
Abstract
Sonography is an effective imaging modality for detecting the presence of breast cancer that has metastasized to other organs. Early determination of the presence of these metastatic lesions has proved essential in improving the survival of patients with this disease. This case study presents a patient who was diagnosed with breast cancer, treated, and considered cancer free 9 months prior to the sonogram presented. Within these 9 months, the breast cancer had metastasized to the liver, where it was initially detected on a right upper quadrant sonogram, evaluated further by computed tomography, and definitively diagnosed by histopathology following core needle biopsy.
Keywords
Approximately 250 000 new cases of breast cancer were diagnosed in 2013, with 40 000 related deaths. 1 There are several risk factors for breast cancer such as increasing age, obesity, hormone therapy, physical inactivity, and alcohol consumption.1–4 With primary breast cancer, there is a 5% to 15% likelihood of metastases, most commonly involving the brain, bone, and liver.2–4 This case study presents a patient who was diagnosed with primary breast cancer and presented months later with metastatic spread to the liver.
Case Report
A woman in her late 40s presented to the emergency department with right upper quadrant pain, nausea, and vomiting. She stated that she had been experiencing the pain for approximately 3 days. Nine months prior, she had received her last chemotherapy treatment for her diagnosis of breast cancer and had had an abdominal computed tomogram (CT) that was interpreted as normal. At that same time, she had a double mastectomy to reduce her future chances of acquiring breast cancer again.
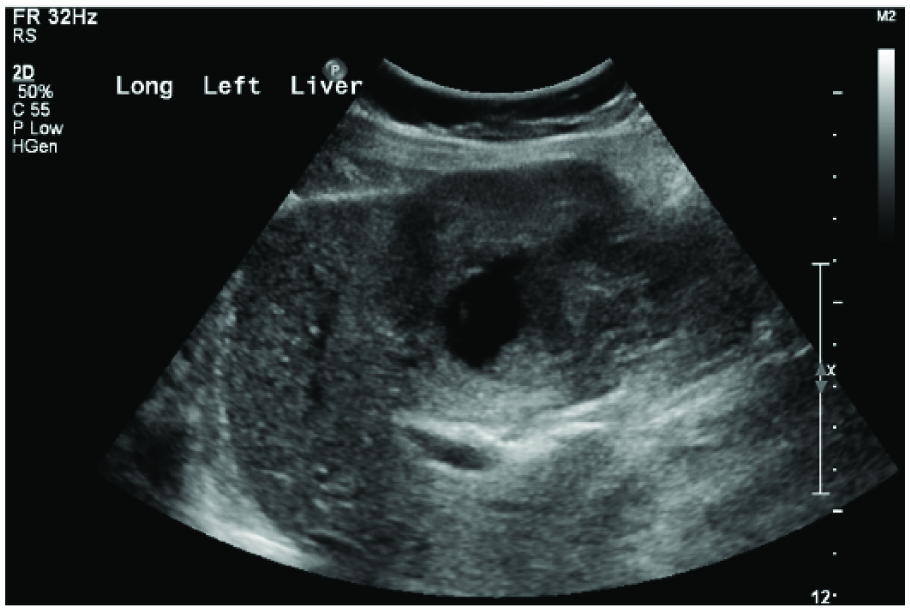
The patient was sent to the sonography department for a right upper quadrant sonogram. A Philips iU22 ultrasound machine (Philips Ultrasound, Bothel, WA) was used with a curvilinear array transducer with a frequency of 5 MHz. The right upper quadrant sonogram showed a mass located in the left lobe of the liver (Figures 1 and 2). The mass measured 6.1 × 8.4 × 5.9 cm and had a heterogeneous echotexture with irregular borders (Figure 3). Color Doppler imaging showed the presence of significant vascularity within and surrounding the mass (Figure 4). The sonogram also visualized the incidental findings of an echogenic hemangioma located in the right lobe of the liver that measured 1.9 × 1.2 × 1.9 cm (Figure 5) and a cyst located in the right lobe of the liver that measured 2.0 × 2.1 × 1.9 cm (Figure 6). Based on the sonographic findings of the suspicious lesion noted in the left lobe of the liver, an abdominal CT was ordered.

Sagittal gray-scale image of the left lobe of the liver showing a large, heterogeneous mass.
Sagittal gray-scale image of the left lobe of the liver taken more medially than the image shown in Figure 1, again showing the large, heterogeneous mass.

Transverse gray-scale image of the left lobe of the liver showing the large, complex heterogeneous mass with a measurement of its largest dimension (8.4 cm).
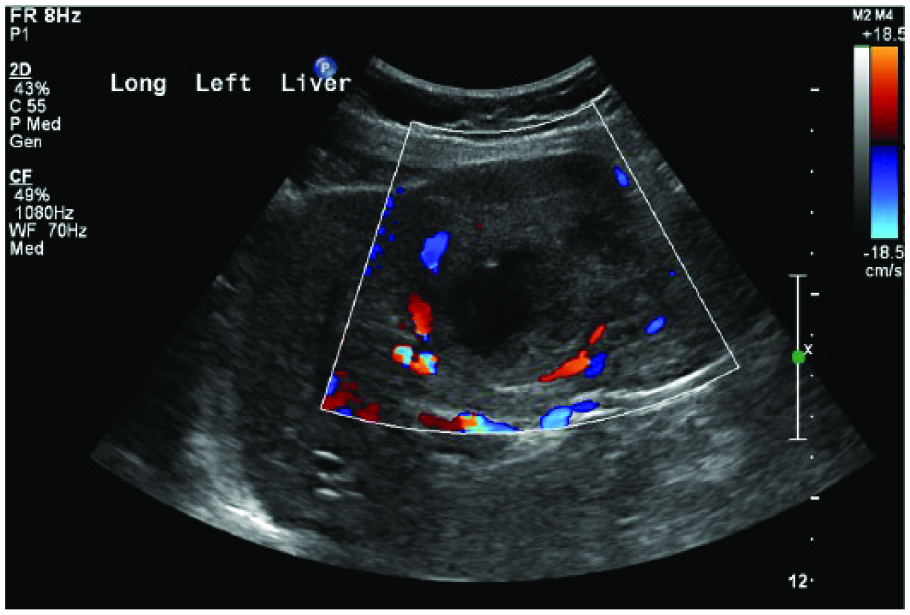
Sagittal color Doppler image of the left lobe of the liver showing the significant internal vascularity of the lesion as well as of the surrounding tissue.
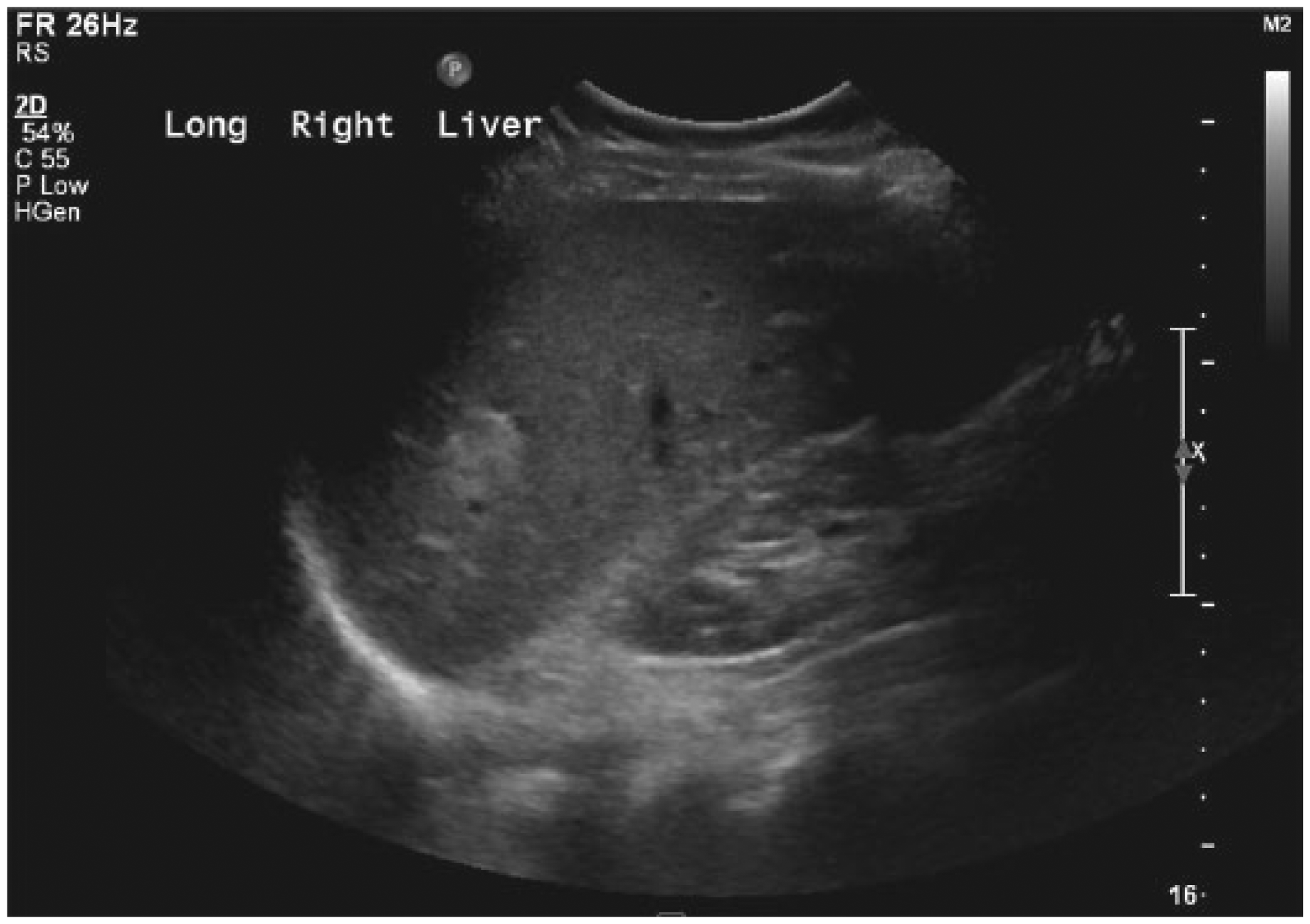
Sagittal gray-scale image of the right lobe of the liver showing the incidental finding of a small echogenic hemangioma.
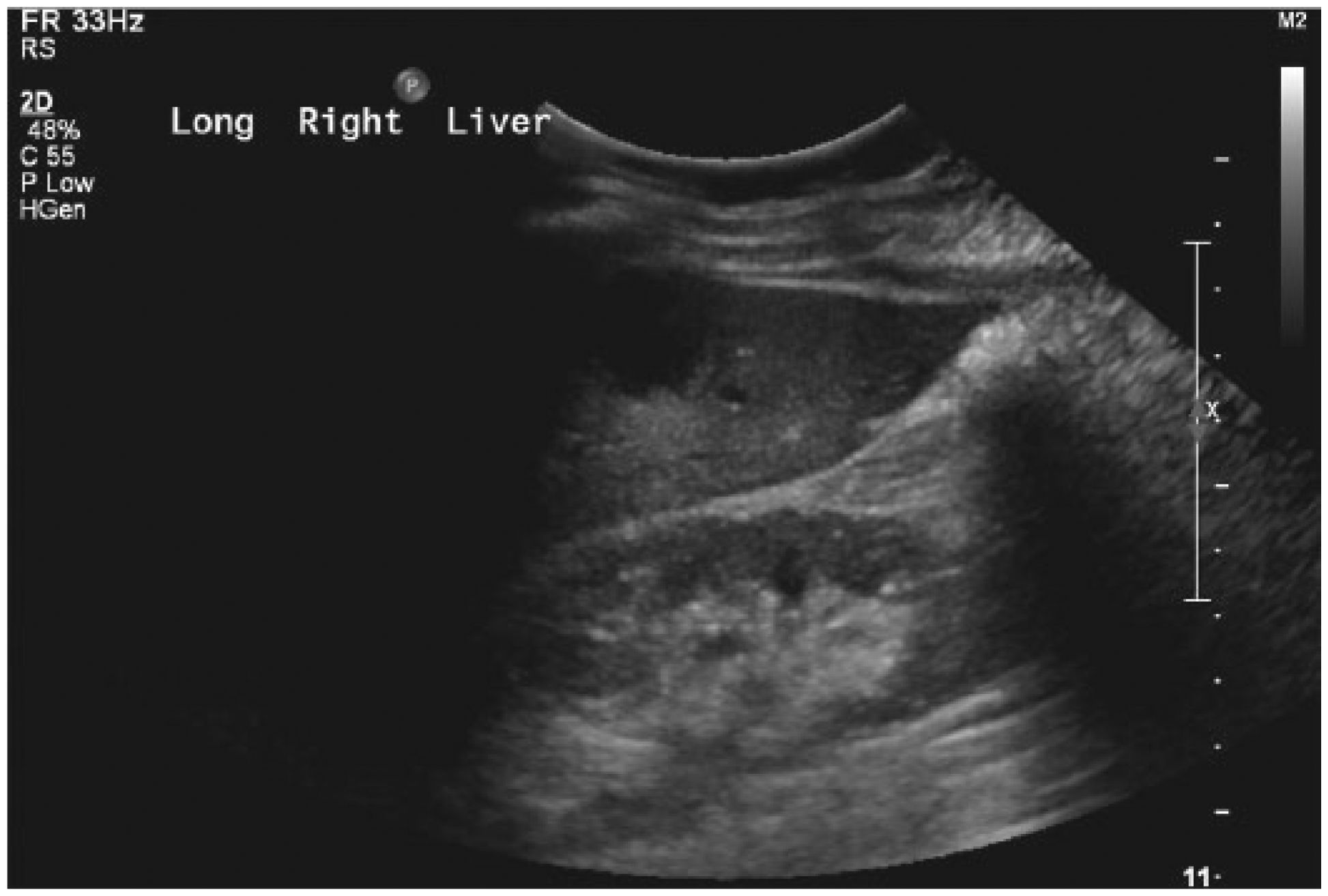
Sagittal gray-scale image of the right lobe of the liver showing the incidental finding of a small cyst.
The abdominal CT with contrast was performed 1 day after the sonogram and showed the mass located in the left lobe of the liver that had been visualized on sonography. The combination of sonographic and CT findings were suspicious for metastatic disease; therefore, a core needle biopsy was done 2 days later. The biopsy results were read as metastatic large-cell carcinoma from primary breast cancer. The patient was informed of her diagnosis and immediately began chemotherapy treatment. Surgical removal of the left lobe of the liver was scheduled for a later date.
Discussion
Breast cancer cells can metastasize through the lymph nodes or the bloodstream to reach other organs. 5 Metastatic spread of breast cancer to the liver is often associated with symptoms including abdominal pain that lasts a significant amount of time, abdominal fullness/bloating, jaundice, an increase in liver function test values, loss of appetite, and weight loss. In cases in which metastatic spread is suspected, diagnostic imaging modalities are essential in determining the presence and extent of metastatic disease.
This case study offers a clear demonstration of how sonography and CT can be used as complementary imaging modalities to determine the presence and extent of metastatic breast cancer to the liver. While sonography is particularly useful in the initial detection of metastatic spread of breast cancer to the liver and offers detailed tissue characterization of suspicious lesions, CT is able to verify the presence of metastatic disease and thoroughly evaluate surrounding structures including bone, pancreas, kidneys, spleen, and adrenal glands for possible spread.
Sonography and CT are the two primary imaging modalities used in examining liver and surrounding structures for metastases. 6 Sonography can provide detail regarding the characterization, classification, and extent of the metastases. In patients with a history of cancer who have sonographic findings suspicious for metastasis, additional tests are typically ordered to further evaluate the metastasis and determine the origin. A CT scan is often the next test performed to examine the liver metastasis as well as to evaluate surrounding organs of interest that metastasis could potentially effect. Based on sonographic and CT results, a core needle biopsy can then be performed to confirm the diagnosis and determine the primary origin of the cancer leading to the liver metastasis. The combination of these imaging modalities offers the most accurate diagnosis possible.
According to the American Cancer Society, metastases occur in the liver in only approximately 1% to 5% of breast cancer patients. 1 The most common areas in which breast cancer metastases occurs are the bone and the brain.2–4,6 These locations cause some of the most severe symptoms, such as weakness, headaches, seizures, and joint pain. 5 Determining the presence of liver metastasis is essential in the patient’s treatment plan and overall prognosis.
There are six principal methods used to treat breast cancer: surgery, radiation therapy, chemotherapy, targeted therapy, sentinel lymph node biopsy followed by surgery, and hormone therapy.6,7 Significant consequences occur when the liver is not able to function properly from the presence of metastasis. Many drugs used to treat primary breast cancer rely on the liver to metabolize the substance contained in the drugs. In turn, the dosage of chemotherapy is affected: if the patient is given a dosage that is too small, the cancer will continue to grow, and the liver will continue to deteriorate. 8 The treatment of liver metastasis includes chemotherapy, with the type of chemotherapy being determined by the primary cancer type. Another treatment method is surgical removal, which is used when the tumor is localized to one lobe in the liver. Patients undergoing hepatic resection have a 5-year survival rate of 9% to 61%. 9 When most or all of the liver is affected, percutaneous embolization can be used to starve or block the blood flow to the liver tumor. The intent is to stop the growth of the metastatic lesion, but this has been shown to be effective in only 63% of patients.8,10
The prognosis for patients with liver metastasis also depends to some extent on the type of primary cancer. A factor important in the case presented was obtaining the complete patient history. Knowing all of the important health information about this patient helped determine the diagnosis of this pathology. Patients with a history of breast cancer and who present with liver metastasis have a shorter life expectancy compared with those who present with bone metastasis. 8 The surgical removal of the primary cancer rarely results in a cure. The long-term prognosis of liver metastasis is poor, with a 5-year survival rate of only 23% despite aggressive treatment. 10 Although treatment can be performed to shrink the tumor or reduce symptoms, patients who have cancer that has spread to the liver typically live less than 6 months after the diagnosis.8,11
Conclusion
Sonography provided a quick, noninvasive imaging modality used to evaluate and characterize a suspicious liver lesion. With the knowledge gained from a complete patient history, sonography proved to be beneficial in reaching an early diagnosis of metastatic breast cancer to the liver. Without this knowledge of the patient’s history of breast cancer, the appropriate diagnosis would not likely have been determined in such a timely manner. Based on the sonographic findings suspicious for metastasis, further evaluation using CT enabled the visualization of the extent of the lesion to the liver without involvement of surrounding organs. Further testing resulted in the patient’s being able to begin the appropriate treatment promptly.
Footnotes
Acknowledgements
The authors thank Dee Sharrock, Mark Tinsley, C. W. Scheidt, Michelle Klenklen, Jenny Seaton, Courtney Camp, Marsha Glaskey, Wendy Benn, Jessica Bright, and the University of Missouri Diagnostic Medical Ultrasound staff for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.