
Abstract
Breast cancer liver metastasis (BCLM) is considered to occur by hematogenous spread of primary breast cancer cells. We herein present a case of lymphatic BCLM that was confirmed by preoperative imaging for sentinel lymph node biopsy (SLNB). A woman in her early 70s was diagnosed with clinical stage T2N0M0 invasive lobular cancer of the left breast. She underwent mastectomy with SLNB. Preoperative lymphoscintigraphy showed intense accumulation of isotope in the upper abdomen, corresponding to segment IV of the liver on single-photon emission computed tomography/computed tomography (SPECT/CT). However, no abnormalities were detected on magnetic resonance imaging. At 2.5 years postoperatively, the patient’s serum CA15-3 concentration was elevated, and positron emission tomography/computed tomography (PET/CT) showed a solitary liver metastasis. The PET/CT findings were similar to the SPECT/CT findings obtained 2.5 years earlier, indicating that the BCLM had developed lymphatically. To the best of our knowledge, this is the first case report of lymphatic BCLM proven by imaging examination.
Keywords
Introduction
Lymphoscintigraphy is primarily performed to trace lymph drainage. In lymphoscintigraphy for sentinel lymph node biopsy (SLNB) in patients with breast cancer, not only the ipsilateral axillary lymph nodes but also extra-axillary drainage (e.g., the internal mammary chain and subclavicular region) may be visualized. 1 However, liver accumulation on lymphoscintigraphy is extremely rare; only one case has been reported to date. 2
Lymph drains from the lower inner part of the breast to the liver, penetrating the rectus abdominis muscle. 3 This route is considered important for the development of breast cancer liver metastasis (BCLM). 4 However, it is difficult to prove whether BCLM is hematogenous or lymphogenous in clinical practice. We herein present an extremely rare case of BCLM that developed via the lymphatic vessels as assessed by preoperative imaging. Identifying the presence of lymphatic liver metastasis may provide an additional local treatment option for liver metastases that are usually treated with systemic therapy.
Case Report
A woman in her early 70s presented to our hospital with a left breast lump. She had no history of breast surgery. The tumor measured 3 cm in the upper outer quadrant and was diagnosed as invasive carcinoma by means of core needle biopsy. Computed tomography (CT) of the chest, abdomen, and pelvis showed no signs of distant metastases or enlarged regional lymph nodes. Preoperative lymphoscintigraphy was performed to identify the sentinel lymph nodes. Technetium-99m nanocolloid was intradermally injected into the periareolar region at a dose of 74 MBq. Three hours after this injection, scintigraphic sequential planar images showed weak tracer accumulation in the axilla and intense accumulation in the upper abdominal region (Figure 1).

Lymphoscintigraphy images obtained 3 hours after injection showing weak tracer accumulation in the axilla and intense accumulation in the upper abdominal region. The injection site is shielded using a lead plate. (a) Anterior view. (b) Left anterior oblique view.
Following lymphoscintigraphy, single-photon emission CT/CT (SPECT/CT) was performed to show the exact anatomical localization of radiotracer uptake. SPECT/CT showed intense tracer accumulation in segment IV (S4) of the liver (Figure 2). The patient underwent total mastectomy with SLNB. Intraoperative identification of the sentinel lymph node was performed using a gamma probe and vital blue dye, and one radioactive node and two neighboring non-radioactive nodes were excised. Intraoperative examination showed no metastases in these lymph nodes. Therefore, axillary lymph node dissection was not performed. The hot spot of the liver was left untouched. Histopathological examination showed invasive lobular carcinoma with a 6-cm spread. Immunohistochemistry of the tumor showed positivity for estrogen receptor, negativity for progesterone receptor, 2+ positivity for human epidermal growth factor receptor 2, and negative results of dual-color in situ hybridization.

Single-photon emission computed tomography revealing focal uptake in the medial segment IV of the liver. (a) Axial plane. (b) Coronal plane.
Postoperatively, the patient underwent adjuvant chemotherapy with the EC four-cycle protocol (epirubicin 90 mg/m2, cyclophosphamide 600 mg/m2) and radiotherapy (50 Gy/25 fractions) to the chest wall and supraclavicular area, followed by hormonal therapy with an aromatase inhibitor (anastrozole at 1 mg once daily). Liver magnetic resonance imaging performed 86 days postoperatively showed no abnormal lesions or metastases (Figure 3).
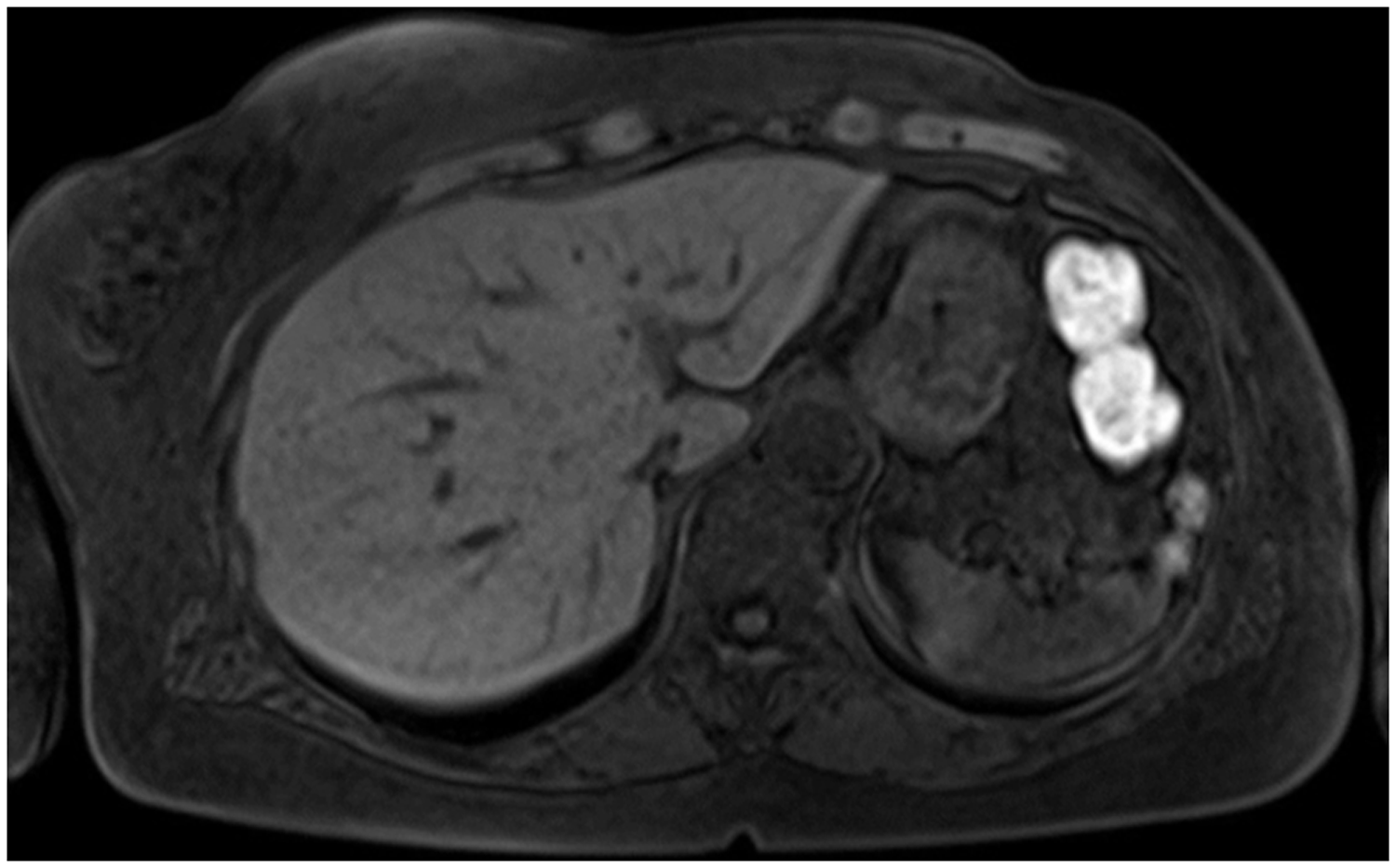
Liver magnetic resonance imaging performed 86 days postmastectomy showing no abnormal lesions or metastases.
The patient underwent regular follow-up every 3 months. Two years 6 months after the operation, her CA15-3 concentration was elevated. No clinical manifestations were observed. 18F-fluorodeoxyglucose positron emission tomography with concurrent CT (PET/CT) showed focal 18F-fluorodeoxyglucose accumulation in S4 of the liver, with no other distant or locoregional metastases (Figure 4).

Positron emission tomography/computed tomography performed 2.5 years postoperatively showing a solitary liver metastasis with no other distant or locoregional metastases.
PET/CT showed exactly the same finding as SPECT/CT performed 2.5 years earlier. Liver biopsies were taken, and the histological findings were consistent with breast cancer metastasis. Immunohistochemistry showed positivity for gross cystic disease fluid protein 15, weak positivity for estrogen receptor, negativity for progesterone receptor, and negativity for human epidermal growth factor.
Chemotherapy was administered for this recurrence. In addition, upon the patient’s request, proton beam therapy was delivered as a local treatment at another hospital. At the time of this writing (>5 years after detection of the liver metastasis), the patient was alive with no further recurrent lesions.
Written informed consent for publication was obtained from the patient. Because this is a case report, ethics committee approval was not required. The reporting of this study conforms to the CARE guidelines. 5
Discussion
Lymphoscintigraphy is performed to trace lymph flow and is routinely used to visualize the sentinel lymph nodes in patients with breast cancer. 6 The lymphatic drainage pathway from the breast is mainly toward the axilla, 7 and axillary sentinel lymph nodes can be visualized in 97.5% of patients with breast cancer. 8 Lymphoscintigraphy can also identify extra-axillary sentinel lymph nodes of the internal mammary chain and supraclavicular and contralateral axillary sentinel lymph nodes. 1 However, planar lymphoscintigraphy does not always delineate the exact anatomical location of the sentinel lymph nodes. Subsequent SPECT/CT can provide an accurate image to overcome this difficulty.9,10
Our patient had abnormal uptake in the upper abdomen on lymphoscintigraphy, and additional SPECT/CT showed that it corresponded to S4 of the liver. Focal uptake by the lymphatic system in the liver is extremely rare. 5 In our institution, lymphoscintigraphy for SLNB was performed for 4659 patients from January 2001 to December 2020, and no patients other than the patient described in the present report showed focal uptake in the liver. In a consequent literature search of PubMed using the keywords “breast cancer,” “lymphoscintigraphy,” and “liver,” only one case report of focal accumulation in S4 of the liver described the use of lymphoscintigraphy with SPECT/CT. In this case report, one internal mammary lymph node and two axillary lymph nodes were observed in addition to the hot spot of S4. However, whether metastasis occurred at these sites was not reported. 6 To the best of our knowledge, the present case is the first report of lymphatic liver metastasis from breast cancer confirmed using lymphoscintigraphy followed by SPECT/CT.
Lymphatic flow drains the lower inner part of the breast toward the liver, penetrating the rectus abdominis muscle. This lymphatic route originates from the internal mammary lymphatic system of the diaphragm and liver. 3 Therefore, this route is considered important for lymphatic metastasis to the liver. 4 A falciform ligament is present in the vicinity of S4 of the liver; it involves lymphatic flow from the liver toward the diaphragm. Lymphatic BCLM is thought to occur by retrograde lymph flow secondary to lymph vessel obstruction caused by extensive involvement of the regional lymph nodes. In the present case, which involved no regional lymph node metastases, we consider that the liver metastasis occurred by direct lymph flow from the breast to the liver. 11
In contrast, liver uptake is related to the injection technique. Normally, technetium-99m nanocolloid, a tracer for lymphoscintigraphy, enters the lymphatic vessels through a subcutaneous injection and is trapped by the reticuloendothelial system of regional lymph nodes; the sentinel lymph node is then visualized. If the tracer is injected into a blood vessel and enters the bloodstream, it is phagocytosed by Kupffer cells, and the liver is delineated.12,13 The tracer accumulates in the normal liver but not in metastatic areas, resulting in a defective image.
BCLM is considered a systemic disease because of its hematogenous spread, 14 and it has a poor prognosis. 15 Therefore, even when isolated BCLM occurs as the first recurrence, systemic treatment is usually chosen. In our case, proton therapy was added to the systemic chemotherapy to treat the BCLM at the patient’s request. The proton therapy was performed at another hospital. Consequently, long-term stable disease has been maintained for more than 5 years, and no metastasis has been found except in the liver. The reason for this could be that the mechanism of BCLM is lymphogenous and localized, similar to regional lymph node recurrence, making local treatment more effective.
In conclusion, we experienced an extremely rare case of BCLM that developed via the lymphatic vessels as determined by preoperative imaging. SPECT/CT was useful to determine the exact anatomical location of abnormal extra-axillary uptake on lymphoscintigraphy. The patient has remained stable for more than 5 years. Lymphatic BCLM may have a better long-term prognosis than hematogenous BCLM.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211064793 - Supplemental material for Metastasis of breast cancer to liver through direct lymphatic drainage: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605211064793 for Metastasis of breast cancer to liver through direct lymphatic drainage: a case report by Hiromi Tokisawa, Tomoyuki Aruga, Yuichi Kumaki, Naoko Iwamoto, Rika Yonekura, Toshiyuki Ishiba, Yayoi Honda and Mizuka Suzuki in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank our colleagues at the Department of Breast Surgery and Reconstructive Surgery, Tokyo Metropolitan Cancer and Infectious Disease Center Komagome Hospital. We would also like to thank Toshinari Yamashita for her assistance in preparing the manuscript. Finally, we thank Editage (![]() ) for performing English language editing of the manuscript.
) for performing English language editing of the manuscript.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T. Aruga has received honoraria from Chugai Pharmaceutical Co. Ltd., AstraZeneca K.K., Eli Lilly Japan K.K., and Pfizer Japan Inc. The other authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.