
Abstract
Objective:
Variation in organ size can occur due to different sonographic scan planes used to make measurements. Diagnostic accuracy may be compromised due to the variations in organ measurement. Therefore, the aim of this study was to compare sonographic measurements and actual organ measurements, taken predissection and postdissection, to determine the accuracy of sonographic measurements, taken in various sonographic scan planes.
Materials and Methods:
Sonographic organ measurements were made of the liver, kidney, and spleen, prior to cadaver dissection. Liver length measurements were acquired in the midclavicular and intercostal sonographic scan planes. All kidney length, height, and width measurements were acquired scanning from the anterior and coronal planes. Spleen measurements were acquired using an intercostal sonographic scan plane, using longest dimension for length, and acquiring transverse measurements from both a 90-degree and a 180-degree transducer rotation. Descriptive statistics were reported using mean, standard deviation, median, and interquartile range.
Results:
Liver length, spleen length, right kidney length and width, and left kidney width showed no measurement differences. Sonographic measurements of right kidney height varied (p < .0001). The sonographic left kidney length was more accurate when acquired in the coronal plane (p = .006), and the height measurement was more accurate taken from the anterior plane (p < .001). Spleen width varied between the 90-degree and 180-degree transducer rotation, and postdissection measures (p = .0010).
Conclusion:
This pilot study would suggest that there is a need for the development of standardized sonographic organ measurement protocols.
Sonography is often the first diagnostic imaging technique used to evaluate abdominal and retroperitoneal organs, primarily because it is more accessible, noninvasive, and lower cost when compared with other diagnostic imaging choices. Physicians use 2D sonographic measurements to make clinical decisions, regarding normality or abnormality of an organ. Because sonography is operator dependent, there can be wide variation in organ size, due to the measurement techniques and the associated imaging planes. This variability may lead to uncertainty in diagnosis, and alternate imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI), which are sometimes preferred because they offer more consistency in imaging and measuring techniques. Additional imaging can increase health care costs and may not be as readily available. Standardizing the protocol for making sonographic measurements, for each organ, could improve the diagnostic accuracy of sonography and increase its diagnostic reliability.
There are standards and guidelines for practice set forth by various accrediting organizations, including the American Institute of Ultrasound in Medicine (AIUM), Society of Radiologists in Ultrasound, and American College of Radiology (ACR), and the Society for Vascular Ultrasound.1 –3 These documents relate to the practice of sonography in general but are not prescriptive on what sonographic scan planes should be used to acquire measurements. The American Society of Echocardiography provides specific guidance on sonographic scan planes, acoustic window, and electronic caliper placement, to properly measure cardiac structures. 4 There are many accepted sonographic scan planes that can be used to measure the liver, kidneys, and spleen. Normal values can vary based on which scanning plane is chosen to image the organ and acquire measurements, and limited evidence was found that related to measurement accuracy variance due to sonographic scan planes.5 –9
The adult right lobe liver length is used when evaluating for hepatic diseases and the length can vary over time in size, shape, and texture. 6 Normal liver length ranges from 13 to 15.5 cm and varies based on if the midclavicular scan plane, or the intercostal scan plane that is used to capture a long axis image. In some cases, up to 17 cm in length is normal.7,8 Sonography demonstrates high specificity and positive predictive value in assessment of liver diseases and is often used in screening patients with abnormal lab values. 10 Although liver length may screen for liver diseases with good accuracy, liver length measurement varies based on which sonographic scan planes are chosen by the operator. This variation creates difficultly in observing gradual or subtle changes in organ size, especially when following a patient’s condition over time. Though Kawamura and Nolan, 7 and DeJong 8 recommend a midclavicular approach for making organ measurements, clinically an intercostal approach is often used.
Kidney size, which varies based on patient age, body surface area, gender, hydration status, and side, is an important clinical factor in the diagnosis and treatment of renal diseases.11,12 Normal values for adult kidneys range from 9 to 12 cm in length, while width and height are more variable.6,8,12 Braconnier et al 13 reported that sonographic kidney length measurements correlate well with MRI measurements. Some research demonstrates a good correlation between kidney function and volume, calculated by taking kidney length, width, and height measurements and indexing with patient body-surface area. 11 Bakker et al 14 criticized sonographic kidney volume measurements finding that kidney volume formula may underestimate kidney volume. This can be attributed due to the standard ellipsoid volume calculation, used in sonography, which does not apply to kidneys that are not ellipsoid shaped. Reduced kidney size can indicate chronic kidney disease, and in patients with kidney transplants, decreased graft size is suggestive of low glomerular filtration rates.15,16 Increased kidney size can correlate with injury, cystic disease, or urinary obstruction.12,17 –19 Obtaining accurate sonographic kidney measurements is vital for clinical decision-making.
The spleen is an irregularly shaped organ located in the left upper quadrant and is most often imaged in conjunction with examinations of other abdominal organs. Average splenic size is 12–13 cm in length, while width and height are less standard measurements to acquire with sonography.6,9 Spleen echogenicity is compared with the left kidney to establish kidney normalcy.7,8 Though the spleen is rarely the primary location for disease, due to its major involvement in the immune system, it is often affected by inflammation and infection. 6 Injury to the spleen is also common in blunt force trauma, and diagnostic imaging may be needed to clarify location of injury and splenic function. 20 Splenomegaly can be seen when the spleen measures greater than 13 cm, although, due to irregular shape of the organ, upper limits of normal are only roughly established.7,8
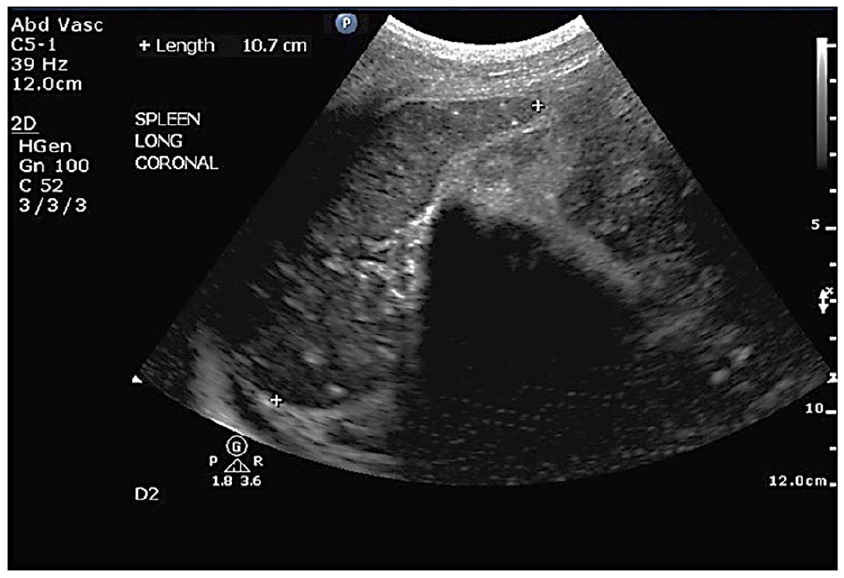
CT and MRI are diagnostic gold standard for evaluating splenic volume, but sonography allows for more efficient and portable use. 5 The spleen is imaged with sonography by placing the transducer intercostally, with the long axis aligning with the ribs. Turning the transducer 90-degrees shows a transverse orientation, where width and height should be measured, as recommended by Kawamura and Nolan 7 In clinical practice, many ultrasonographers rotate the transducer 180-degrees and refer to that as the transverse sonographic scan plane 7 (See Figure 1). This practice creates a disparity in organ width measurements. Though a true transverse sonographic scan plane may have rib shadowing and diminished image quality, the organ measurements acquired would provide better accuracy, when evaluating splenic volume. Establishing an assessment method that produces reliable splenic measurements could be an important development for the use of sonographic evaluation of the spleen.
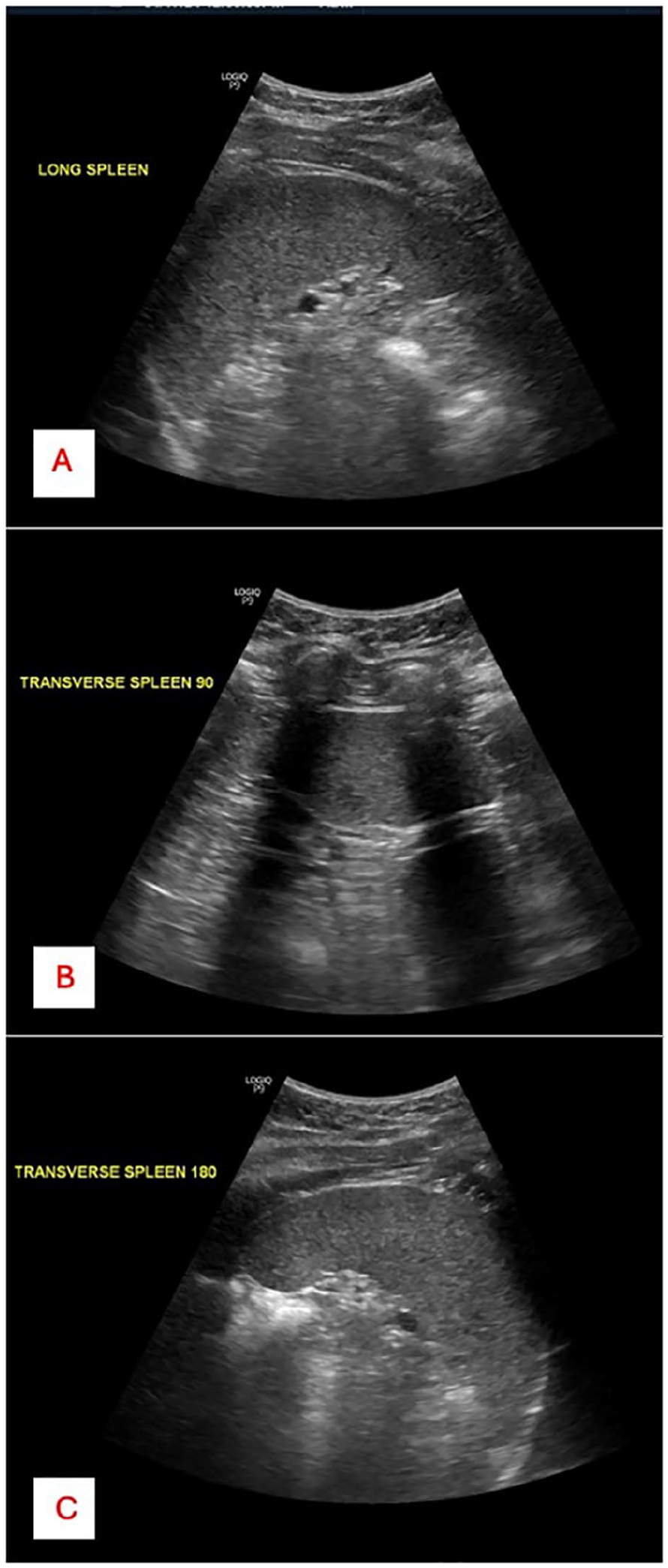
(A) An example of a normal spleen imaged in the longitudinal sonographic scan plane. (B) An example of a normal spleen imaged in a true transverse sonographic scan plane, acquired by rotating the transducer 90-degrees. (C) An example of a normal spleen imaged in the transverse sonographic scan plane, based on a 180-degree transducer rotation.
Since sonographic measured organ size could contribute to a pathological diagnosis, it is important for the ultrasonographer to use evidence-based measurement techniques. Overestimation, or underestimation of size potentially can lead to misdiagnosis. The purpose of this research was to determine which sonographic scan planes were most accurate for the purpose of measuring the liver, kidneys, and spleen, compared with actual organ measurements from cadaver specimens.
Materials and Methods
The purpose of this study was to compare predissection organ measurements acquired from sonograms using different sonographic scan planes to actual organ measurements taken postdissection on cadaver specimens. This would allow for determining which sonographic scan planes yielded measurements that most closely replicated actual organ size. An institutional review board, in conjunction with the university willed body program, and the state anatomical board granted approval for the research on cadaveric specimens.
The research took place in a university undergraduate cadaver anatomy laboratory course that was cataloged for undergraduate general education. Cadavers were provided through the University’s anatomical donation program. Sixteen cadaveric specimens were available for this study. To protect the anonymity of the donors, the laboratory faculty and staff were not provided with patient identity, medical history, height, or weight. Gender and age were the only demographic details provided. Each cadaver was assigned a subject number for consistent, repeatable data collection.
A CX50 ultrasound equipment system (Philips Healthcare, Andover, MA, USA) with a curvilinear 1–5 MHz transducer was used for predissection imaging. The equipment settings were altered as needed to provide the best image resolution. All of the sonographic data collection was completed over two separate days. Equipment system calibration and quality control was done before each imaging session to ensure machine accuracy. Sonographic images of the liver were acquired in the midclavicular and intercostal scan planes, kidneys were measured in the anterior and coronal scan planes, and splenic measures were taken from the intercostal scan plane, prior to the dissection of the abdomen and retroperitoneum. Transducer pressure was used as needed to obtain optimal sonographic images, to mimic a diagnostic sonogram.
Predissection Sonographic Measurements
The right liver was imaged from two sonographic scan planes and the length measurement acquired. The dome of the liver served as the most superior landmark, and the most inferior tip of the right lobe served as the inferior landmark. In the midclavicular approach, the transducer was positioned subcostally and aligned to show the right kidney posterior to the liver, whenever possible. For the intercostal approach, the transducer was positioned slightly posteriorly and obliquely from the coronal side of the right ribcage to allow visualization through the intercostal spaces. In both measurement techniques, electronic calipers were placed from the most inferior tip of the right lobe of the liver, to the border of the diaphragm at the greatest distance, in an anteroposterior sonographic scan plane (See Figure 2).
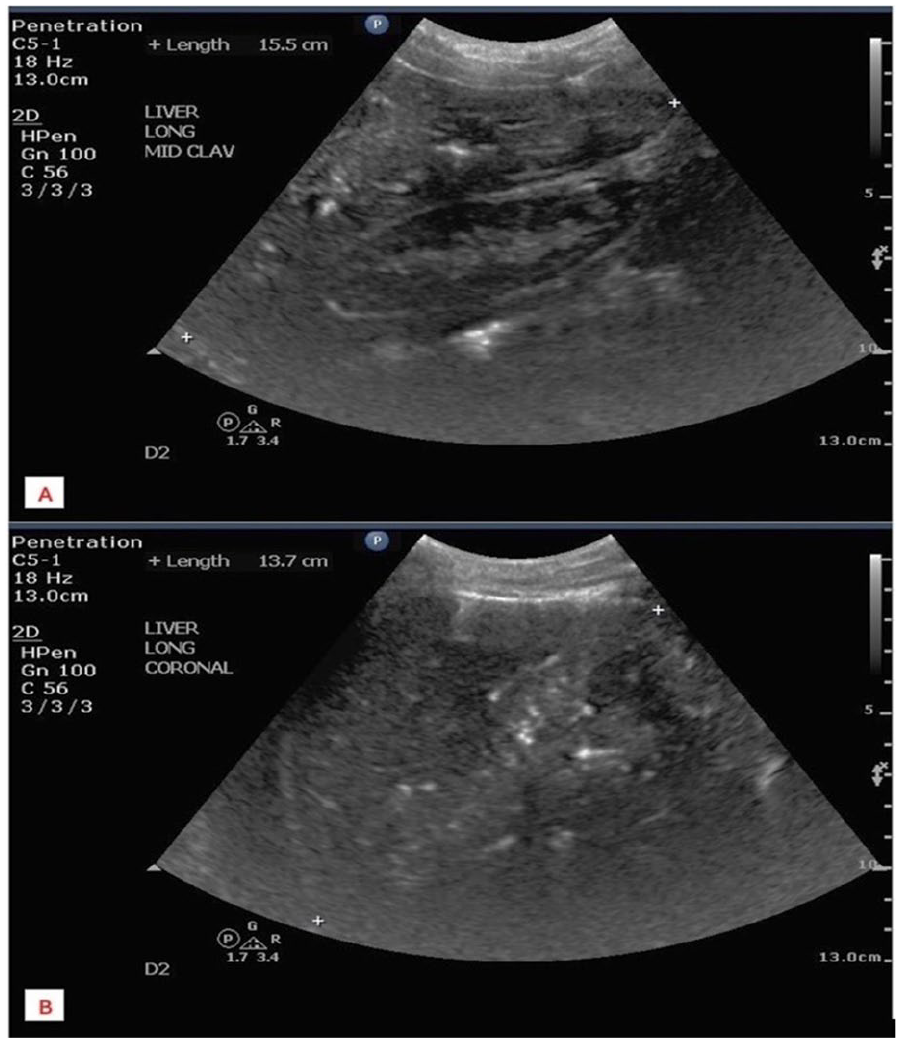
(A) An example of liver length measured on a sonogram created from a midclavicular scanning approach. (B) An example of liver length measured on a sonogram created from an intercostal scanning approach.
Both kidneys were evaluated from the anterior/midclavicular and coronal sonographic scan planes. Measurements were acquired for organ length, width, and height. In the anterior/midclavicular sonographic scan plane, the kidney was imaged from the anterior side of the abdominal wall, inferior to the ribs. For the coronal scan plane, the kidney was imaged from the lateral aspect of the abdominal wall, inferior to the ribs. The transducer angle was adjusted to demonstrate the kidneys in their longest dimension. To acquire kidney length, electronic calipers were placed from organ border to border, at the longest dimension of the kidney (See Figure 3). To acquire kidney height and width, the transducer was rotated 90-degrees counterclockwise from the longest dimension. Measurements were taken midkidney at the level of the hilum, where the renal vessels could be seen entering the kidney. The width was measured from midhilum to the lateral aspect of the kidney and the height was measured perpendicular to width in an anteroposterior sonographic scan plane (See Figure 4).
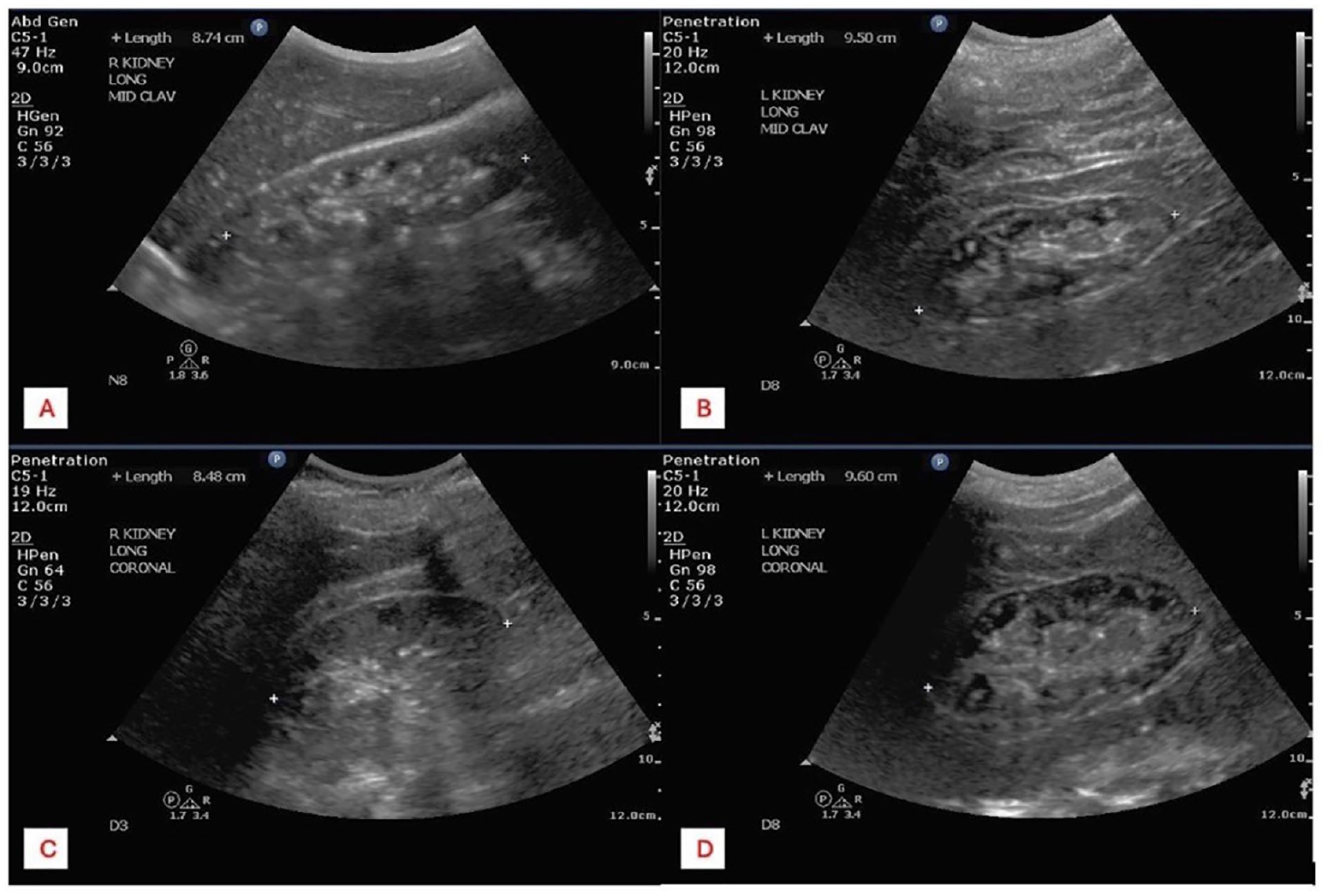
(A) An example of a right kidney length measured on a sonogram, created from an anterior scanning approach. (B) An example of a left kidney length measured on a sonogram, created from an anterior scanning approach. (C) Another example of a right kidney length measured on a sonogram, created from a coronal scanning approach. (D) Another example of left kidney length measured on a sonogram, created from a coronal scanning approach.
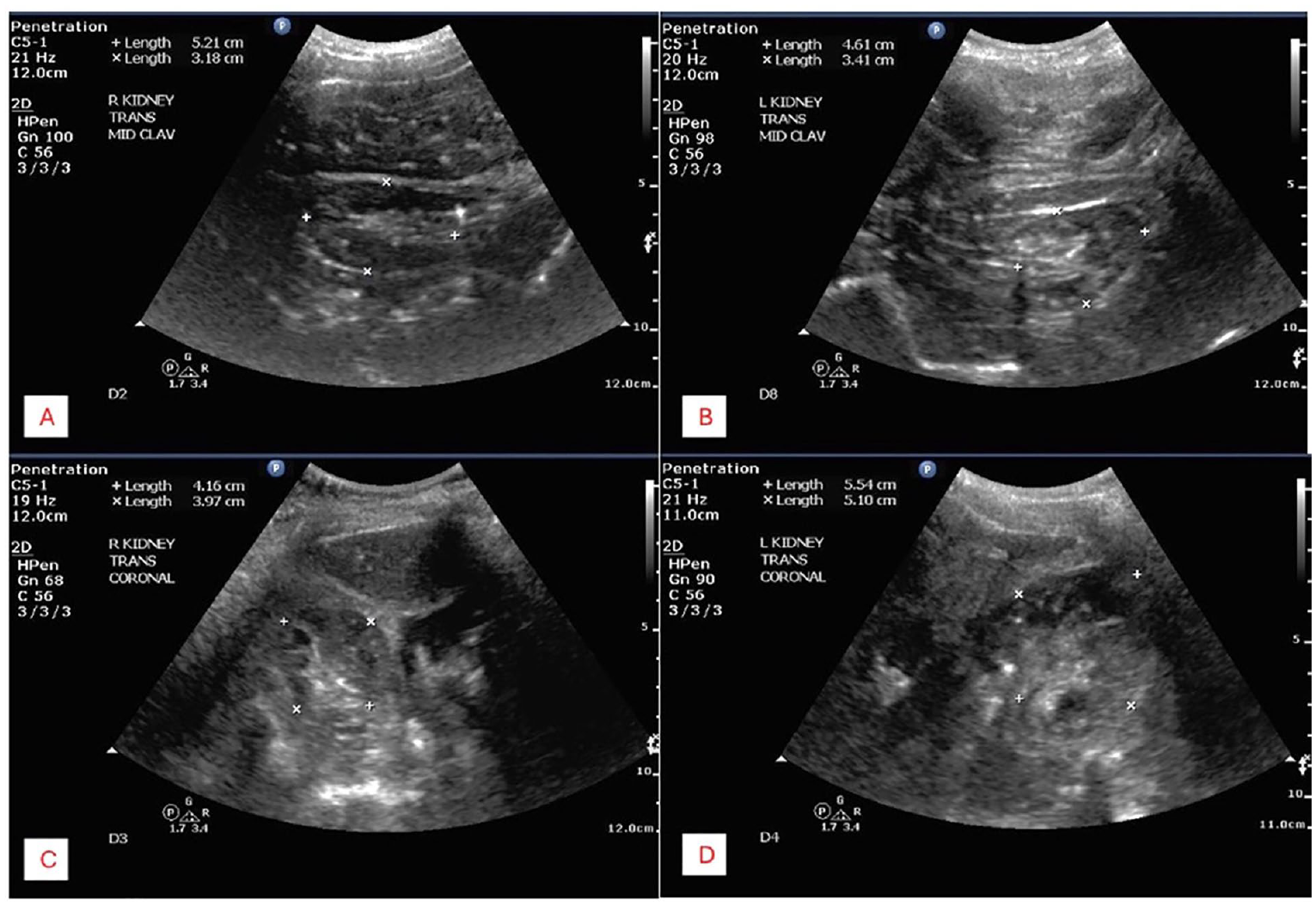
(A) An example of a right kidney measured transversely, on a sonogram, created from an anterior scanning approach. (B) An example of a left kidney measured transversely, on a sonogram, created from an anterior scanning approach. (C) Another example of right kidney measured transversely, on a sonogram, created from a coronal scanning approach. (D) Another example of left kidney measured transversely, on a sonogram, created from a coronal scanning approach.
The spleen was imaged from a coronal left intercostal sonographic scan plane, with the transducer angled oblique and slightly posterior, which allowed for imaging between the ribs. Spleen length was measured at the longest dimension of the organ with the electronic calipers placed from the inferolateral end to the superior-medial end (See Figure 5). The splenic width measurement was taken in a true transverse sonographic scan plane, rotating 90-degrees counterclockwise from the longitudinal scan plane. Additional width measurements were taken in the commonly accepted 180-degree counterclockwise rotation from the longitudinal sonographic scan plane. For both techniques, the electronic calipers were placed at the widest dimension from lateral border to medial border (See Figure 6).
An example of splenic length measured on a sonogram, created with a coronal scanning approach.
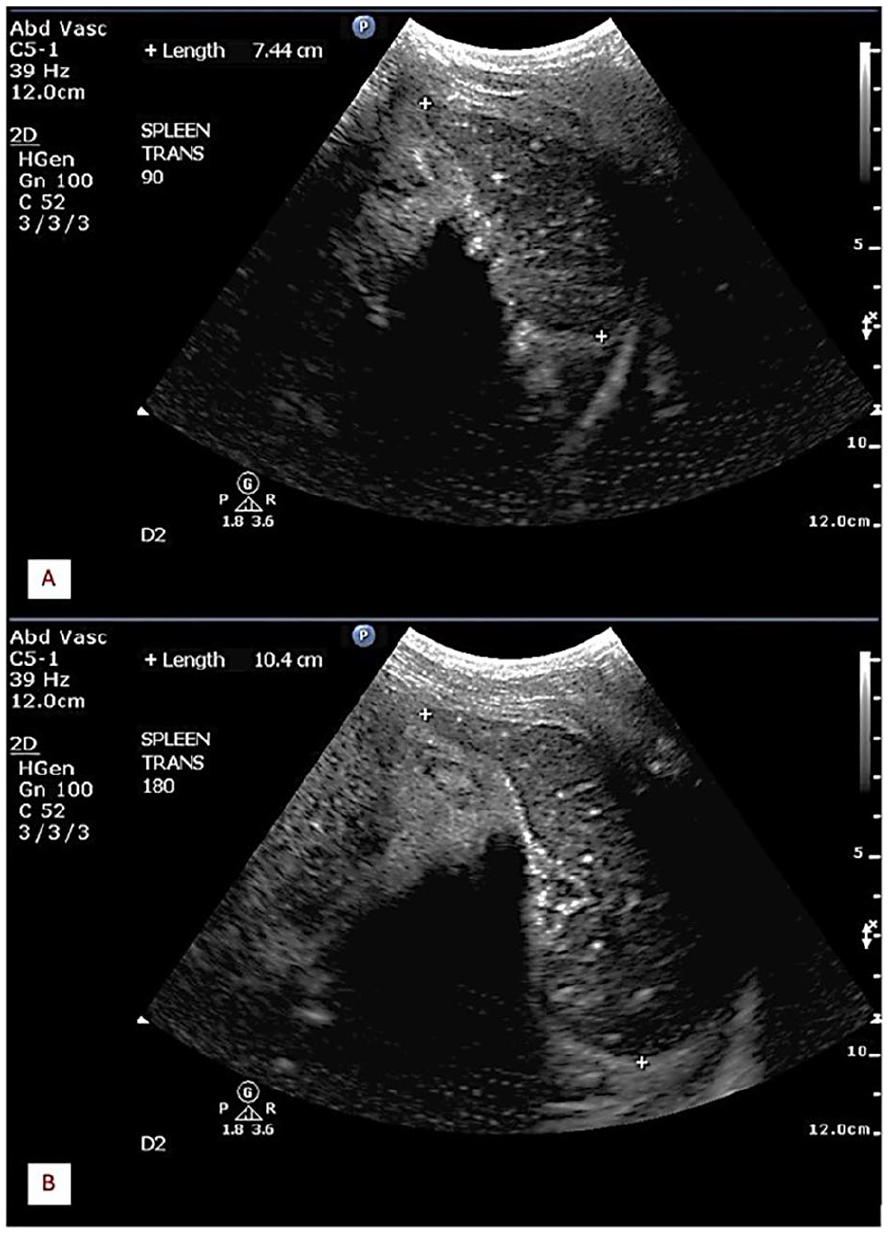
(A) An example of spleen width, measured on a sonogram, created with a 90-degree transducer rotation. (B) Another example of spleen width, measured on a sonogram, created with a 180-degree transducer rotation.
Postdissection Organ Measurements
Postdissection organ measurements were acquired after the cadavers had been fully dissected. A contour measurement of the organ shape was acquired with a contour gauge in each scan plane separately, and once achieved, the distance from the top displaced marker to the bottom displaced marker was measured using a ruler for linear dimension. The use of a contour gauge allowed for linear dimensions to be derived from curved structures. Liver length was assessed in-situ to the cadaver. The contour gauge was placed on top of the right lobe of the liver and pressed down to evaluate the shape of the organ from superior margin to inferior margin. Kidney and spleen measurements were assessed with the organs outside of the abdominal cavity. Each kidney was placed on a flat surface, and the contour gauge was placed around each kidney to achieve the measurements, in all three scan planes at their largest dimensions. The spleen was measured at its longest dimension and perpendicular to that for width.
Ultrasonographer Qualifications
For standardization across the study, one researcher, a sonography student, in the last year of sonography training, performed all predissection sonograms and sonographic organ measurements, as well as the postdissection organ measurements. The student had achieved all required abdominal scanning competencies and was deemed competent to perform sonographic measurements. The student ultrasonographer also had 2-year experience employed in the university laboratory as a dissection specialist and was considered competent and qualified to dissect and handle cadaver specimens.
Cadaver Management
The cadavers used in this study were preserved with Embalming Fluid Maryland, which includes methanol, formaldehyde, and phenol. The cadavers arrived in the anatomy labs as frozen specimens and were thawed prior to dissection. They were maintained in body bags, specially designated for cadaver specimens. At the end of each dissection session, cadavers were covered in cotton towels that were sprayed with Nebanol Working Solution, which includes water, propylene glycol, and phenoxyethanol, to prevent drying. The study cadavers were kept in their preservation bags between laboratory sections. Dissection was completed based on body regions and occurred over a 16-week semester, with the abdominal and retroperitoneal cavities being dissected in the latter half of the semester. At the time that the sonographic measurements were obtained, the anterior abdominal wall had been dissected, but the abdominal fascia, peritoneum, and retroperitoneum had not been breached. The ultrasonographer carefully placed the abdominal wall skin in the proper anatomic orientation to conduct sonographic measurements. For postdissection measurements, the ultrasonographer inspected organs to ensure that they were intact, and when needed, was able to dissect extra tissues from the organs to ensure that only the organs were measured, postdissection.
Statistical Analysis
Statistical analysis was used to evaluate sonographic organ measurement accuracy compared with the postdissection measurements. Descriptive statistics were reported using means, standard deviation, medians, and interquartile range (IQR). All descriptive statistics were organized by organ and sonographic scan planes. Tests included, paired t test or repeated-measures analysis of variance (ANOVA), sign rank, or Friedman’s tests. Normality among all measures was tested using Shapiro-Wilk tests, histograms, and QQ plots. If normality assumptions were confirmed, then either a paired t test or repeated-measures ANOVA was used to test differences among the postdissection measure and the sonographic organ measures. If normality assumptions failed, then differences were assessed using sign rank tests or Friedman’s tests. Statistical significance was set at p < .05, a priori.
Results
Sixteen adult cadavers were evaluated at the onset of the study. Conducting sonography with three of the cadavers was not possible, due to their large body habitus. Three additional cadavers were removed from the cadaver laboratory, in the middle of the semester, due to issues with cadaveric preservation. The resulting study sample included ten cadavers; however, the measurements that could be obtained from each cadaver varied. The age of the 10 cadaveric subjects ranged from 62 to 92. Four cadaveric subjects were women and six were men.
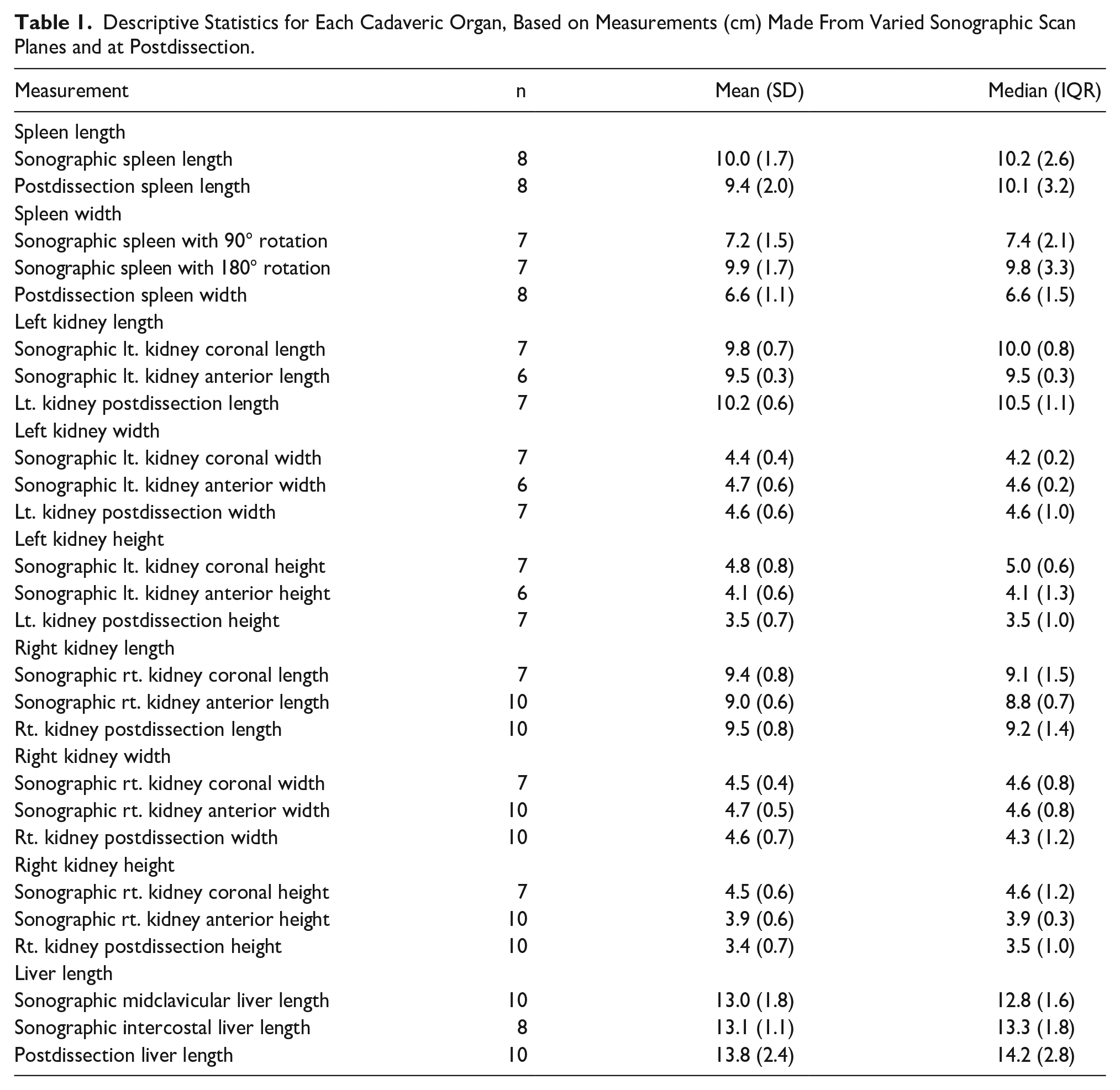
Unpaired cadaveric data had to be dropped before the analysis. This resulted in a reduction of the sample size for the splenic evaluation, to seven subjects. The left kidney coronal sonographic scan plane was based on seven cadavers while left kidney anterior scan plane measurements were collected from six cadavers. The right kidney coronal sonographic scan planes were based on seven cadavers in the analysis, while the right kidney anterior scan plane included ten cadavers. The midclavicular liver length measurements were taken from ten cadavers and the liver intercostal organ length measurements were based on eight cadavers. The specific sample size for each measurement taken, the descriptive statistics, and normality test results are listed (See Table 1). Table 2 shows the means of each measurement method, test used to analyze, test statistic, and p values for each organ and imaging plane.
Descriptive Statistics for Each Cadaveric Organ, Based on Measurements (cm) Made From Varied Sonographic Scan Planes and at Postdissection.
Statistical Methodology and Analytical Results, for Each Cadaveric Organ, Based on Varied Sonographic Scan Planes and at Postdissection.
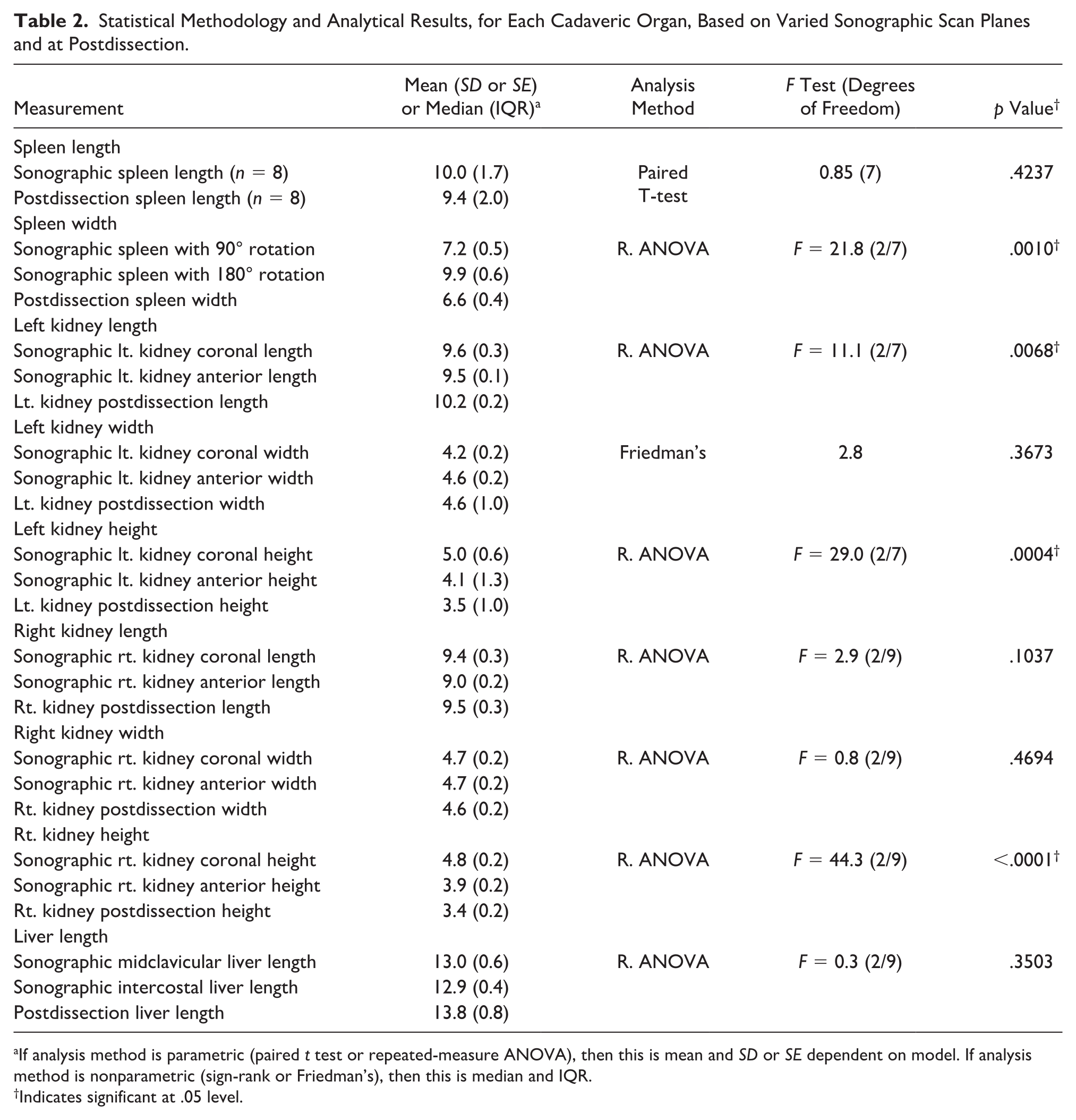
If analysis method is parametric (paired t test or repeated-measure ANOVA), then this is mean and SD or SE dependent on model. If analysis method is nonparametric (sign-rank or Friedman’s), then this is median and IQR.
Indicates significant at .05 level.
Organ length was the only measurement assessed on the liver. Intercostal and midclavicular planes were used and compared with postdissection organ measurements. Both intercostal and midclavicular sonographic scan planes, for liver length, revealed no statistical difference, based on postdissection liver length (p = .3503).
The right kidney measurements showed no statistical difference in length or width measurements (p = .1037 and p = 0.4694, respectively) between sonographic and postdissection measurements. All measurements for sonographically derived right kidney height varied from each other (p < .0001). The right kidney sonographically derived coronal height was 0.9 cm (95% CI: 0.6, 1.2), which was larger than the sonographically derived anterior height measures. Both the coronal and anterior sonographic scan planes overestimated the postdissection right kidney height measurement by 1.4 cm (95% CI: 1.0, 1.8) and 0.53 cm (95% CI: 0.1, 1.0), respectively (p = .0263).
Sonographic measurements of the left kidney length and height differed from postdissection measures. Left kidney length from the coronal sonographic scan plane did not differ from postdissection measures (p = .1769), with a point estimate difference of 0.6 cm (95% CI: -1.5, 0.3) (See Figure 7). From the anterior sonographic scan plane, the left kidney length was 0.8 cm (95% CI: 0.17, 1.4) smaller than postdissection left kidney measurements. However, left kidney height measurements were the opposite, showing better accuracy and no statistical difference from the anterior approach (p = .2312) with an observed point estimate difference of 0.5 cm (95% CI: –0.4, 1.3) (See Figure 8). Left kidney coronal sonographic scan plane height showed a difference of 1.3 cm (95% CI: 0.8, 1.8) larger than postdissection left kidney height (p = .0006). There was not a difference between sonographically measured left kidney width and postdissection left kidney width (p = .3673).
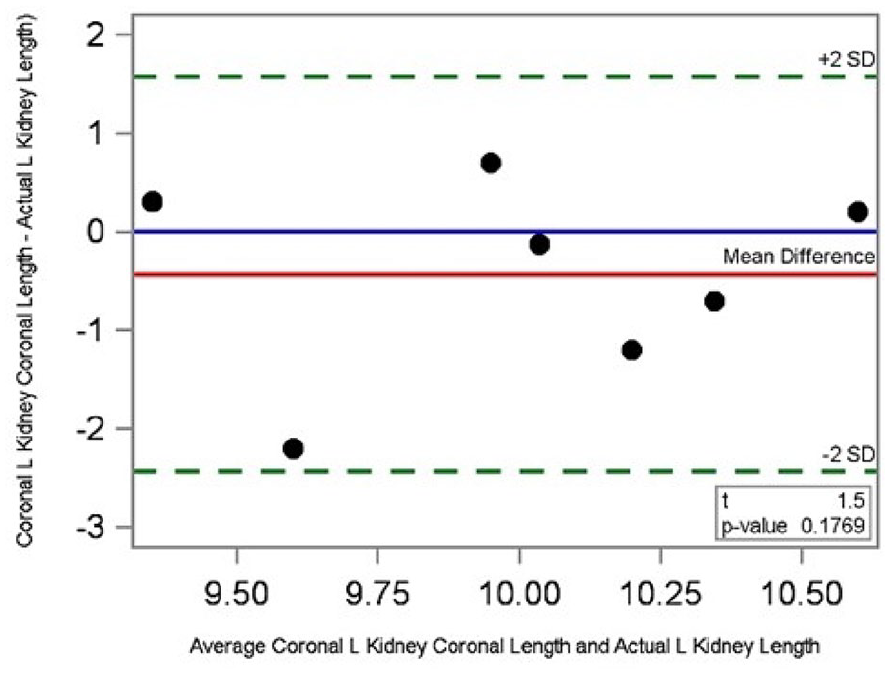
A Bland-Altman analysis that demonstrates agreement between the left kidney length measurements made in the coronal sonographic scan plane and at postdissection.
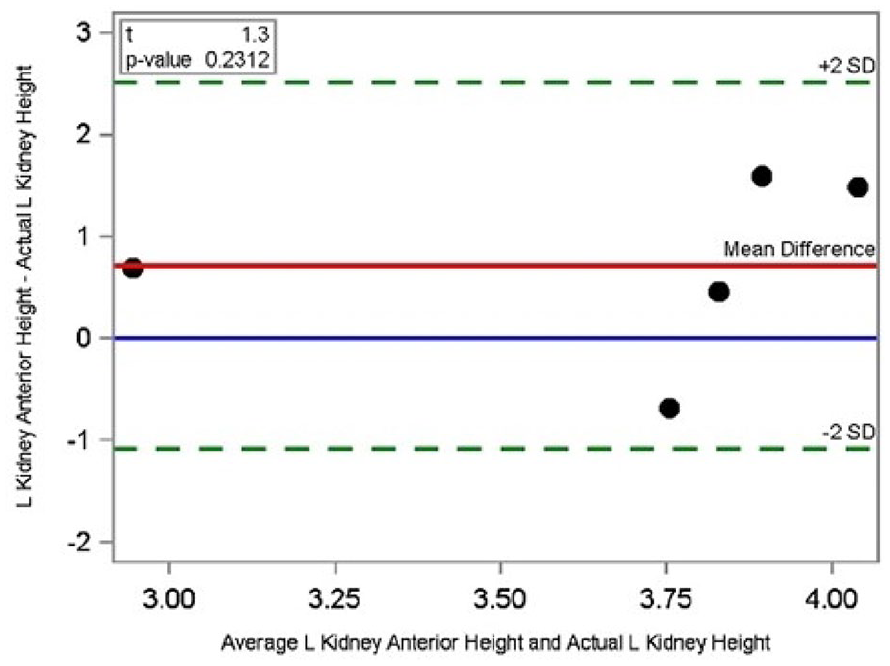
A Bland-Altman analysis that demonstrates agreement between the left kidney height measurements made in the anterior sonographic scanning approach and at postdissection.
Spleen length showed no statistical difference between measurements (p = .4237); however, there was a difference in sonographically measured spleen width and postdissection spleen width (p = .0010). The sonographic width measured at a 90-degree rotation from spleen length showed no significant difference from postdissection spleen width (p = .0539), with an observed point estimate difference of 0.6 cm (95% CI: –0.01, 1.3) (See Figure 9). When measured by rotating the transducer 180 degrees, the measurement averaged 2.7 cm (95% CI: 1.7, 3.7) larger than the 90-degree rotation measurement, and 3.3 cm (95% CI: 2.1, 4.5) larger than postdissection spleen width. When compared with postdissection spleen length, the 180-degree rotation length measurement showed no significant difference (p = .5449).
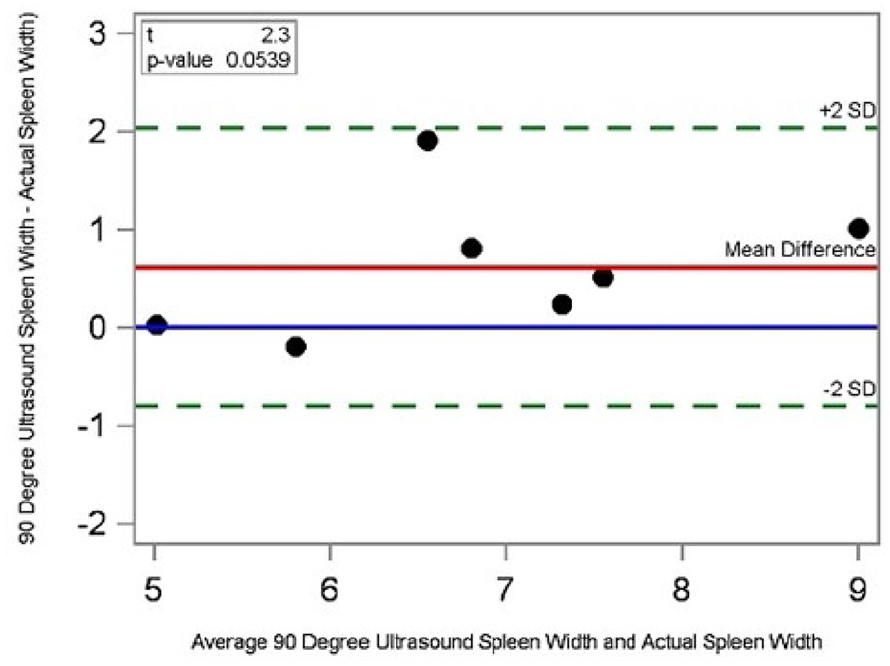
A Bland-Altman analysis demonstrates agreement between spleen width measurements made on a sonogram, created with a 90-degree ultrasound transducer rotation and at postdissection.
Discussion
This pilot study assessed the accuracy and adequacy of various sonographic scan planes and their resulting measurements. Liver length, kidney length, kidney width, kidney height, spleen length and spleen width were all evaluated from standard sonographic scan planes. The results would suggest the need for standardized sonographic organ measurement protocols.
Regarding liver length, both the intercostal and midclavicular approaches showed good correlation with the postdissection liver length, supported by either sonographic scan plane, as an adequate assessment. For liver measurement in this study, electronic calipers were placed from the inferior margin of the right lobe of the liver to the superior diaphragmatic border at the greatest distance, in an anteroposterior plane, as demonstrated in DeJong’s measurement protocols. 8 Varied electronic caliper placement, to assess liver length, was another topic of research that was outside the scope of this study. Riestra-Candelaria et al 6 have previously evaluated the accuracy of electronic caliper placement and found that measurements in a cranio-caudal scan plane, parallel to the anterior surface of the liver, provided more accurate values. However, this accuracy is limited by patient body habitus and, in the case of this study, by the stiffness of the cadaver tissues and inability to use respiration for assistance.
The results of this study demonstrated good correlation for sonographically derived right kidney length and width from either the anterior or coronal sonographic scan planes. Therefore, operators could feel comfortable using whichever scan plane gives the best acoustic window. However, sonographically derived right kidney height showed variation. The right kidney height measured from an anterior scan plane was closer to the postdissection measurements, overestimating the postdissection measurement by 0.5 cm, while the coronal sonographic scan plane overestimated the postdissection, by nearly 1.5 cm. This variation may suggest that an anterior sonographic scan plane may be considered more accurate. It is unclear whether the liver as an acoustic window could have affected these measurements, but more evidence is needed to evaluate why there was so much variation in this sonographic scan plane.
The left kidney showed more variations in measurement accuracy than the right. The sonographically derived length measurement better matched postdissection measurements when taken from a coronal sonographic scan plane while the anterior scan plane underestimated the length. Left kidney height showed the opposite result and was more accurate from the anterior sonographic scan plane. The coronal scan plane overestimated the height measurement by approximately 1.5 cm, which potentially could be the difference between a normal versus abnormal measurement. The left kidney width showed good correlation with postdissection measurements from both sonographic scan planes.
Both kidneys sonographically derived measurements showed better accuracy for height from an anterior sonographic scan plane. This accuracy could be attributed to better axial resolution within the ultrasound beam, allowing for clearer borders in the anteroposterior scan plane that height. Standard three sonographic scan plane measurement techniques were used to place the electronic calipers for kidney assessment. This required that one sonographic measurement be taken in the longitudinal scan plane and two in the transverse sonographic scan plane. Further research could evaluate whether height taken in the same scan plane as the length, or in the transverse scan plane with the width, yielded more accurate organ height measurements.
The most significant results in the study related to the measurements of the spleen. Splenic length had good correlation with the postdissection measurements when taken from a left intercostal sonographic scan plane, with the longest distance measured. Splenic width showed large variation between the two transducer rotation techniques. A commonly used technique to measure the splenic width in the clinical environment, is a 180-degree rotation from the long scan plane, as this helps remove rib shadowing and demonstrates more splenic tissue. Typical sonographic references highlight this view as a transverse representation of the spleen, ignoring that it is a full 180-degree turn and not a standard 90-degree rotation to reach a transverse scan plane.7,8 When measured at this 180-degree rotation, the spleen width was overestimated by 3.3 cm compared with the postdissection width. The length measurement with the 180-degree rotation showed no statistical difference from the postdissection splenic length, supporting the hypothesis that a 180-degree rotation is an inverse image of the longitudinal spleen. When employing a 90-degree rotation, the measurements showed no difference from postdissection splenic width.
These results provide evidence that a change may be needed in the standard splenic protocol for evaluations based on a longitudinal and true transverse sonographic scan plane. Without making these adjustments, an accurate splenic volume may not be obtained, and size could be overestimated leading to inaccurate assessment of normality. The shape of the spleen seems to be incorrectly assessed as a symmetrical ellipsoid, while the postdissection cadaveric shape is more ovoid or oblong and nonsymmetrical. This assumption could contribute to the general acceptance of a 180-degree turn, as an accurate view of splenic width.
Impact on Clinical Practice
Michel et al 21 noted that in pediatric sonography, the kidney dimensions varied based on patient position and sonographic scan plane. The AIUM and ACR practice parameters do not specify scan planes for acquiring liver, kidney, or spleen imaging, but suggest that length measurements can aid in diagnosing enlargement.1,2 Both professional organizations specify that kidney length should be measured, and any scan plane that is recommended.1,2 As sonography becomes the primary imaging technique for the abdomen and retroperitoneum, professional organizations may look at improving consistency of results across their accredited practices. By establishing more controlled measurement standards, variation in organ measurements could be minimized and allow for improved assessment, particularly when repeated over time with different operators. In turn, sonography practices may need to evaluate their measurement protocols to determine whether they are providing accurate data to assist in making the diagnoses, for their patients.
The literature on cadaver research is scarce, with only a few studies published in the last 10 years. Ristela-Candelaria et al 6 have the most current study with a sample size of 21 cadaver subjects, which was larger than the current study. Like the current study, their specimens had oversight from an anatomical donation program. 6 However, their methods were different because they focused on liver measurements only and additionally looked at the liver in the midaxillary imaging plane, in which the current study did not consider. 6 Beige et al 22 studied kidney volume on 13 cadaver kidneys that were part of an anatomical donation program. Their primary aim was to study sonographically derived kidney volume compared with actual volume as measured by water displacement, however, they did take sonographic length, width, and height organ measurements. 22 They found good correlation of sonographic length with actual measurements. 22 However, the researchers used one imaging plane and did not specify which plane was used, contrasting with this study that used both the anterior and coronal imaging planes. 22 In addition, their focus was on volume rather than the three linear measurements used in this study. 22
An important distinction should be made for those cadaver studies that used deceased patients, scheduled for autopsy, rather than anatomical donation. Such research is not as regulated by anatomical donation programs, which have strict regulations on cadaver handling. Loftus et al 23 studied 47 spleens on deceased persons scheduled for autopsy. Their research found that splenic length by sonography was comparable with the actual measurement, as was reported in this study. 23 Partik et al 24 studied kidney volume in seven deceased patients who were scheduled for autopsy, and were not part of an anatomical donation program for laboratory dissection. 24 They were able to perform sonograms within 12-hour postmortem, which was not possible in a cadaver anatomy laboratory course. 24 In addition, their focus was on kidney volume, which was not the focus of the current study. 24
Limitations
The major limitation to this pilot study was the preexperimental research design that has inherent threats to internal and external validity. The sample size was also limited due to the finite number of cadavers available for use in a semester-long university course. In addition, this basic science study is limited due to scarcity of cadaveric specimens. Beyond the internal validity issues related to the study design, additional concerns center on the organ measurements having been performed by one individual, as well as only one measurement per organ being recorded, in both predissection and postdissection measurement phase. The anatomical board regulations require that laboratory and cadaver access is limited to enrolled students, and laboratory faculty and staff. One member of the research team was authorized to access the laboratory. The host university’s willed body program prioritizes education, and research is not permitted to interfere with the educational mission of the cadaver laboratory. The diagnostic imaging and associated measurements needed to be completed when students were not in the laboratory. An added limitation was the decision to take only one measurement in predissection imaging and postdissection measurement, as well as the delay between predissection imaging and postdissection measurements. The measurement delay was primarily due to the need to work around the cadaver laboratory classes. The laboratory requirements for cadaver care included spraying the cadaver with a Nebanol solution at the end of each lab session and storing it in a cadaver bag, which is designed to help preserve specimens. Thus, the delay in measuring after diagnostic imaging was not expected to impact postdissection measurements due to preservation issues.
Another challenge to executing this study was that the researchers did not have access to the subject’s height and weight, which are known to affect an individual’s kidney size. However, the goal of the current study was not to compare kidney size between the cadaver specimens, but rather to compare sonographic organ measurements with actual specimen measurements. Since sonographic derived and actual organ measurements were compared on the same cadaveric specimen, this limitation was avoided. As noted, not having data on subject’s height and weight, is problematic given those factors influence on organ size.25,26 The objective of this study was to match the sonographically measured size to the actual organ size, within the same cadaver, to determine which sonographic scan planes yielded the most accurate results, not to determine variance between the cadavers. Thus, not having subject’s height and weight had a lesser influence on the results of this study.
Postdissection measurements were completed with a contour gauge, but not sonographically. Because solid organs are curved structures, applying the transducer to the structure ex-situ would not have achieved linear measurements. A water-based acoustic stand-off pad would have been necessary to image postdissection organs and derive linear sonographic measurements, and then the organ measurements would have been sonographically derived, rather than actual organ measurements. The anatomical board did not give permission to place an acoustic stand-off pad on any part of the cadaver specimen. Previous studies by Loftus et al 23 and Koga 27 used water acoustic stand-off pads to image the spleen, those studies were either on specimens waiting for autopsy, or for live patients undergoing splenectomy. Because sonographic liver length (i.e., based on bilateral sonographic scan planes), splenic length, right kidney length (i.e., based on bilateral sonographic scan planes), and the right kidney and left kidney (i.e. based on coronal and anterior sonographic scan planes), did not vary from the actual organ measurements, based on the use of the contour gauge, it appears that the use of the contour gauge, to measure organ length, did not appear to impact the results of the study. In addition, the goal was to compare the predissection sonographic measurements with actual organ measurements, and comparing predissection and postdissection sonographic measurements would not have addressed to study objective.
The acquisition of sonographic measurements was limited by the inability to incorporate patient inspiration that automatically adjusts organ alignment with the ribs. In standard sonograms, patient inspiration is a technique that shifts the abdominal and retroperitoneal organs inferiorly and helps eliminate rib shadowing, which can obscure organ boarders needed for proper caliper placement. Respiration can provide better visualization of the superior portion of the liver and the diaphragmatic border. Without the use of inspiration, only one electronic caliper placement technique could be used for the liver measurements, and some inability to acquire all the specimen images could be attributed to the absence of the respiration technique. The inability to incorporate breathing is an inherent limitation of conducting a cadaver-based study.
A final critique of the study is cadaver management. Despite using best practices, three cadavers grew mold. Because the mold growth was considered serious, the cadavers were removed from the labs. Research has demonstrated that even though cadavers are embalmed, formalin, a ubiquitous embalming agent, does not protect against all bacteria and fungi 28 and that fungi is a common problem in dissection laboratories.29,30 The main impact of removing the cadavers in this study was that it further limited sample size. Another potential impact of cadaver management on this study is that because many undergraduate students were part of the dissection, the variations of their techniques as well as their inexperience in dissection could have impacted the results, in unforeseen ways.
Future research with larger sample sizes is recommended to obtain more robust measurement results. Having more than one measurement per organ, both predissection and postdissection are advised, and incorporating more researchers performing these measurements could mitigate this bias. Future research could expand on these results through comparisons of electronic caliper placement. A survey of ultrasonographers to assess their measurement techniques could be done to better evaluate the current state of practice and contribute knowledge needed to create a standardized sonographic measurement protocol, specific to abdominal and retroperitoneal organs.
Conclusion
Sonography is an effective diagnostic imaging tool to use for evaluating the abdomen and retroperitoneum. The measurements taken can be used by physicians to determine normalcy or aid in a patient’s diagnosis. Historically, these measurements are variable which can lead to additional imaging or evaluation. The results of this study suggest a need for standardization to sonographic organ measurement protocols, particularly when evaluating the kidneys and spleen. Reliable sonographic measurement techniques can improve diagnostic confidence with regards to organ size and patient diagnosis and may prevent unnecessary additional imaging. Reducing excess imaging helps to reduce health care costs, as well as reducing health care institutions’ patient wait times and workload across the imaging specialties.
Footnotes
Acknowledgements
Thank you to Cindy L. Gordon, PhD, Professor and Director of Human Anatomy Program and to Professor Jess Eberle, MS, Anatomy Instructor of Biology in the Dodge College of Arts and Sciences Department of Biology at the University of Oklahoma, for their assistance with this research.
Ethics Approval
Ethical approval for this study was obtained from the institutional review board (IRB #16365) in conjunction with the university willed body program, and the state anatomical board for the research on cadaveric specimens.
Informed Consent
Informed consent was not sought for the present study because all case data were deidentified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not Applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially funded by a University of Oklahoma Health Sciences College of Allied Health Tier 1 Student Creativity Grant.