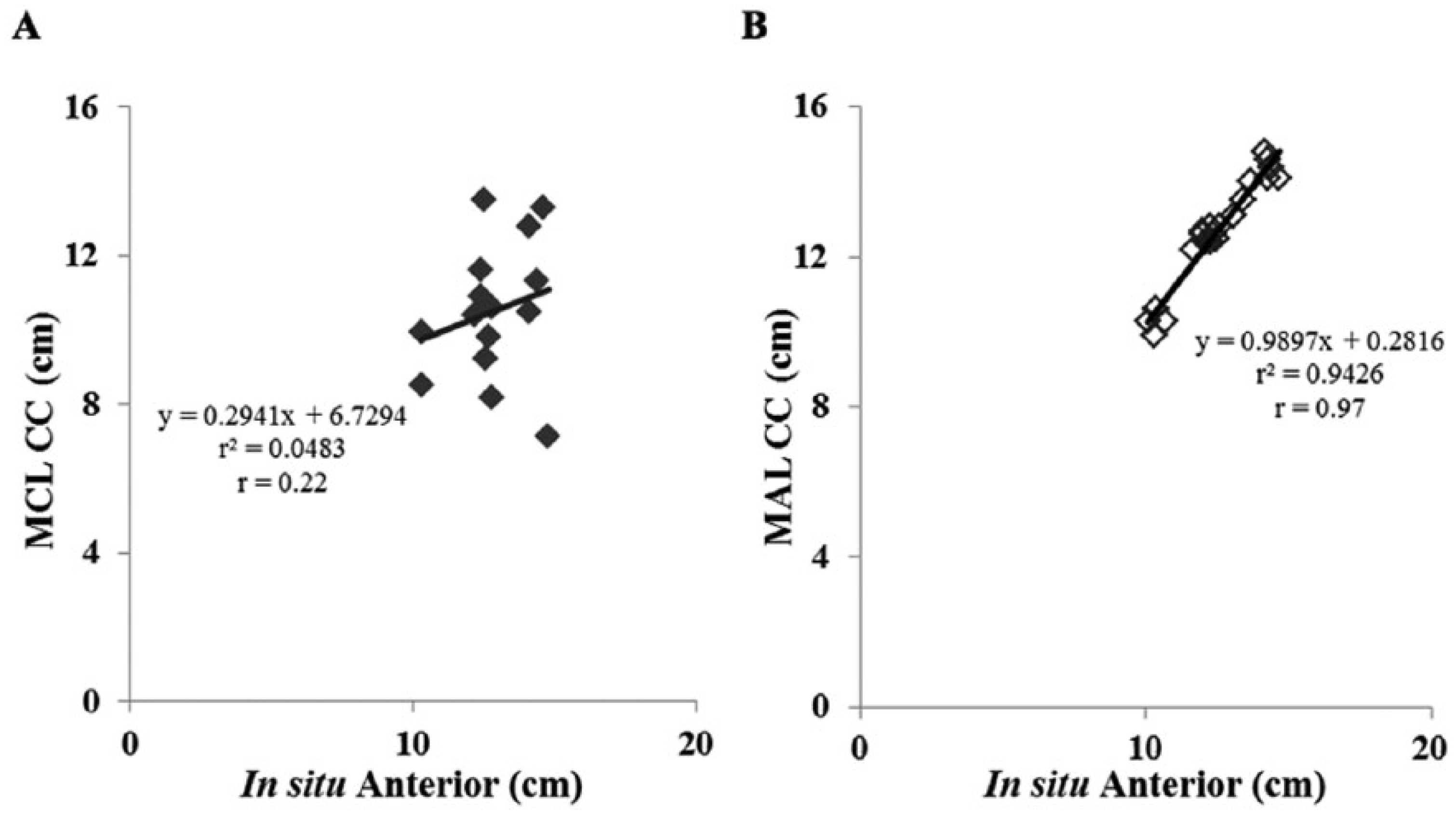
Regression and correlation analyses for measurements of the length of the right lobe of the liver. (A) Direct in situ anterior versus midclavicular craniocaudal (MCL CC) measurements. (B) Direct in situ anterior versus midaxillary craniocaudal (MAL CC) measurements.
Anthropometric Measures
The average body mass index (BMI) for all cadaveric specimens was 26.2 ± 5.63 kg/m2, and the average waist circumference was 86.5 ± 24.1 cm (Table 2). Figure 3A shows the anterior in situ RLL length as a function of BMI (underweight, adequate weight, overweight, and obese). Statistical analysis showed that anterior in situ RLL length varied according to BMI, F(2, 17) = 49.53, P < .001; underweight was not included in this analysis because there was only one case. A statistically significant difference in length was noted between adequate weight specimens and obese specimens (P = .0159). Figure 3B shows that waist circumference measured at the level of the navel varied according to BMI, F(2, 17) = 7.54, P = .004, and statistical differences were noted between adequate weight specimens and obese specimens (P = .005) and between adequate weight and overweight specimens (P = .05). Finally, analysis of anterior in situ RLL length as a function of waist circumference showed that specimens with waist circumferences above 102 cm had a significantly larger RLL length than specimens with less than 102 cm waist circumference (P = .003, Figure 3C).
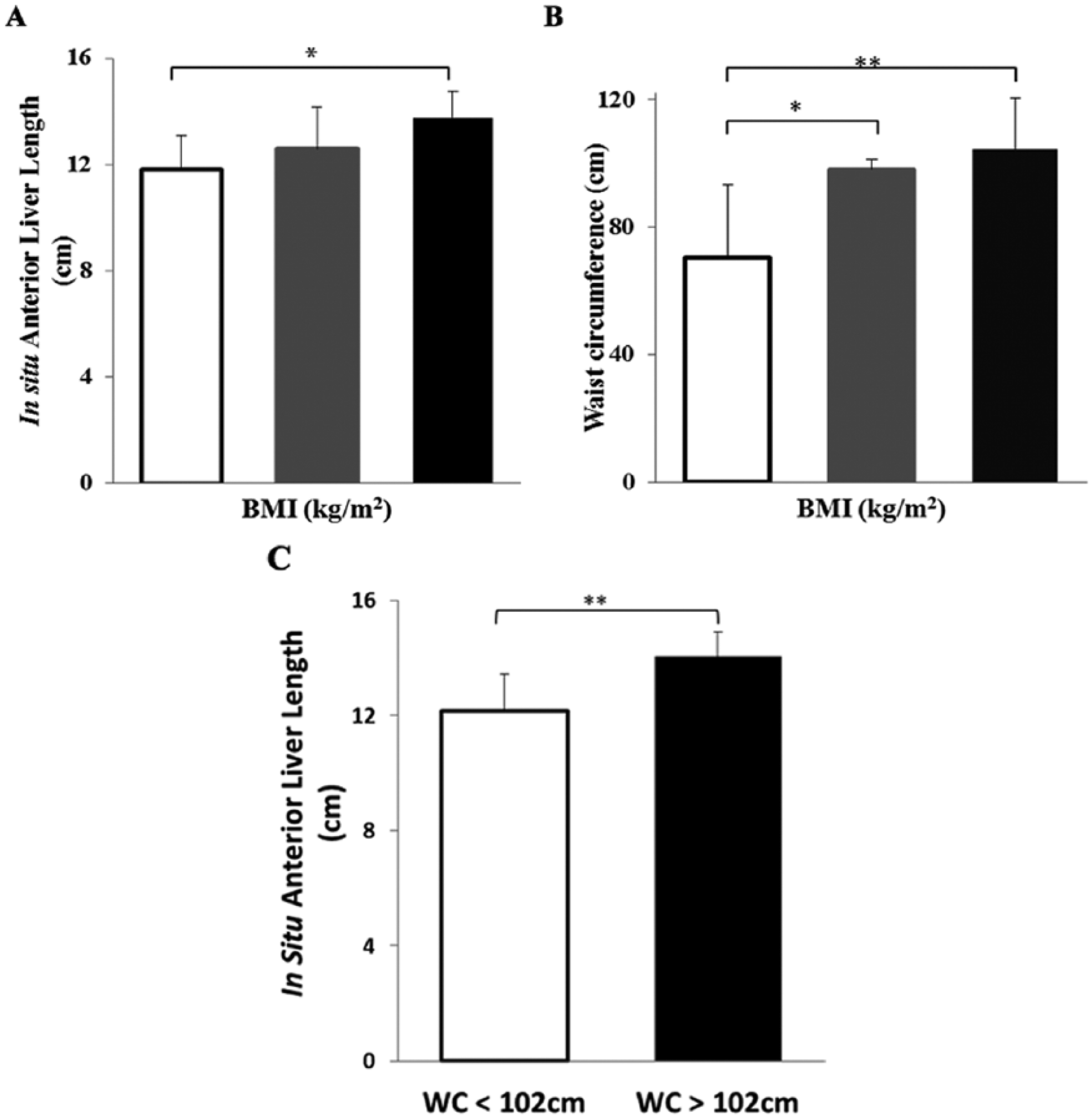
Comparison of mean cadaveric anthropometric data and direct in situ anterior measurements of the length of the right lobe of the liver. (A) Body mass index (BMI) groups versus in situ anterior liver length. (B) BMI versus waist circumference. (C) Waist circumference versus in situ anterior liver length. Errors bars show standard deviation values. Classification of BMI groups: adequate (19.0–24.9) (white bars for Panels A and B, n = 9), overweight (25–29.9) (gray bars for Panels A and B, n = 4), and obese (> 30) (black bars for Panels A and B, n = 7). *P ≤ .01–.005. **P ≤ .001–.0001.
Discussion
There is lack of consensus on standard reference values for sonographic measurements of the liver.13–16 For instance, sonographic measurement of this organ is most commonly performed with the patient in the supine position, and RLL length is assessed longitudinally in the midclavicular line. Traditionally, this measurement is considered as being obtained in the craniocaudal plane. 7 But the line drawn for this measurement is oblique, which in many cases overestimates liver length. By using cadaveric specimens, this study demonstrates that the most accurate measurement of RLL length is obtained in the craniocaudal plane along a midaxillary line. The RLL length was assessed from the uppermost right hemi-diaphragm to the inferior tip of the right lobe (whenever visible), or to the most inferior boundary of the lobe, through a horizontal line parallel to the anterior liver wall as shown in Figure 1, Panels D–F. When compared to in situ assessment of RLL, the concordance of RLL measurements in the craniocaudal plane along a midaxillary line was 97%.
Cooperation of the patient typically is required to access the entire RLL for organ measurement by ultrasonography. For instance, gases in the abdominal cavity, the rib cage, variability in organ anatomy such as shape and size, its location in three-dimensional space, the anatomical boundaries of the organ, and breathing of the patient are some of the factors that can hinder a high-quality visualization of the RLL by ultrasonography. By studying the gross anatomy of the liver across cadaveric specimens, it was noted that the right lateral inferior tip of the liver in the sonographic image is the longest portion of the right lobe. This portion is surrounded by the lateral edges of the ribs, which makes it difficult for accurate measurement by sonography. In addition, as this portion of the RLL shows anatomical variations in terms of morphology and length, it should not be taken into account to determine liver length or weight.
Even though assessment of the RLL in the craniocaudal plane along a midaxillary line is accurate, it is important to note that such measurement varies as a function of BMI and waist circumference. Specifically, obese specimens and specimens with waist circumference larger than 102 cm at the level of the navel had larger RLL values. This suggests that abdominal shape and size affect liver length. At this time, it is not possible to make a sound statement with regard to RLL size and sex because of the small sample of female cadavers in this study. Further studies will be necessary to determine whether there are gender differences in liver length and whether disease processes affect liver size in a sex-specific manner.
It is of clinical relevance to be able to detect early gradual change in hepatic size before a patient develops hepatomegaly by using the least expensive and least invasive imaging techniques. A panoramic view of the organ is always desirable in spite of the inherent limitations that are usually confronted to access the liver by ultrasonography. However, when the panoramic view is not feasible, based on the results of this study, it is proposed that ultrasonographic measurements of the RLL should be taken in the craniocaudal plane (from the uppermost right hemi-diaphragm to the inferior tip of the right lobe through a horizontal line parallel to the anterior liver wall) along a midaxillary line (see Figure 1D). In addition, it is proposed that standard reference values for liver length should be developed according to the anthropometry of the patient.
Conclusion
It is important to establish the most accurate way to assess liver length by sonography to assure consistency and establish ranges for normal values. Clinical follow-up with sonography of those patients who may develop liver disease is warranted before the occurrence of major health complications. In the best clinical scenario, particularly for those cases where the tip of the liver cannot be visualized in real-time sonographic images, panoramic views should be obtained for measurement accuracy. This study showed that the most accurate way to obtain measurement of the right lobe of the liver was from the uppermost right hemi-diaphragm to the inferior tip of the right lobe through a horizontal line parallel to the anterior liver wall through the midaxillary line. By using such an approach, it is expected that intra- and interobserver variability will be reduced. Moreover, the establishment of a conservative range of normal values for liver length by sonography according to the anthropometry of the patient would allow professionals to determine when a given measurement is indicative of liver pathology.
Footnotes
Acknowledgements
The authors wish to acknowledge Diagnostic Imaging Supplies & Services (DISS-PR), and Ms. Angeles Pérez in particular, for providing the ultrasound equipment that was used to complete this study. We also acknowledge the enthusiastic collaboration of forensic pathologists, forensic autopsy technicians, and auxiliary personnel of the Institute of Forensic Sciences of Puerto Rico throughout the data collection process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. JCJ is a Fellow of the Independent-Research Professional Development (I-RPD) Program, Medical Sciences Campus, University of Puerto Rico sponsored by the National Institute on Minority Health and Health Disparities (2U54MD007587).