
Abstract
Objective
Despite the recent advances in surgical techniques and perioperative care, liver resection (especially extended hepatectomy) is still a high-risk procedure with considerable morbidity and mortality. Experimental large animal models are the best option for studies in this regard. The present study was performed to present an easy-to-learn, fast, and multipurpose model of liver resection in a porcine model.
Method
Stepwise liver resections (resection of segments II/III, IVa/IVb, and VIII/IV) were performed in eight pigs with intraoperative monitoring of hemodynamic parameters. The technical aspects, tips, and tricks of this method are explained in detail.
Results
Based on the specific anatomical characteristics of the porcine liver, all resection types including segmental resection, hemihepatectomy, and extended hepatectomy could be performed in one animal in an easy-to-learn and fast technique. All animals were hemodynamically stable following stepwise liver resection.
Conclusion
Stepwise liver resection using stapler in a porcine model is a fast and easy-to-learn method with which junior staff and research fellows can perform liver resection up to extended hepatectomy under stable conditions.
Introduction
Liver resection is still the treatment of choice for malignant hepatic tumors. 1 , 2 Although the mortality rate following liver resection is now as low as 5% in experienced hepatobiliary centers because of improvements in perioperative care and advances in surgical techniques,3–5 extended hepatectomy (EH) is still a high-risk operation with a considerable morbidity rate. 6 The most important complications following EH include post-hepatectomy liver failure, intraoperative and postoperative bleeding, bile leakage, biliary fistulas, ascites, abdominal fluid collections, and abscesses. 3 , 4 Moreover, many patients cannot undergo curative EH because the potential remnant liver volume is too small.7–9
These challenging intraoperative and postoperative complications illustrate the need for a valid and reliable model to provide authenticated evidence. Experimental models can be used to develop effective methods of prevention, management, and treatment of complications in this regard. 10 Pigs are widely used in experimental studies because they are anatomically and physiologically similar to humans, readily available, and inexpensive. 11 The morphology and segmental anatomy of the porcine liver are very similar to those of the human liver and provide a simple template for resection procedures. 12 , 13 However, the literature contains no descriptions of a fast and easy-to-learn method for liver resection in a porcine model that can be learned and performed by junior staff or research fellows without major problems and without biasing the final results. Stapler hepatectomy is an easy-to-learn method that shortens the operation time and has morbidity and mortality rates comparable with those of other methods.14–18 This study was performed to present a simple method for liver resection up to EH in a porcine model that can be easily learned and rapidly performed by junior staff and young fellows.
Methods
We performed stapler hepatectomy in eight pigs and monitored the animals throughout the procedure. The necessary preoperative preparations and the surgical technique with a focus on special variations based on the porcine liver anatomy and our experience during the last several years are described below.
All animals received humane care according to institutional guidelines established for the Animal Care Facility at the University of Heidelberg at all stages of the experiment. The animals were housed at the Interfacultary Biomedical Faculty of Heidelberg University, where they underwent all procedures. The study protocol was approved by the Committee for Animal Care, Karlsruhe, Germany (AZ: 35–9185.81/G45/12). Analgesia during the surgical phase was performed with administration of buprenorphine (0.05 mg/kg) and metamizole (25–35 mg/kg). The dose was adjusted if necessary. At the end of the experiments, all animals were sacrificed during deep anesthesia (0.75%–1.5% isoflurane) by intravenous injection of potassium chloride (2 mmol/kg). The pigs were then monitored until no sign of heart contraction was detected.
The technique described herein was performed on eight Landrace pigs (four female and four male pigs) aged 2 to 3 months with body weights ranging from 35 to 40 kg. Before the surgical procedure, the animals were fasted for 12 hours with free access to water. The standard protocol of general anesthesia in our center involves intramuscular injection of azaperone (6 mg/kg), ketamine (10 mg/kg), and midazolamine hydrochloride (0.5 mg/kg) 15 minutes before induction of anesthesia. Ketamine (1 mg/kg) and midazolamine hydrochloride (0.1 mg/kg, plus 0.04 mg/kg atropine) were administered intravenously into a dorsal vein in the pig’s ear to induce anesthesia. Endotracheal intubation was performed using an endotracheal tube with an internal diameter of 7.0 mm in the supine position. After endotracheal intubation, 0.75% to 1.5% isoflurane along with 1.5 to 2 L/min oxygen and 0.5 to 1.0 L/min air were used to maintain anesthesia. After a lateral cervical incision and preparation of the carotid sheath, two 16-gauge catheters were inserted into the internal jugular vein and common carotid artery to control the central venous pressure and mean arterial pressure during the operation. The heart rate, mean arterial pressure, central venous pressure, peripheral capillary oxygen saturation, and body temperature (rectal) were monitored continuously.
Similar to the human liver, the porcine liver is divided into five lobes: the left lateral lobe (LLL), left medial lobe (LML), right medial lobe (RML), right lateral lobe (RLL), and caudate lobe. These lobes can be further subdivided into eight segments (I to VIII). The gallbladder adjoins the RML (Figure 1). Porcine liver lobes are divided by deep prominent fissures. Additionally, arterial and portal supplies and venous and biliary drainage are separate in each segment. This makes anatomical resections in pigs almost identical to those in humans. 13 However, the volumes of porcine liver lobes are different from those of human liver lobes. 19 , 20 Another important difference is that the parenchyma of segment I (caudate lobe) covers the vena cava approximately up to the right adrenal gland (Figure 2). Importantly, the parenchyma of segment I should be considered when measuring the remnant liver volume after resection (Figure 2). Moreover, the vena cava passes through the parenchyma of the liver in pigs. Therefore, the liver is not attached to the vena cava in a piggyback position but instead encompasses it completely.

Segmental anatomy of porcine liver in posterior view. Segment I: caudate lobe. Segments II and III: left lateral lobe. Segment IV: left medial lobe. Segments V and VIII: right medial lobe. Segments VI and VII: right lateral lobe.

Ventral view of segment I and inferior vena cava. Segment I encompasses the subhepatic vena cava, cranial to the right adrenal gland.
We performed laparotomy with a long midline incision extending from the xiphoid to the last mammary gland. A long midline incision is less complicated and easier to perform than an L-shaped or chevron incision. In male pigs, the incision was slightly deviated laterally around the penis to prevent injury to the urethra and periurethral vascular plexus. After laparotomy, the liver was mobilized from the falciform ligament (Figure 3(a)) and triangular ligament. Because the liver encompasses the vena cava in pigs, no Makuuchi ligament is present. However, a very thin ligament exists between the posterior side of the liver and the abdominal wall from the suprahepatic vena cava up to the right adrenal gland. It contains several small vessels that should be considered when mobilizing the liver. In the next step, the hepatoduodenal ligament was prepared. The structures of the hepatoduodenal ligament (including the right and left hepatic arteries, portal vein, and common hepatic duct) were dissected and marked with colored loops (Figure 3(b)). To perform the Pringle maneuver, which is suggested for junior surgeons and research fellows, a loop was placed around the hepatoduodenal ligament (white loop in Figure 3(c)). Notably, the cystic duct lies parallel to the common hepatic duct and joins it at the distal third of the hepatoduodenal ligament. Additionally, the liver artery divides into right and left branches at a very proximal location. The cystic artery most often arises very proximal to the right hepatic artery. One to three small branches arise from the left hepatic artery, and these branches supply the stomach. The right hepatic artery may be divided before entering the parenchyma. The artery of the RLL (segment VI/VII) might also arise from the common hepatic artery and ascend to the liver posterior to the portal vein (Figure 4).
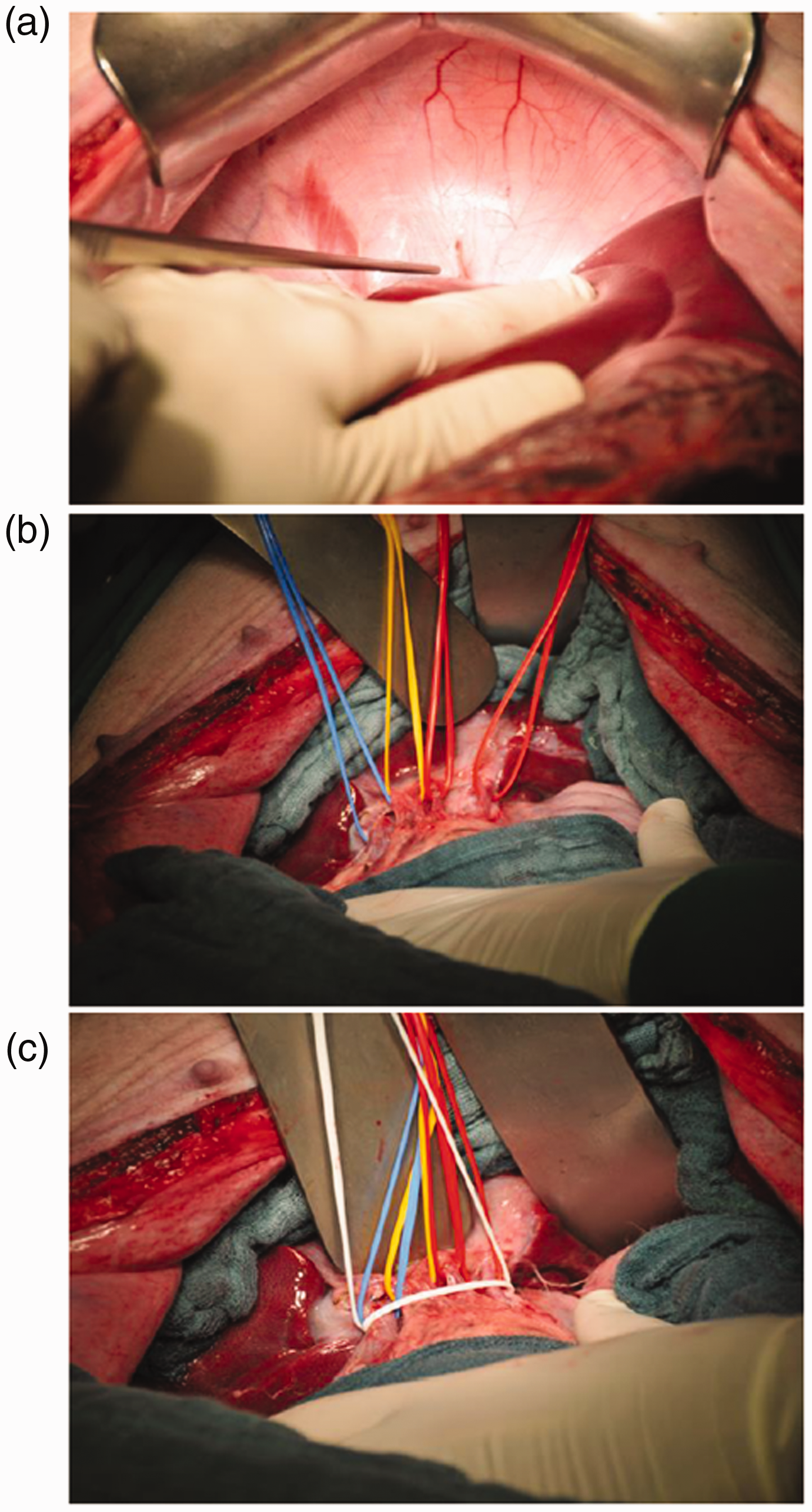
Mobilization of the liver and preparation of the hepatoduodenal ligament. (a) Falciform ligament. (b) Hepatoduodenal ligament: blue loop, portal vein; yellow loop, common bile duct; red loops, right and left hepatic arteries. (c) Pringle maneuver with white loop.
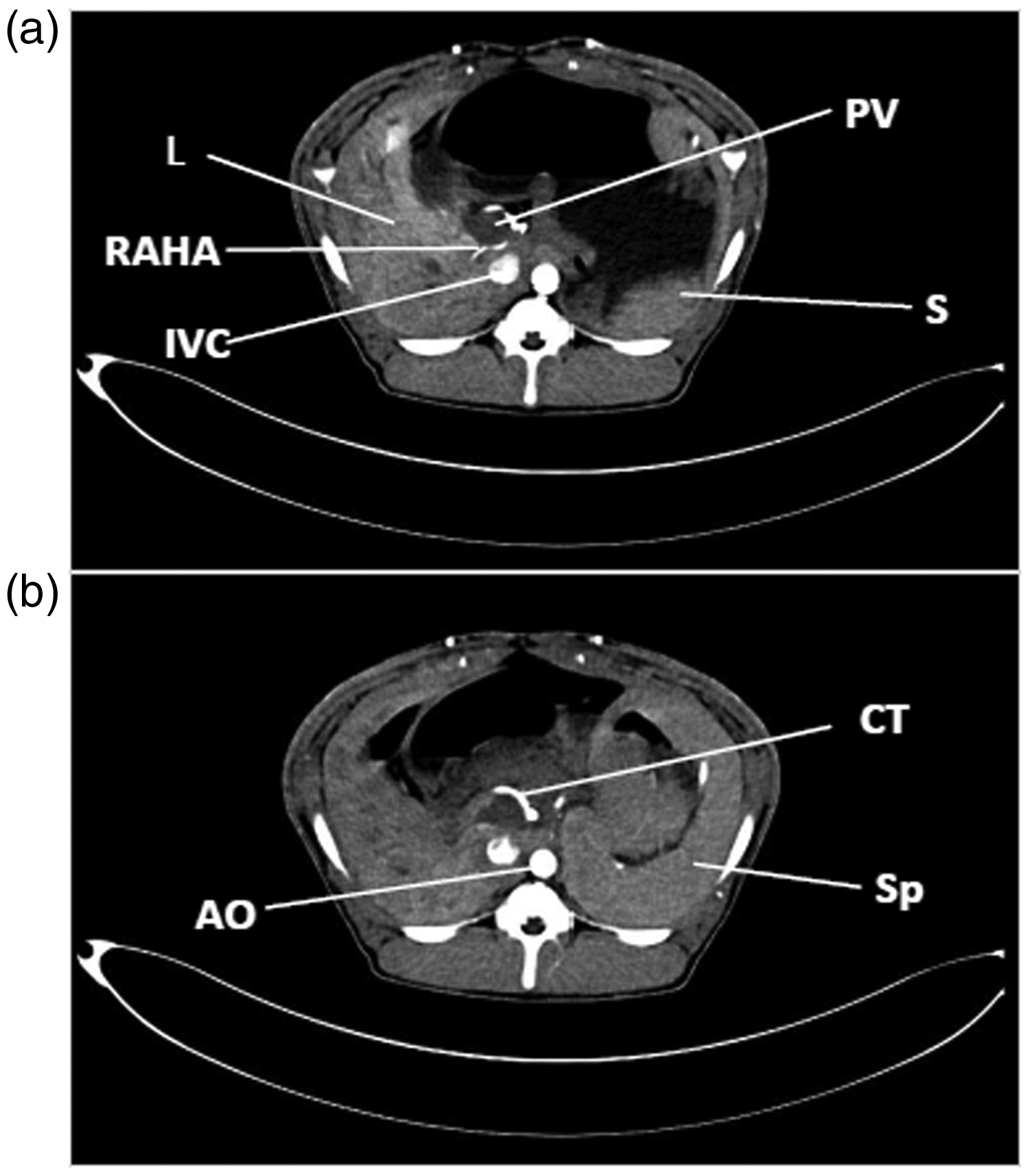
Upper abdominal computed tomography scan of porcine liver with arterial contrast. (a) Right accessory hepatic artery to right lateral lobe (segment VI/VII). (b) Celiac trunk.
To resect the LLL, which consists of segments II and III, we used one 60-mm and one 45-mm surgical stapler (Endo GIA™ Universal Stapler; Covidien/Medtronic, Minneapolis, MN, USA) (Figure 5(a)). The resection plane is illustrated in Figure 5(b). This is the easiest and fastest method for resecting segments II and III. However, because of the deep intersegmental fissure, these segments can be easily resected using any method. The Pringle maneuver is not necessary for this resection. Notably, even with stapler, performing a resection very close to the base of the hepatic vein may cause the vena cava to be open; however, this can be controlled very easily with sutures.

LLL resection. (a) Resection of LLL. (b) RP after resection of LLL.
Left hemihepatectomy can be performed in one or two steps (LLL followed by LML). To perform one-step resection or complete the second step of a stepwise resection, we defined the resection line using a vascular clamp (Figure 6(a)). The LML (segment IV) was resected using two 60-mm and one 45-mm Endo GIA™ staplers (Figure 6(b–e)). The resection surface immediately after resection with a closed Pringle loop is depicted in Figure 6(f). Bleeding from the resection surface was controlled using 3-0 polybutester sutures (Novafil™; Covidien/Medtronic) and bipolar coagulation.

LML resection. (a) Defining the resection line of the LML. (b) Resection of the LML with a stapler. (c–e) Repeating the same procedure for resection of the rest of the LML. (f) Resection plane after resection of LML.
It is preferable to resect the RML separately from the LLL (Figure 7(a) and (b)) because of the porcine liver anatomy and the deep fissure between the LML and RML. Simultaneous resection of the LLL, LML, and RML with a stapler can cause inadequate closure of the resection plane and bleeding. We needed three staplers to resect the RML (one 60-mm and two 45-mm Endo GIA™ staplers). The resection plane must be high enough to avoid opening of the vena cava or injury to the RLL bile duct, which sometimes joins the common hepatic bile duct in a curved fashion way at the base of the RML. As shown in Figure 7(b), the gall bladder was resected en bloc with the RML. Following resection, bleeding was controlled with hand-suturing. The resection plane after opening of the Pringle loop is illustrated in Figure 7(c). To achieve the maximum resection volume for experimental studies, 21 additional resection of the distal part of the RLL (segment VI/VII) is possible (Figure 8(a), (b)). For this purpose, we used one 45-mm and one 60-mm Endo GIA™ stapler. The resection surface is shown in Figure 8(b). After this level of resection, it is important to consider liver edema and possible late bleeding. The resected liver lobes are shown in Figure 9(a) and (b) in the dorsal and enteral view, respectively. The mean parenchymal transection time and operation time were 9.7 ± 1.6 minutes and 50.1 ± 8.1 minutes, respectively.

RML resection. (a) RML with GB. (b) Resection of RML line. (c) Resection plane after completion of hemostasis.

(a) Resection of distal part of right lateral lobe (segment VI/VII). (b) Resection plane after opening of the Pringle loop.

Ventral and dorsal view of the resected liver. From right to left: left lateral lobe (segment II/III), left medial lobe (segment IVa/IVb), right medial lobe (segment VIII/V), and distal part of right lateral lobe (segment VII/VI) of the porcine liver. (a) Ventral view. (b) Dorsal view.
Results
All animals were stable during all steps of liver resection (Figure 10). The mean heart rate was 82 bpm before liver resection and ranged from 81 to 86 bpm during resection. The mean central venous pressure was 7.75 mmHg before liver resection and ranged from 7.12 to 7.75 mmHg during resection. The mean arterial pressure was also stable before and after resection and ranged from 53 to 62 mmHg. The oxygen saturation and body temperature were also monitored during all procedures. The oxygen saturation varied from 91% to 94%, and the body temperature was stable before and after resection (range, 36°C–37°C).
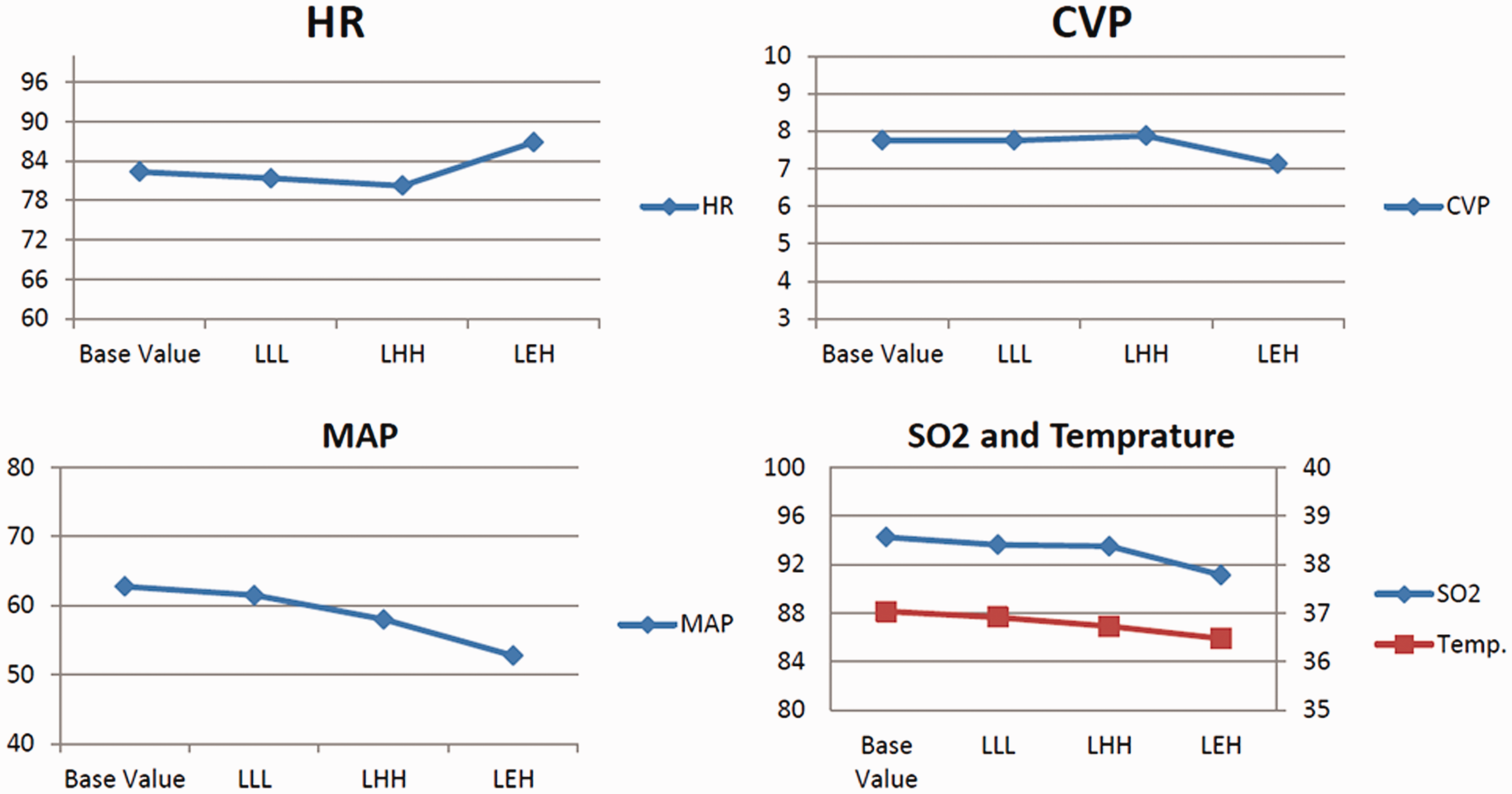
Hemodynamic parameters of the animals during liver resection.
Discussion
New developments in liver surgery have uncovered promising treatments. However, new treatments must be studied and validated in experimental models that simulate the clinical situation. Stapler hepatectomy in porcine models has been previously described in the literature. Zilling et al. 22 presented segmental hepatectomy and left hemihepatectomy 23 in pigs using a stapler technique. In the present study, we have demonstrated a stepwise stapler hepatectomy technique that can be used to perform many types of anatomic liver resection from segmentectomy to EH. Stapler hepatectomy is an easy-to-learn and fast method for this purpose, and it can be learned and performed by junior staff and research fellows. Notably, however, this method is not the optimal resection technique for atypical liver resection in porcine models of cirrhosis. The main disadvantage of stapler hepatectomy is its high cost. Although stapler hepatectomy is an expensive method, it can be rapidly learned and easily performed, omitting the need for experienced surgeons, long operation times, and postoperative complications. These advantages can compensate for the high cost. Additionally, it is possible to combine multiple aims with different resection volumes in one pig through stepwise resection, which can reduce the number of animals used. The establishment of a simple guideline for liver resection can help junior staff and young fellows to perform their experimental studies with low bias.
Footnotes
Authors’ contributions
AMa: Designed the research project, performed the experiments, critically revised the manuscript, approved the final draft
JK: Acquired the data, performed the experiments, approved the final draft
EK: Performed the experiments, drafted the manuscript, approved the final draft
OG: Performed the experiments, drafted the manuscript, approved the final draft
NG: Acquired the data, drafted the manuscript, approved the final draft
PF: Acquired the data, performed the experiments, approved the final draft
SM: Acquired the data, analyzed and interpreted the data, approved the final draft
MA: Acquired the data, analyzed and interpreted the data, approved the final draft
AMe: Designed the research project, critically revised the manuscript, approved the final draft
MG: Designed the research project, performed the experiments, critically revised the manuscript, approved the final draft
Availability of data and materials
The datasets used during the current study are available from the corresponding author on request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.