
Abstract
Objective:
Breast cancer is a leading cause of mortality in industrialized and developing countries. Mammography and a core needle biopsy are among the detection methods that are used to diagnose and confirm tumor subtypes.
Methods:
A retrospective, noninterventional observational study was conducted in a tertiary center between January 2009 and December 2014. A total of 265 patients underwent ultrasonography (US)–guided core needle biopsy (CNB). A cohort of 147 patients met the inclusion criteria and data were subsequently extracted from their medical records.
Results:
From this cohort, US-CNB detected malignant lesions in 109 patients, with a total sensitivity and specificity for malignancy at 96.33% and 75.10%, respectively. The most frequent malignant tumor diagnosed with US-CNB was invasive ductal carcinoma. The most common benign masses detected were 38 (32.1%) fibroadenomas and fat necrosis. The positive and negative predictive values for US-CNB were 92.4% and 87.5%, respectively.
Conclusion:
The findings would suggest that the use of US-CNB could play a major role in the identification and management of the breast lesions. It could also redeem any biopsy errors or operator inexperience. Sensitivity and specificity in detecting tumors, malignant or benign, using US-CNB could aid in efforts to provide an appropriate medical management plan.
Breast cancer is the most commonly diagnosed cancer among females and is among the leading causes of cancer-related deaths in females worldwide. Breast cancer accounts for more than 23% of newly diagnosed cancers and 14% of cancer mortality. 1 Currently, breast cancer burdens both industrialized and developing countries, with an increasing incidence rate. Despite this fact, the overall mortality associated with breast cancer has been trending downward over the past decade, mainly due to the screening mammography. 2 Interestingly, not all cancers can be detected with mammography; therefore, a biopsy with adequate diagnostic material, via the least invasive approach, is needed. 3
Ultrasonography (US) has been used in diagnosing breast cancer as it helps to provide interventional guidance of suspicious areas in the breast tissue and the axilla. In patients suspected of having breast cancer, US is proven to be useful (1) to further characterize a mammographically detected lesion or an area of architectural distortion, (2) to differentiate between simple and complex breast cysts, (3) to fortify clinical breast examination findings, (4) to determine the need for a US-guided biopsy, and (5) to measure lesion size before starting chemotherapy and radiation therapy. 4 In addition, perioperative axillary US may be useful in aiding the diagnosis of breast malignancy as well as detecting positive lymph nodes. 5
Flobbe et al. 6 highlighted the importance of adding US to a clinical workup of suspected breast cancer. They studied 2020 patients (470 with a palpable mass) who underwent a clinical breast examination, mammography, and breast US. Adding US helped to detect eight additional malignant cases and corrected 332 diagnostic cases, suspected of malignancy, to a benign diagnosis (predominantly cysts or fibroadenomas). Hence, the main benefit of adding breast US was improved specificity when used in a targeted diagnostic manner.
Patients with suspicious mammography results or a palpable mass, on the clinical examination, should be considered for a biopsy after US findings for a mass or mass-like lesions. A biopsy is also warranted in cases of a suspicious mammogram. An US-guided biopsy is considered the diagnostic preoperative gold standard and can aid in choosing the proper treatment approach. It is important to note that following a biopsy, a hematoma and/or inflammation may develop at the site of the mass. Therefore, this postprocedure development can complicate the clinical assessment. 7
Surgical biopsy should be considered as a last resort in cases where palpation-guided and/or image-guided biopsy is not attainable. Core needle biopsy (CNB) is usually performed under local anesthesia through a small skin incision; careful introduction of the needle is warranted to avoid a potential pneumothorax. 8 The use of a vacuum-assisted CNB provides greater tissue removal compared to a non-vacuum-assisted CNB, and a larger-diameter device will yield a larger volume of tissue. For example, the 8-gauge device yields approximately 245 to 310 mg of tissue per core compared to an 11-gauge device yielding 83 to 116 mg of tissue per core, thereby increasing diagnostic accuracy. 9 The use of ultrasonography-guided core needle biopsy (US-CNB) allows for real-time evaluation of the lesion sampled, and this method is also faster and cost-effective compared to other image-guided biopsy techniques. Image-guided biopsies are also indicated for small, deep, or mobile lesions. Henceforth, fewer samples are required to establish a diagnosis. After biopsy, clip placement is important to mark the biopsy site and to ensure sonographic correlation with a surgical approach. 10 The major drawback in diagnostic accuracy of US-CNB is the failure to visualize the lesion, given the operator dependence, and a need for radiologic correlation. 11
US is proven to be more clinically preferred in breast imaging as an initial bedside investigation, given its many advantages compared to imaging modalities such as magnetic resonance imaging (MRI) and mammogram. US allows for real-time visualization of the lesion and has no added risk of radiation or contrast exposure. Also, US is useful in a situation where other modalities are contraindicated, for example, in patients with metallic prosthesis or pacemakers, and in pregnancy. 12
Hussein et al. 13 looked at the accuracy of US-CNB in detecting breast malignancies. They analyzed 79 patients who underwent US-CNB followed by surgical excision in a Dubai hospital. The sensitivity of US-CNB was 84.9%, with a specificity of 90.9%, which is lower than the international standards. These findings were attributed to the small patient sample that was studied. Thus, the present study was designed to reexamine the sensitivity and specificity compared to previous data and international standards. The study was a continuation of the work by Salem et al. in the same medical center. A secondary aim of the study was to measure the sensitivity and specificity of US-CNB in detecting different types of malignant breast lesions. Based on a search of recently published literature, this research effort was one of the largest studies to originate in the Arabian Gulf region.
Materials and Methods
A retrospective cohort study was conducted in a tertiary hospital in Dubai, UAE, and a patient flow of around 200,000 in 2017. The study inclusion criteria included females older than 13 years who underwent a CNB procedure and cases in which sample histological analysis was completed in the medical center’s laboratory. Cases of breast mass in males, patients younger than 13 years old, and those who were lost to follow-up were excluded from the study. Over the study period, 265 patients have had US-CNB done there. In total, 147 of those patients fulfilled the inclusion criteria. Data for the patients who met the inclusion criteria were extracted from their medical files, as well as their electronic medical records, including (1) patient demographics, (2) symptoms and signs at presentation (including breast mass identification, weight gain or weight loss, areolar and/or nipple changes, menstrual cycle character and/or disturbance), (3) US-CNB result, and (4) histopathological results. All patients who underwent a surgical excision of the lesion, either lumpectomy or mastectomy, also had postoperative histopathologic correlation completed. To maintain the confidentiality of the patients, personal medical information was accessible only to the primary investigator.
Ethical approval was obtained from the institutional ethics committee prior to data collection. Statistical analysis was done using IBM Statistical Package for the Social Sciences (SPSS) software, version 21. Results were presented at a confidence interval of 95%, and a P value of .05 was considered statistically significant. In addition, the sensitivity and specificity of US-CNB results were recorded.
Results
Of the 147 patients included in the study, 109 (74.1%) had a malignant lesion found with a CNB while 38 patients (32.1%) had a benign lesion (see Table 1). The sensitivity and specificity of US-CNB, in detecting a malignancy, were 96.33% and 75.10%, respectively. In the study, the positive predictive value of US-CNB was 92.4%, while the negative predictive value was 87.5%. The most frequently encountered malignant breast lesions were (1) invasive ductal carcinoma and (2) invasive lobular carcinoma (see Figure 1). Conversely, the most frequently encountered benign lesions were (1) fibroadenoma and (2) fat necrosis (see Table 2).
Ultrasound-Guided CNB Sensitivity and Specificity (n = 147).
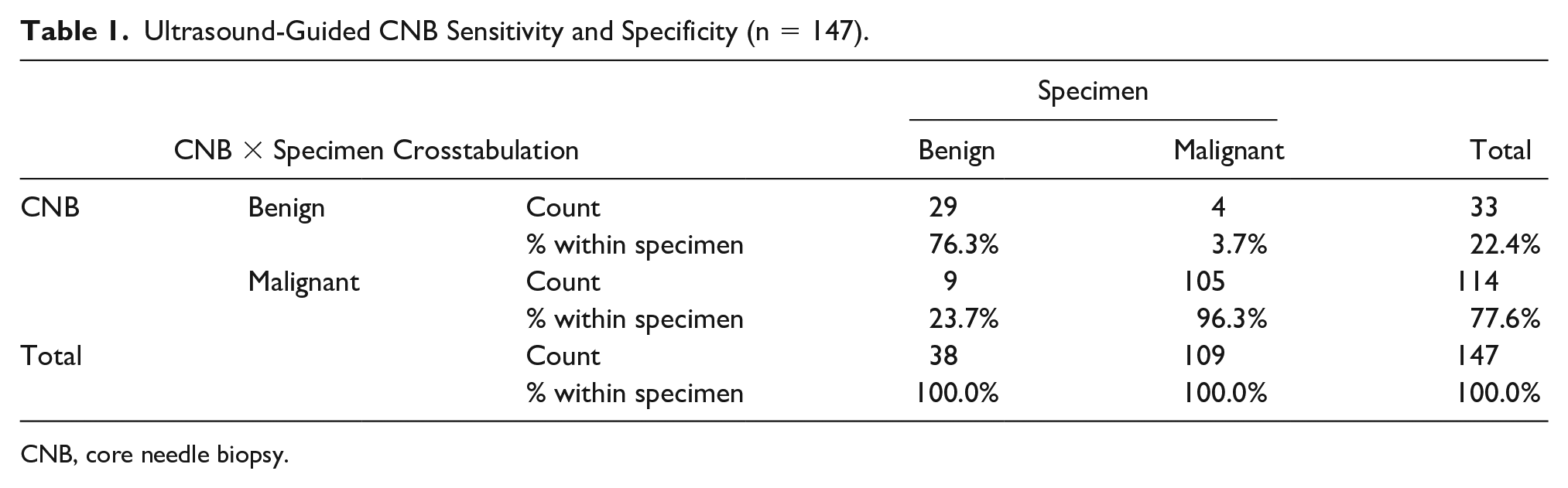
CNB, core needle biopsy.
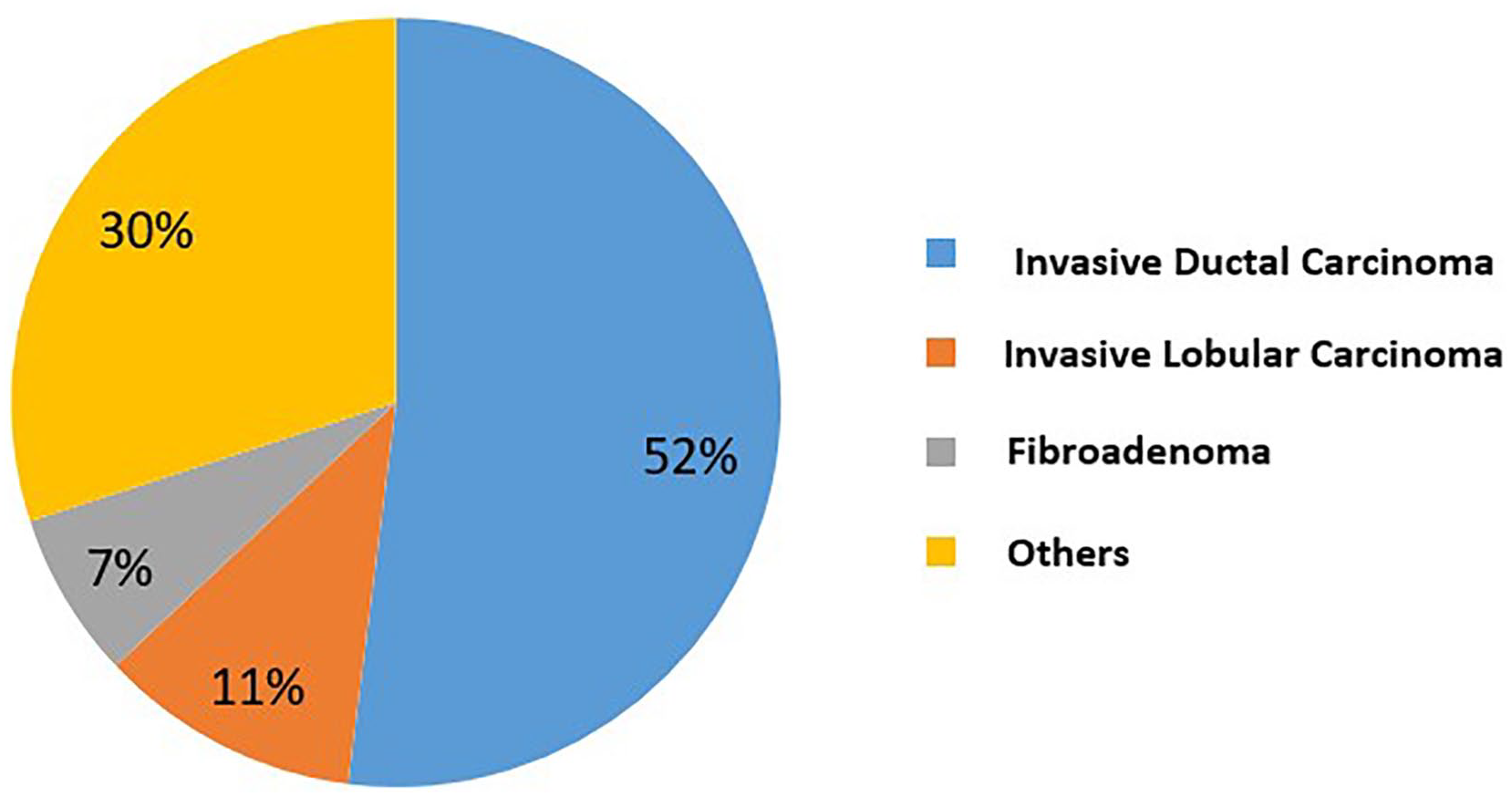
The most common breast lesions found via ultrasonography-guided core needle biopsy (n = 147).
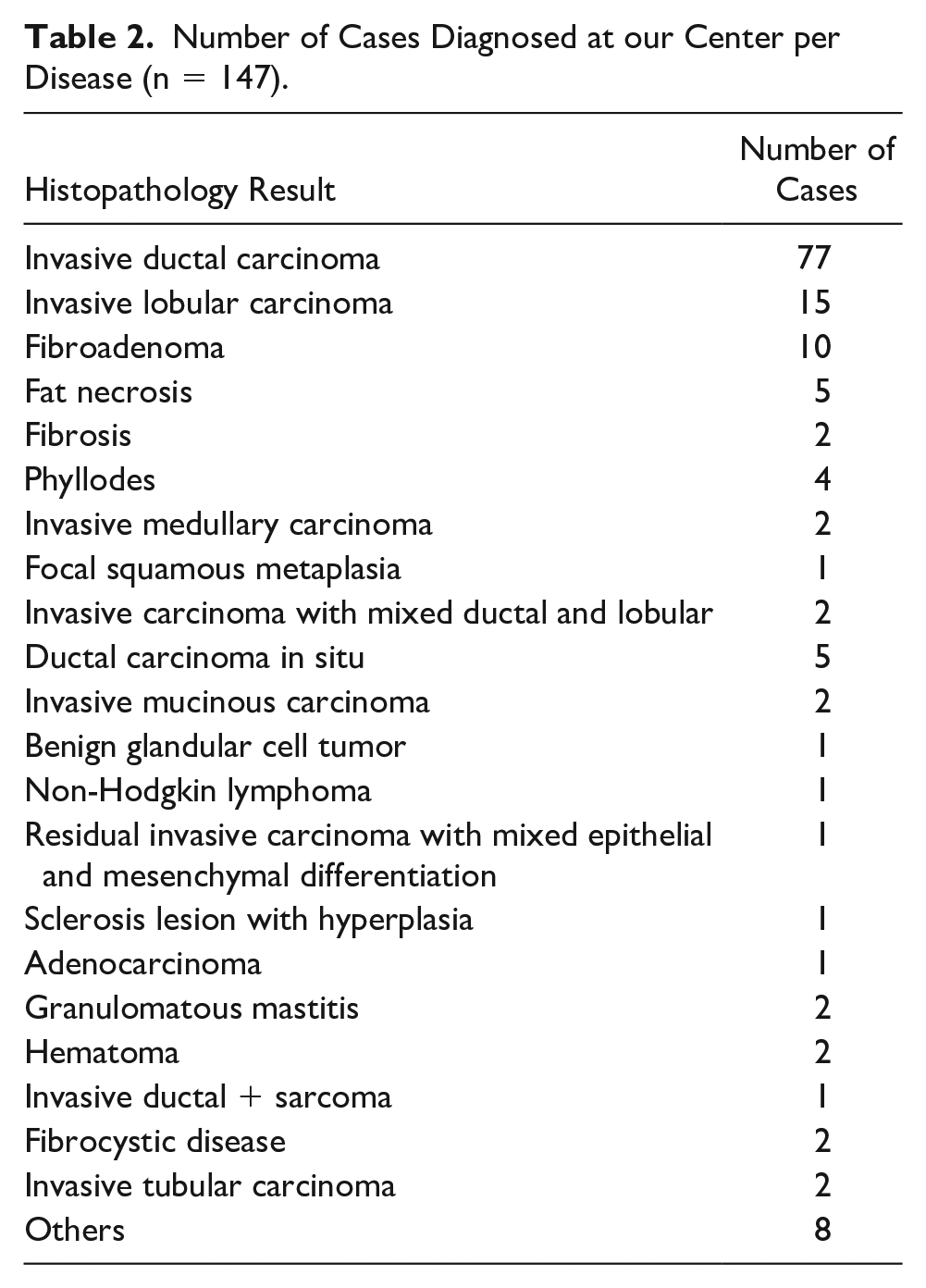
Number of Cases Diagnosed at our Center per Disease (n = 147).
Considering the benefit of US-CNB in detecting some commonly encountered malignant breast lesions, invasive ductal carcinoma was detected with a sensitivity of 81.18% and a specificity of 78.88%. US-CNB detected invasive lobular carcinoma with a sensitivity and specificity of 66.67% and 99.20%, respectively. US-CNB had a sensitivity and specificity of 80% and 98.55%, respectively, in detecting fibroadenoma, and that was the most common benign lesion (see Figure 2). During the study, some infrequently identified breast lesions that were encountered included (1) ductal carcinoma in situ (DCIS) (see Figure 3), (2) non-Hodgkin lymphoma, (3) phyllodes, and (4) invasive mucinous carcinoma.
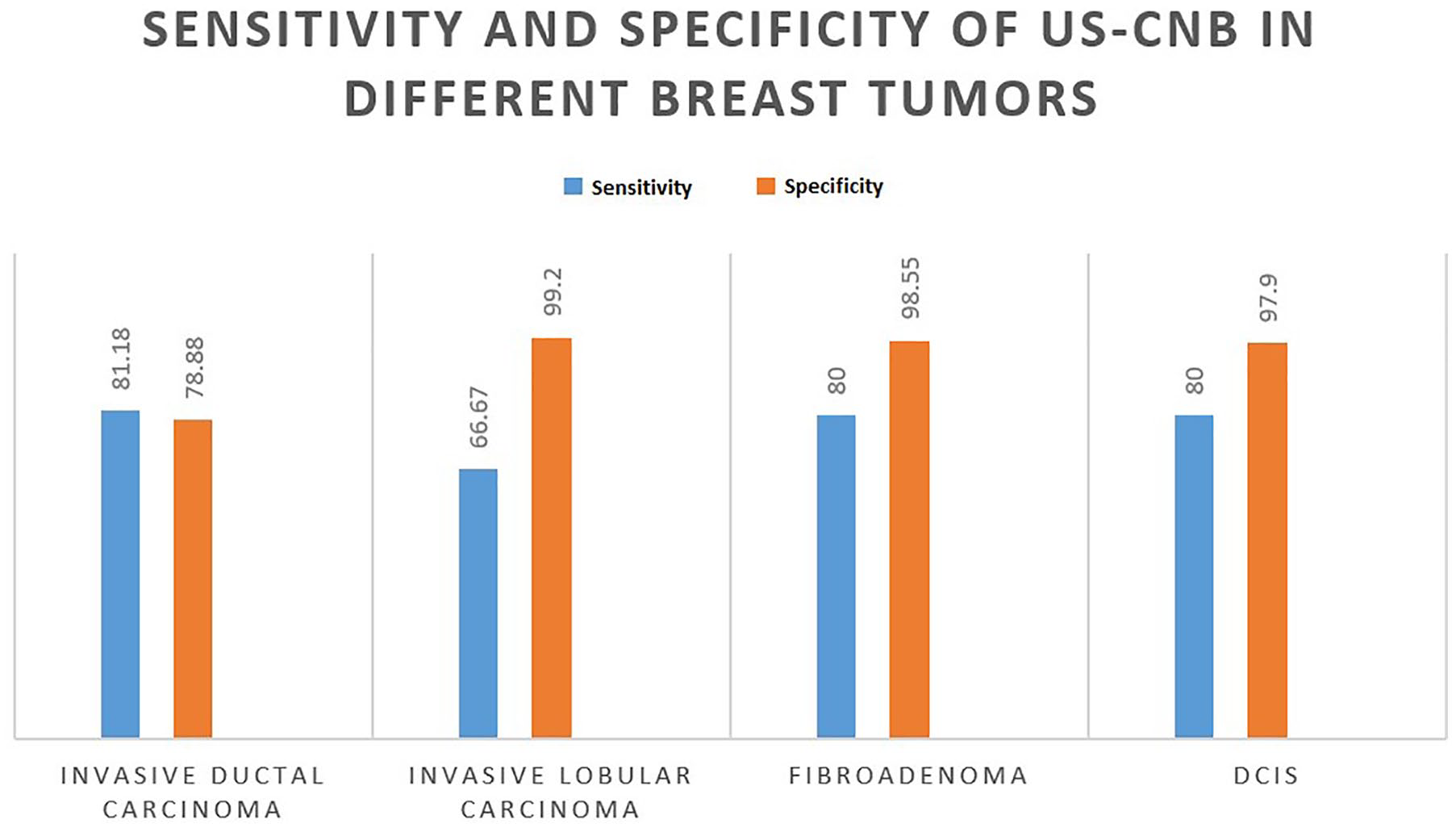
Ultrasonography-guided core needle biopsy sensitivity and specificity for most common breast lesions at the study hospital.
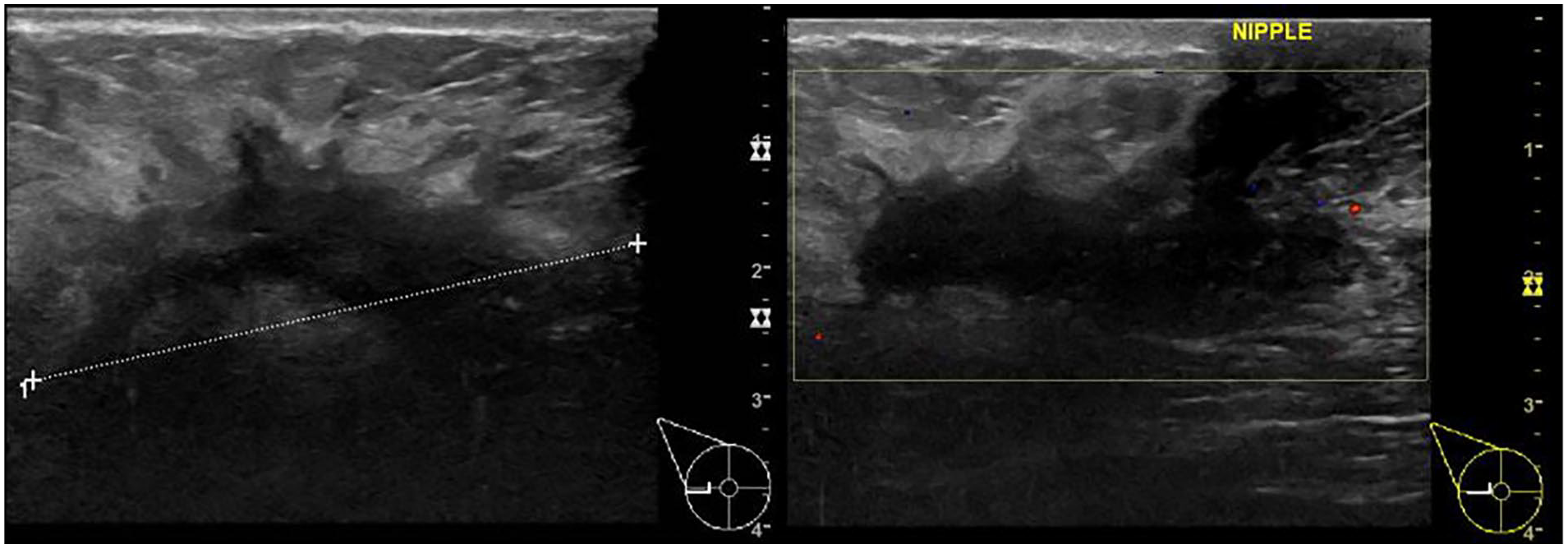
A breast ultrasonography image showing a large highly suspicious lesion associated with right axillary lymphadenopathy on physical examination, which was found to be ductal carcinoma in situ on histopathological examination after ultrasonography-guided core needle biopsy.
Four patient cases that had a cancer diagnosis were missed by the initial pathologist report, based on the final histopathology specimen. In this subgroup of cases, two patients had malignant phyllodes tumors that were reported as fibroadenoma, based on the CNB specimen. However, in these patients, the final surgical specimen was determined to be a phyllodes tumor. Phyllodes tumors are uncommon fibroepithelial breast tumors and are capable of a diverse range of biologic behaviors. Two other patient cases were identified as an invasive ductal carcinoma and adenocarcinoma (see Figure 4). Both of these lesions were misdiagnosed as DCIS and chronic perivascular inflammation, respectively.
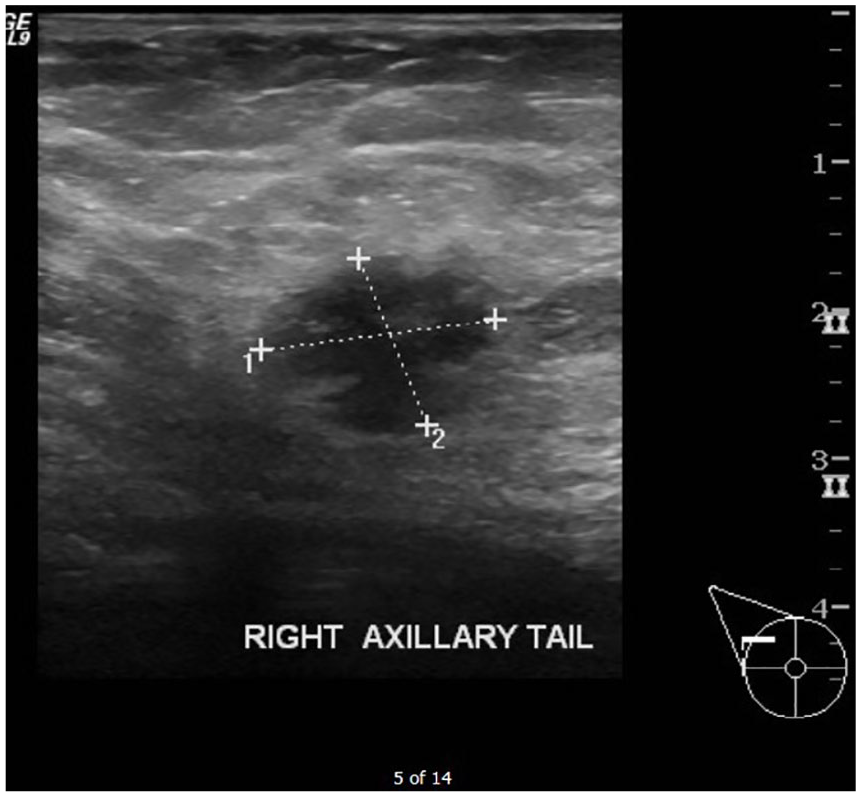
A breast ultrasonography image showing a hypodense lesion that was found to be invasive ductal carcinoma on ultrasonography-guided core needle biopsy.
Discussion
Although screening mammography helped to decrease the incidence of mortality, related to an early identification and treatment of breast cancer, there remained an inability to identify all the specific types of lesion. In addition, the type of breast tissue density does affect mammogram quality. 14 Thus, recently, US-CNB has been used to confirm mammographic findings and increased the overall outcomes for these patients. 15
Despite recent advances in breast imaging, tissue sampling remains the best method to confirm the presence a malignant or benign lesion. 16 There are also a variety of benign lesions that resemble a malignancy with breast imaging modalities, such as mammography (e.g., tomosynthesis, contrast-enhanced mammography), US, and MRI. These imaging modalities can help detect and diagnose palpable and nonpalpable breast lesions. Over the years, these imaging modalities have improved patient management and aided in avoiding an unwarranted surgical biopsy of a benign lesion.17,18
Zhang et al. 19 studied 339 patient cases with US-CNB of breast masses. They concluded that the negative predictive value, in their sample, was 99.40%, with two false-negative cases. 19 The authors recommended pathology be correlated with radiologic findings, to avoid delaying a carcinoma diagnosis. In addition, Prutki et al. 20 looked at the usefulness of CNB, as a diagnostic tool, for suspicious breast lesions followed by surgical excision and histopathological validation of CNB results. They found US-CNB to be 98% accurate in diagnosing the type of lesion. Wiratkapun et al. 21 did a retrospective analysis of 733 patient cases that underwent either US-CNB or had a minor surgical specimen removed. They concluded that US-CNB had a good diagnostic yield and can be used instead of the minor surgical specimen. Fan et al. 22 reviewed 2152 patient cases with suspicious breast masses that were either investigated with US-guided biopsy or a palpation-guided biopsy. 22 They found a lower false-negative rate, a higher sensitivity, and specificity using US-CNB. The authors reported a false-negative rate of US-CNB (2.10%, 22/1068), which was lower when compared to freehand-guided CNB (7.40%, 29/393) (P < 0.05). This might have been due to the variability among physicians and their level of expertise for performing the palpation-guided biopsy.
The current study results are consistent with previously published studies and comply with international guidelines with regard to the sensitivity and specificity of US-CNB in the diagnosis of breast masses. This study helps to illustrate that breast US plays a pivotal role in the diagnosing of breast lesions. It is also important to make sure that US diagnoses have a pathology-radiologic correlation (see Figure 5).4,23
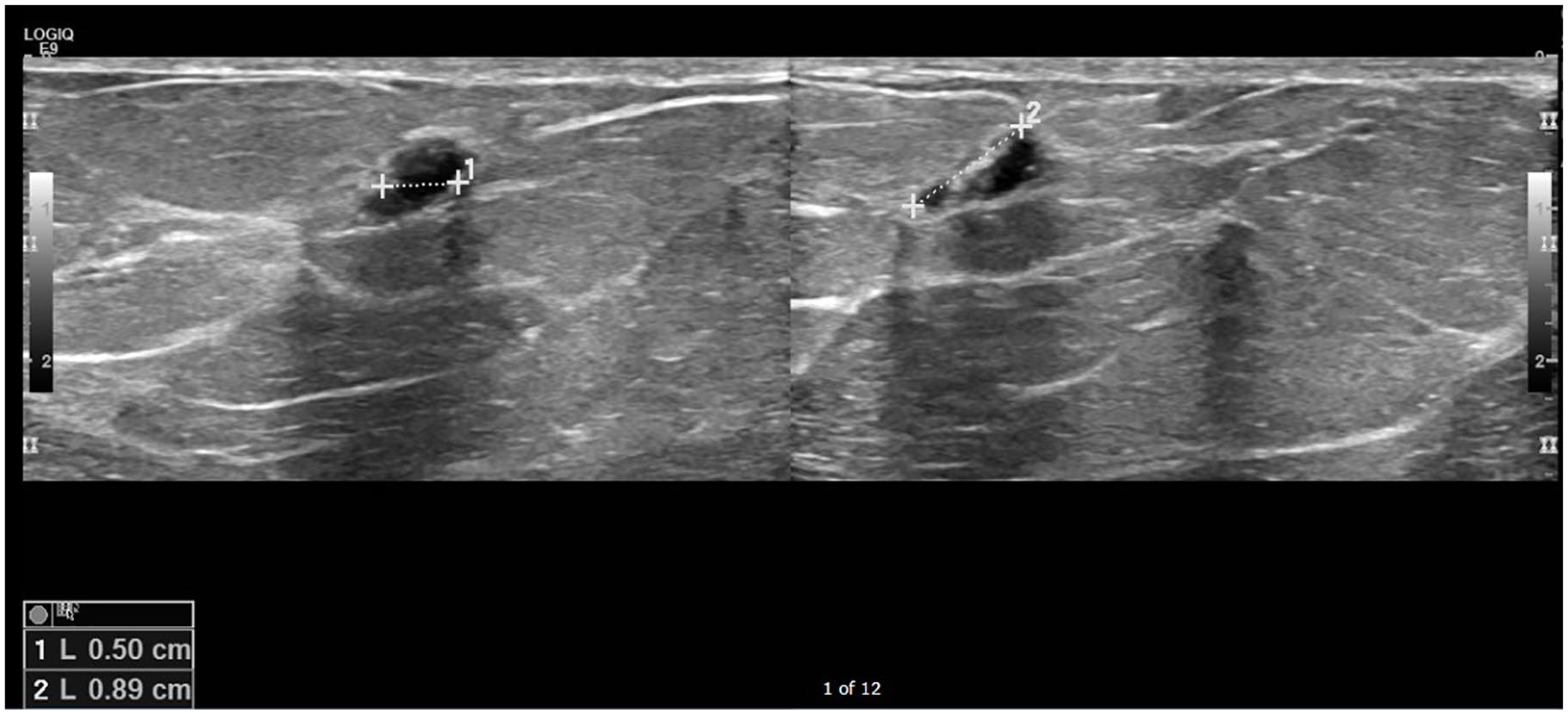
A breast ultrasonography image of a 51-year-old woman with a history of a painful breast lump that showed to be small cystic fluid-filled lesion.
Conclusion
The subtypes of breast malignancies encountered during the study period included invasive ductal carcinoma as the most common subtype, followed by invasive lobular carcinoma, while the most frequent benign breast lesion was fibroadenoma. During the study period, some of the rare subtypes of breast cancer were encountered, including non-Hodgkin lymphoma and invasive mucinous carcinoma.
Among the notable reasons for missing malignancies with CNB include an inadequate number of biopsies and operator experience with handling the ultrasound machine. US-CNB proved to have an incremental role in the diagnosis and management of breast lesions in this cohort with the proper radiologic correlation to histopathologic findings. An additional factor is that US is a user-dependent imaging modality; therefore, careful interpretation of results is warranted, especially in situations with difficult assessments or with limited experience users. These cohort findings showed similar rates of sensitivity and specificity when compared to international standards and reported results worldwide.
Given that these study results were limited to one institution, institutional guidelines and scope of practice might be different across institutions. US is a user-dependent imaging modality; therefore, human error in conducting a guided procedure can be mitigated but not fully omitted. This work was built on previously published institutional work; therefore, these findings should be compared with other institutions to gain a better understand of their epidemiology and practice using US-CNB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.