
Abstract
Hepatic abscesses are masses or lesions within the liver as a response to an infection manifesting into the liver. Hepatic abscess can be a result of other abdominal diseases, such as any biliary tract disease or appendicitis. Because of its inconsistent characteristics in many imaging modalities, its appearance can be mistaken for other pathologies like liver metastasis. With the use of one or more imaging modalities and an imaging-guided biopsy of the targeted lesion, hepatic abscess can be confirmed. The case presents multiple hepatic abscesses throughout the liver with similar imaging characteristics as that of metastasis. Computed tomography (CT), sonography, magnetic resonance imaging, and a biopsy were performed to successfully diagnose the hepatic abscesses.
Hepatic abscesses are lesions in the liver caused by bacterial, parasitic, or fungal infections as a response to the presence of diseases such as appendicitis or, more commonly, biliary tract diseases.1,2 Although hepatic abscesses have no specific clinical symptoms, in over 50% of patients present with fever and/or abdominal pain.2,3 Sonography, computed tomography (CT), and magnetic resonance imaging (MRI) are used to visualize and play a role in the process of diagnosing hepatic abscesses, in about 90% of patient cases.3,4 However, because of hepatic abscesses’ variable appearance, these imaging modalities are not able to consistently provide a definite diagnosis without the results of a fine-needle aspiration, to confirm the diagnosis.3,4 This case report presents the results of an inpatient with multiple hepatic abscesses and sonographic characteristics that were similar to metastatic disease.
Case Report
A 70-year-old man was admitted to the emergency department with a body temperature of 99°F and abdominal pain. The patient’s medical lab results showed an elevation in blood urea nitrogen (BUN), creatinine, alanine transaminase (ALT), and aspartate transaminase (AST) levels, indicating a complication with liver function. 5 An abdomen and pelvis non-contrast CT examination was ordered for the clinical indications of abdominal pain and septic shock. Multiple low-attenuating lesions were seen in the dome of the liver (see Figure 1). An abdominal sonogram was recommended to further assess the lesions, within the liver.
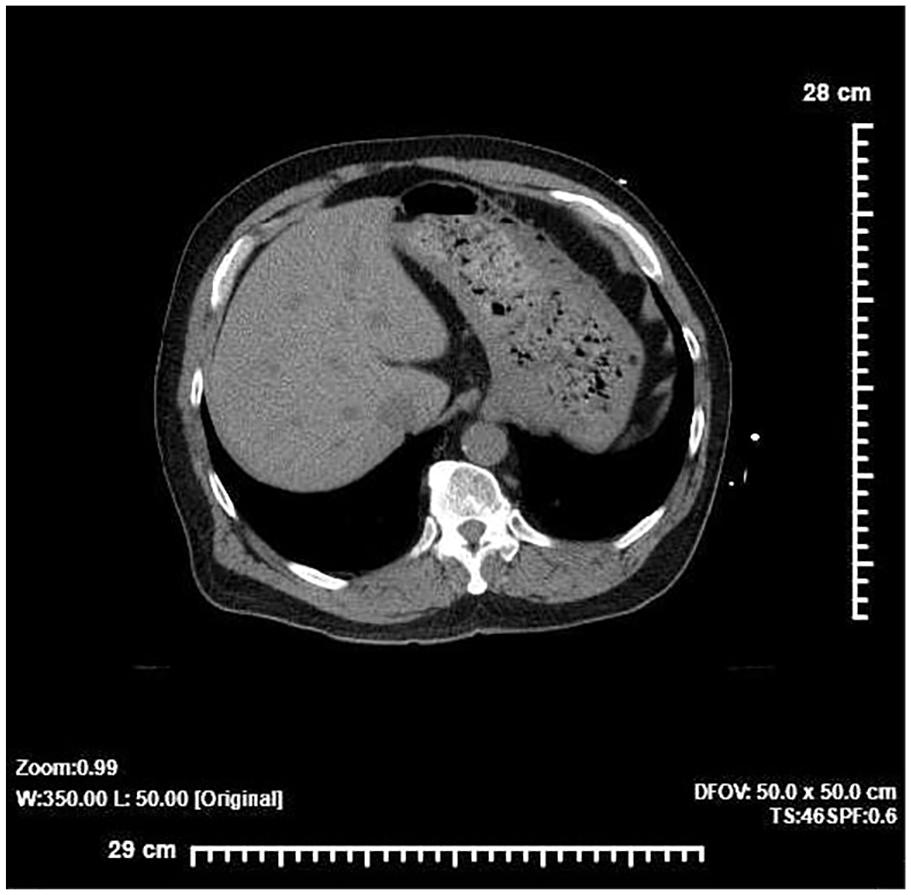
A transverse view of an abdominal computed tomogram, without contrast, demonstrated multiple low-attenuating hepatic lesions, throughout the liver.
The next day an abdominal sonogram was performed with a Philips EPIQ 7 ultrasound equipment system, utilizing a 5-1 MHz curvilinear array transducer. Multiple hypoechoic hepatic lesions were seen throughout both lobes of the liver (Figures 2 and 3). The largest lesion was seen posterior to the porta hepatis, in Couinaud’s V segment and measured 3.98 cm × 2.39 cm × 3.80 cm, presenting with an isoechoic rim (see Figure 4). With its proximity to the porta hepatis, color Doppler was used to document the patency of the main portal vein and the hepatic artery (see Figure 5). The gallbladder, common bile duct, pancreas, and right kidney were unremarkable. The radiologist suggested that the hepatic lesions were most likely the repetitiveness of a metastatic disease.
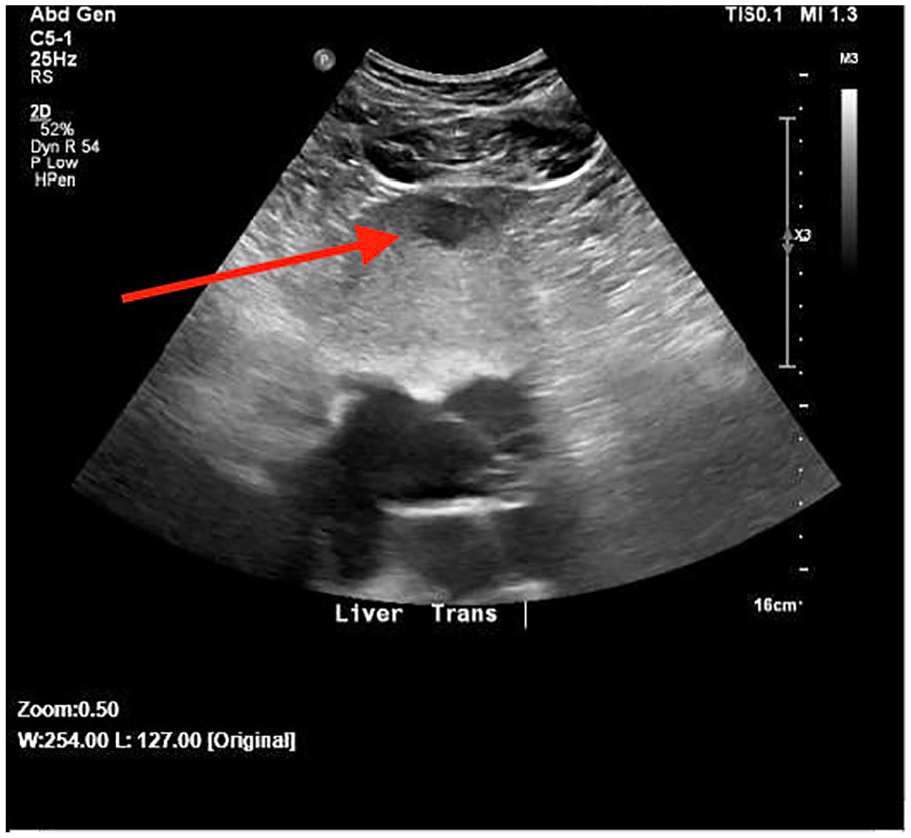
A transverse abdominal sonogram demonstrated a hypoechoic lesion (arrow pointing to it) in the dome of the left liver lobe.

A sagittal abdominal sonogram showing multiple hypoechoic lesions in the right lobe of the liver.
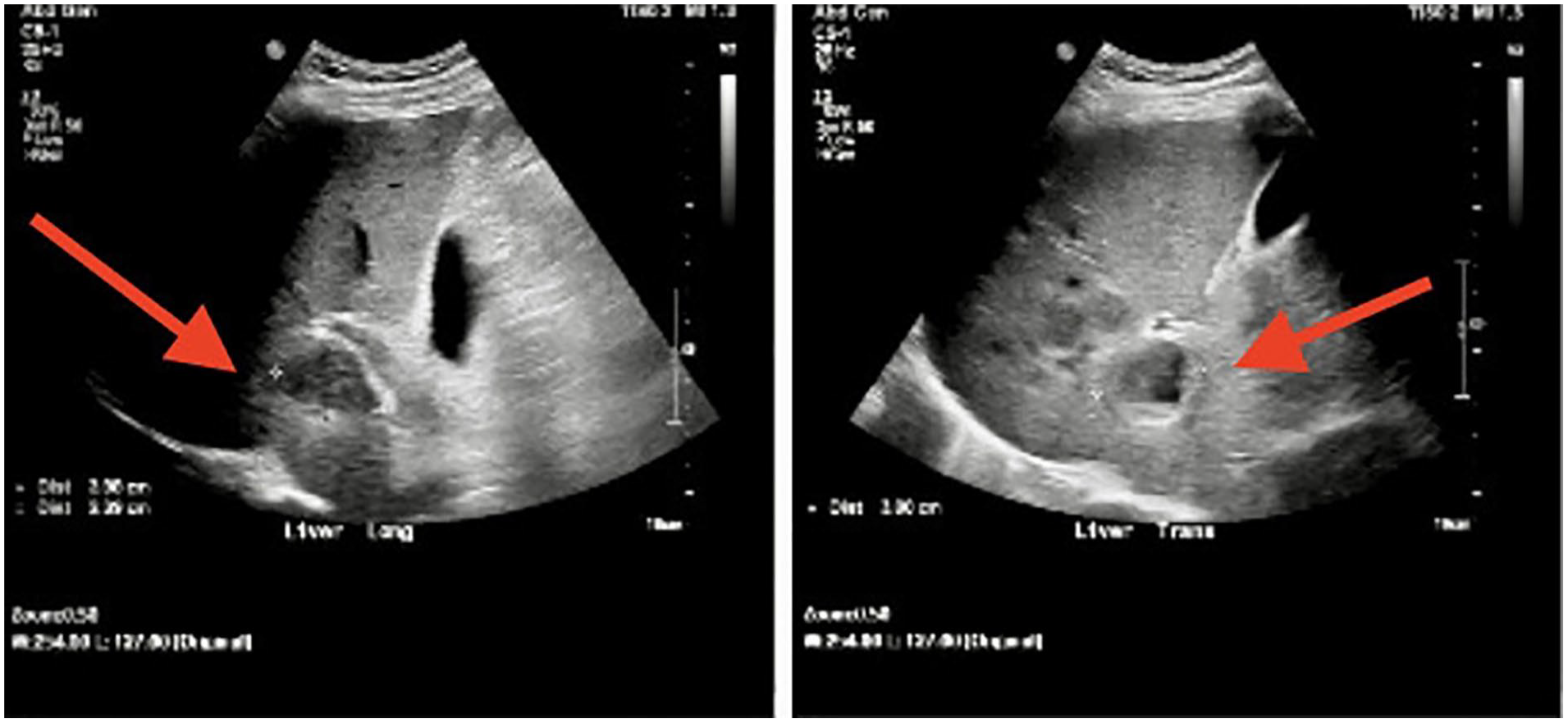
A sagittal and transverse sonogram of the largest liver lesion (arrow pointing to it) which measured 3.98 cm × 2.39 cm × 3.80 cm.
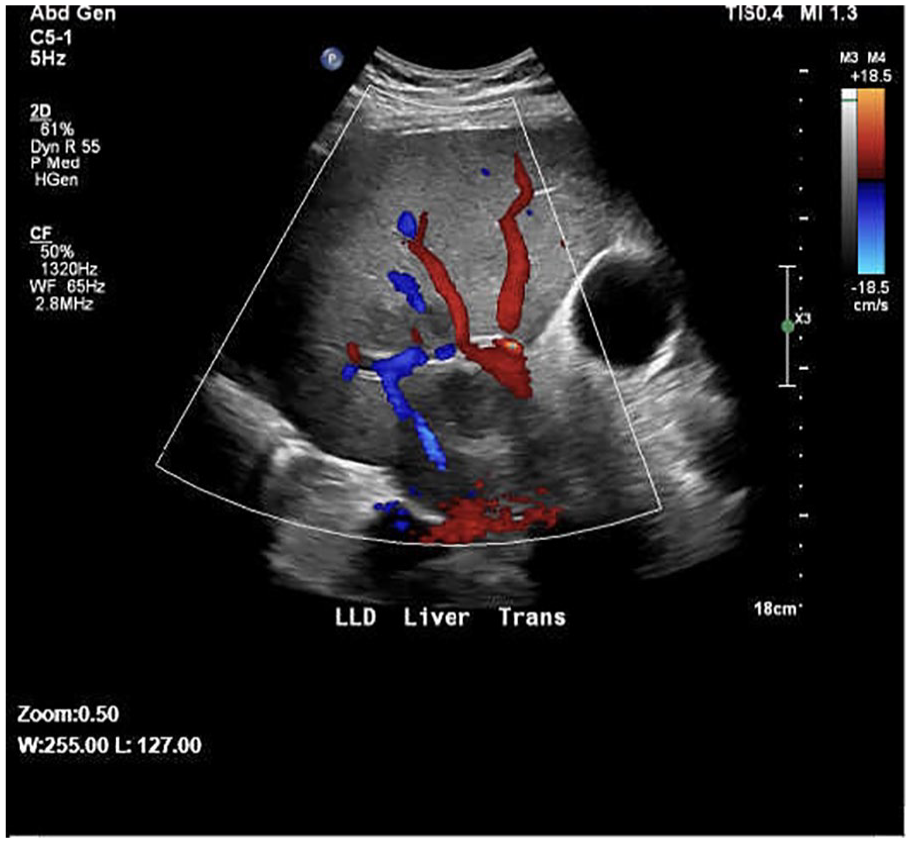
A transverse sonogram demonstrating the lesion near the portal triad, with the patient in left lateral decubitus position. Color Doppler is applied to show patency of the portal vein, hepatic artery, and surrounding hepatic veins.
On the same day, after the abdominal sonogram, an abdominal MRI was performed with a clinical indication of liver disease. A T2-weighted MRI and short tau inversion recovery (STIR) sequences were performed to determine the presence of fatty or water-based tissue and document the intensity of the liver lesions, which can indicate metastasis.6,7 Multiple hyperintense T2 and STIR lesions were found throughout both lobes of the liver (see Figure 6). The radiologist suggested a liver biopsy to distinguish the hepatic lesions between metastatic disease and abscesses.
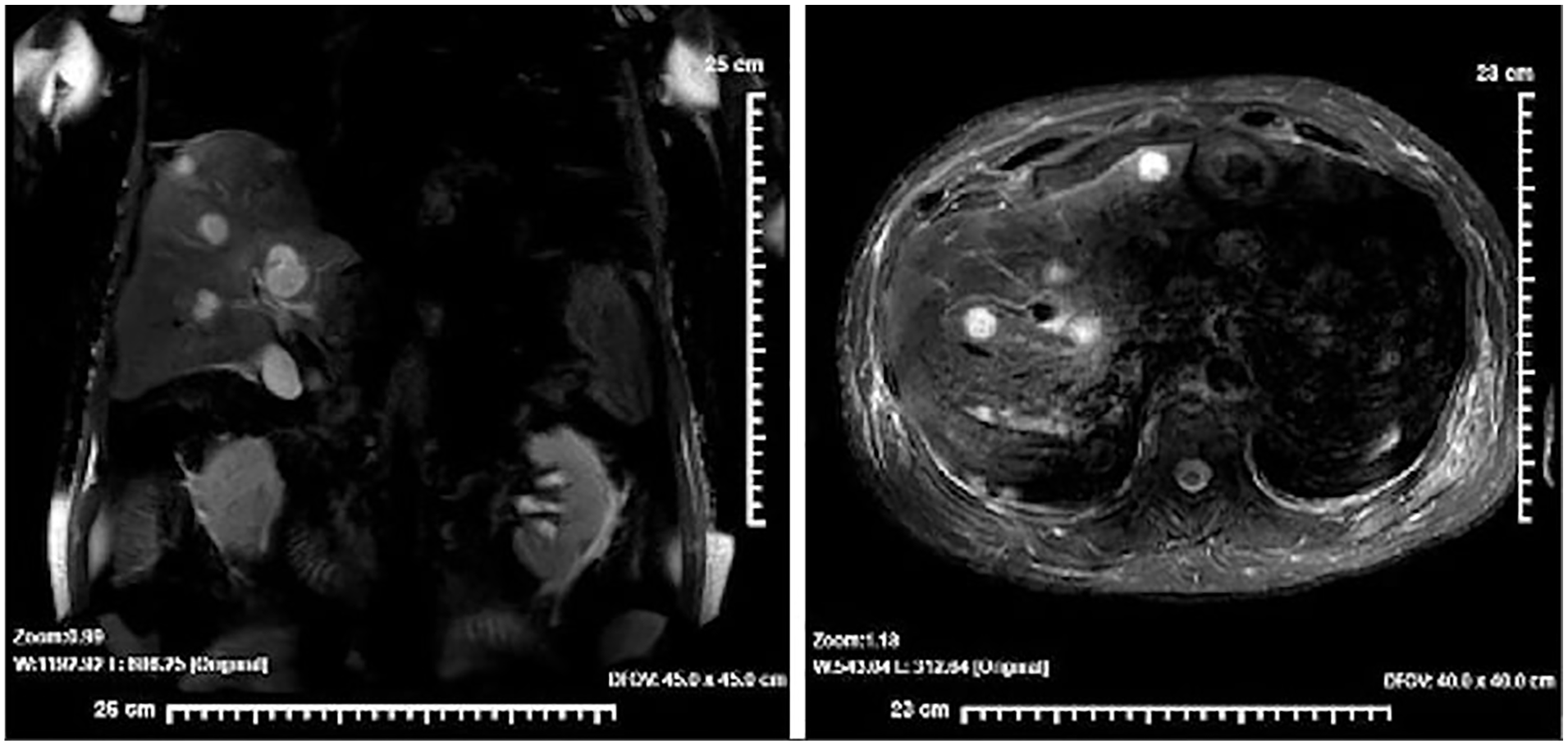
Coronal and transverse magnetic resonance imaging views demonstrate multiple hyperintense lesions, within the liver.
On the same day as the sonogram and the MRI, the patient began antibiotic treatment for septic shock, the initial diagnosis. A few days after the beginning of the antibiotic treatment, another abdominal sonogram was performed. For this sonogram, a GE LOGIQ E10 ultrasound equipment system, with a 6 MHz curvilinear array transducer, was used. The sonogram showed a slightly hypoechoic lesion in the left lobe of the liver measuring 1.26 cm × 1.19 cm × 1.58 cm (see Figure 7). The multiple hypoechoic hepatic lesions seen in the previous sonogram were no longer present (see Figure 8). No trace of a hepatic lesion was seen near the porta hepatis or throughout the right lobe (see Figure 9).
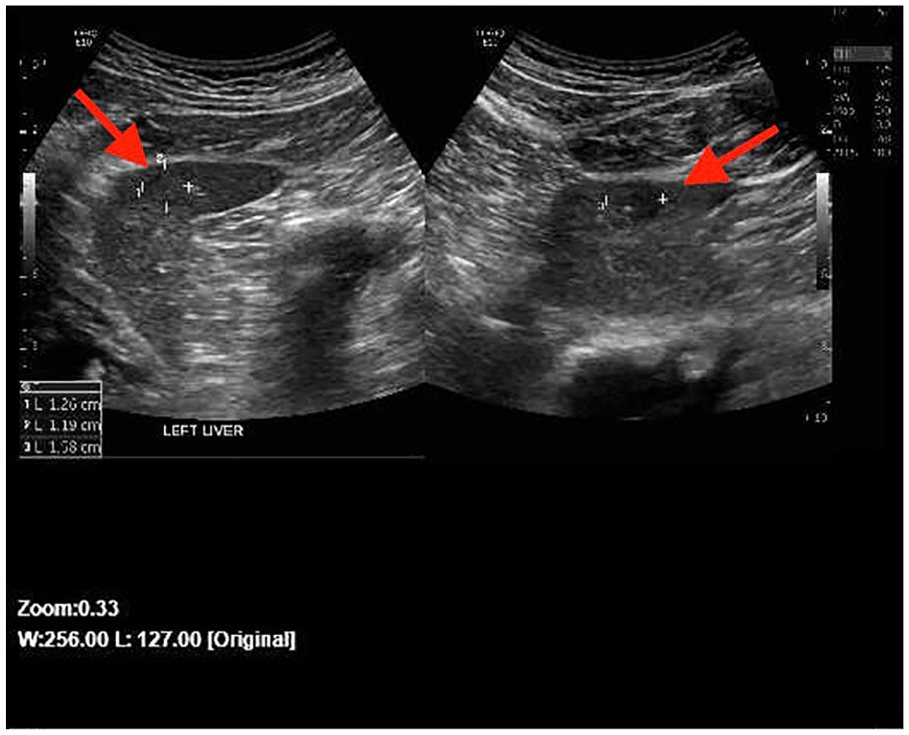
Sagittal and transverse sonographic views of the only remaining lesion (arrow pointing to it) in the liver. A hypoechoic to isoechoic lesion in the left liver measured 1.26 cm × 1.19 cm × 1.58 cm.
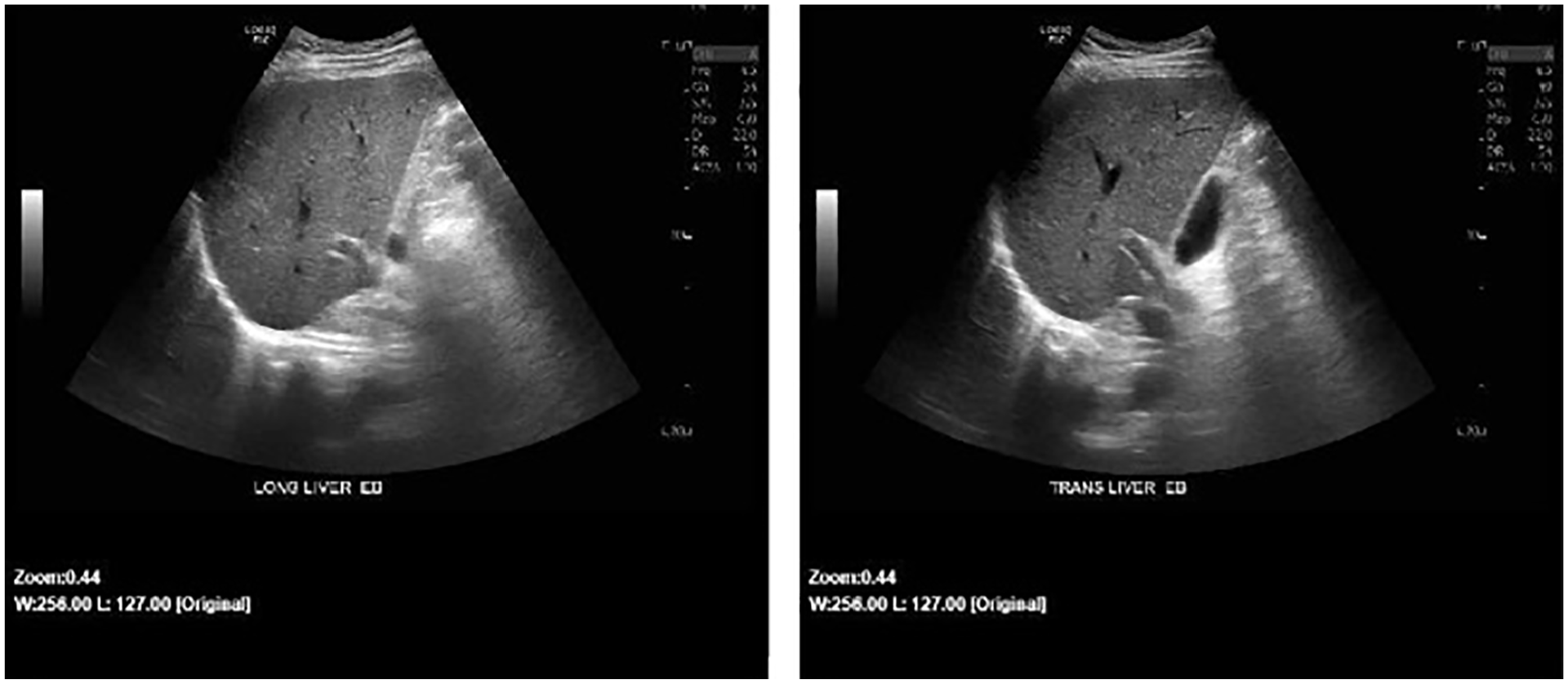
Sagittal and transverse abdominal sonographic images showed a clear right liver. The lesions seen in the previous abdominal sonogram were no longer present.
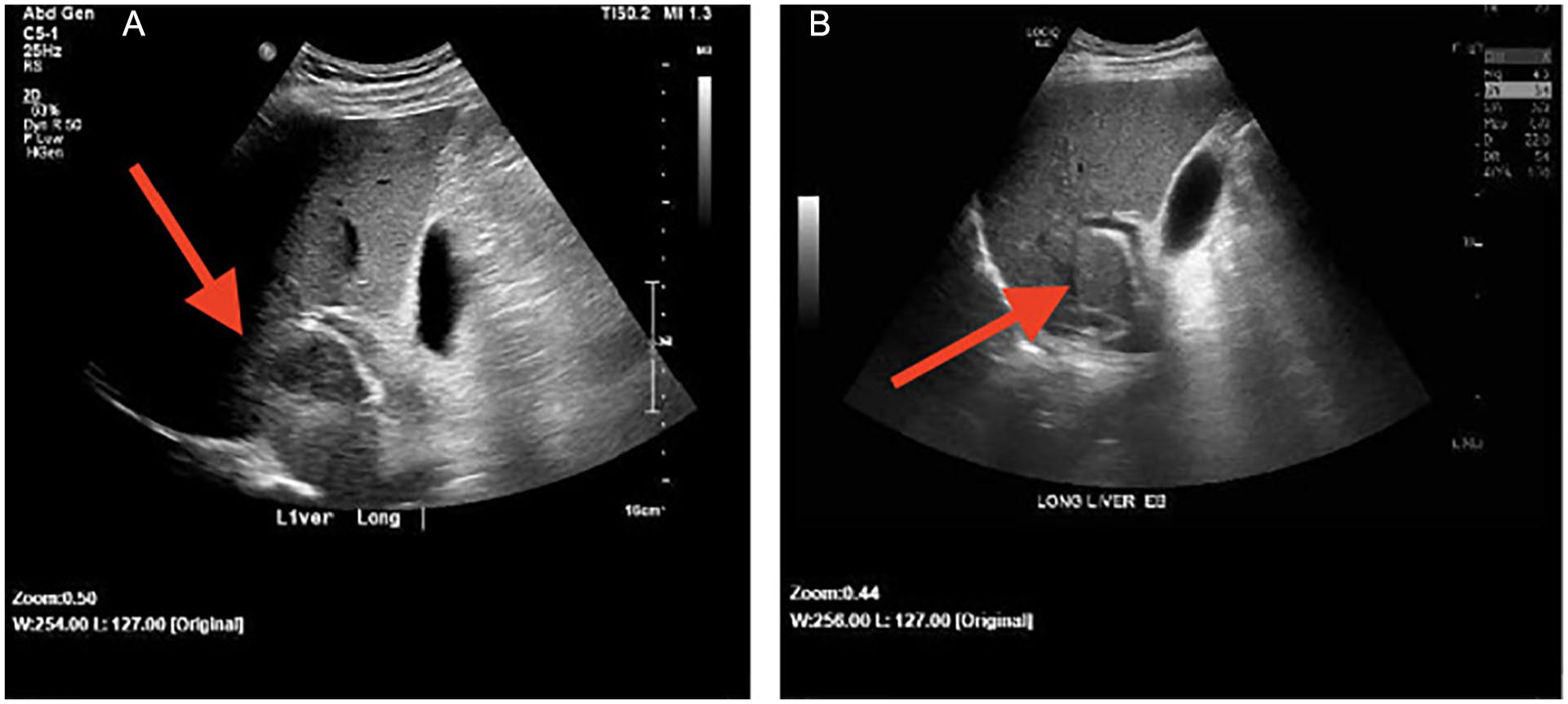
A sagittal abdominal sonographic image of the liver lesion (arrow pointing to it): (A) before treatment and an image of the portal triad and (B) area after treatment. In image B, there is no lesion present (arrow pointing to the region), compared to the prior sonogram.
A week after the last abdominal sonogram, a CT-guided liver biopsy was performed on the remaining hepatic lesion in the left lobe of the liver. The results of the biopsy confirmed that the cells of the lesion were consistent with an organizing abscess with a trace of granulomatous foci.
Discussion
The liver is a large organ, within the human body, which takes up the majority of the right upper quadrant. The liver has a homogeneous texture which can be detected in some imaging modalities such as sonography, CT, and MRI. The liver is divided into multiple sections by the vessels that drains and supplies it, the hepatic and portal veins. 8 The portal triad consists of three vessels: the hepatic artery, portal vein, and the bile duct. 8 These vessels communicate with the liver by either supplying blood or removing bile products from the liver. If there were to be a disease within one of the vessels, an infection within the liver can occur. 2
The presence of hepatic abscesses usually suggests the presence of some type of infection. There are two common types of hepatic abscesses: pyogenic abscess and amoebic abscess. Pyogenic abscess occurs when the immune function is compromised due to pathogens such as Escherichia coli or Klebsiella pneumoniae.8,9 Amoebic abscess is caused by an Entamoeba histolytica, a parasite, that was received from contaminated food or water.8,9 Although the microorganisms are different, both types of abscesses travel to the liver in the same fashion. The infections most commonly travel to the liver via the portal vein or the biliary tract. 2 Because of its function within the liver, an infection within the biliary tract can lead to the formation of hepatic abscesses. 3 The formation of these hepatic abscesses presents with other clinical symptoms.
An abscess’ clinical symptoms are similar to the symptoms of an infection because of the microorganisms that are possibly affecting the immune system. Some of the most common clinical symptoms of an infection that are also seen with hepatic abscesses are fever and abdominal pain.2,3 About 90% of hepatic abscess cases are presented with fever as a symptom, and about 50% present with abdominal pain. 2 Laboratory tests may show an elevation in liver function tests (LFTs) and an elevation in the number of white blood cells.3,8
Hepatic abscesses do not have a definite sonographic appearance. Its appearance is variable; therefore, there is a chance of being misdiagnosed, without further clinical information. These lesions can appear as hypoechoic with well-rounded borders or heterogeneous with irregular borders.3,10 Ninety percent of the time, pyogenic abscesses appear with irregular borders. 8 Pyogenic abscesses are more likely to have a heterogeneous pattern due to the pus or debris it may contain. 4 Sonographically, amoebic abscesses can change over time. Initially, just like the pyogenic abscesses, the amoebic abscesses have an irregular contour, but as it begins to mature it becomes more hypoechoic and well-defined.8,10 As it matures, the walls of the abscess begin to thicken and form the sonographic “target” appearance. 3 When clinical and imaging characteristics align to diagnose a hepatic abscess, sonography and CT can be used to better differentiate hepatic abscesses from differential diagnoses like hepatic metastases.
However, there are cases where the characteristics are indeterminate and further testing is necessary to provide a diagnosis. Fever and abdominal pain are also non-specific symptoms of certain malignancies like metastasis. 10 Sonography and CT are the more common imaging modalities to image the liver for possible abscesses. Although sonography is usually the first choice of imaging for hepatic abscesses, CT has a 97% sensitivity while sonography has a 85% sensitivity for diagnosing liver abscesses.2,9,11 However, some cases of hepatic abscesses have presented itself with similar characteristics as metastasis. 10 Because of its variable appearances in both sonography and CT, a biopsy is usually suggested as a follow-up for confirmation. An image-guided biopsy is able to conclusively diagnose hepatic abscesses.
Depending on the abscess’ reaction to the antibiotics, antibiotics can solely treat the abscess, clearing everything in 3 to 4 weeks. 12 Amoebic abscesses are usually treated solely with antibiotics. 9 However, when dealing with more complex abscesses or pyogenic abscesses (abscesses that contain pus), antibiotics would be a portion of the overall treatment for the hepatic abscesses. Fine-needle aspirations guided with sonography or CT with the addition of antibiotics is the usual treatment for pyogenic abscesses.9,12 Surgical drainage of the abscess is the less common method of treatment due to its level of invasiveness. 9
Conclusion
Hepatic abscesses can change over time, with a higher occurrence due to biliary tract disease compared to appendicitis or other inflammatory bowel diseases. 13 Although there is no definite sonographic appearance of hepatic abscess, general appearances such as the “target” appearance with the addition of clinical symptoms of fever or abdominal pain can lead to a definite diagnosis of hepatic abscesses. This case report demonstrated the importance and effectiveness of the use of sonography for continuous follow-up imaging. This case reiterated the importance of understanding possible differentials and their similar characteristics. It is important to look at the overall clinical picture when dealing with possible diagnostic differentials.
Footnotes
Acknowledgements
The authors would like to thank Melissa Hirner, RDMS, RVT, Emily Baum, RDMS, RVT, Blanca Joya, RDMS, and Mia Meurer, RVT, for their support, time, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.