
Abstract
Intraparenchymal hemorrhage, also known as grade IV hemorrhage, is a severe and uncommon type of intracranial hemorrhage. Intraparenchymal hemorrhage is associated with poor clinical outcomes; therefore, recognition and differentiation of the correct type of intracranial hemorrhage is important for the treatment of the patient. This case report demonstrates the use of real-time sonographic imaging in a preterm neonate as an effective method of diagnosing intraparenchymal hemorrhage and demonstrates a possible presence of fungemia.
Introduction
Premature infants of less than 1500 g are inclined to present more commonly with intracranial hemorrhage and are at increased risk for fungal infections. Intraparenchymal hemorrhage (IPH) in conjunction with intraventricular hemorrhage is generally categorized as a grade IV hemorrhage and is associated with increased infant mortality. 1 Intraparenchymal hemorrhage is usually hyperechoic on sonograms; however, over time its appearance becomes hypoechoic.2–4 Cranial sonography is highly accurate in indicating the presence and the severity of intracerebral hemorrhagic lesions. 5 Early recognition of parenchymal involvement may offer different treatment options to improve neonatal neurodevelopmental outcome.4,5
Case Report
A male child was born at a gestational age of 25 weeks and 3 days with a birth weight of 705 g. The infant presented with agonal respirations, pale skin color, and Apgar scores of 3 and 4. He was intubated in the delivery room because of poor respiratory effort. Shortly afterward, he was admitted and transported in an open warmer to the neonatal intensive care unit for further monitoring and treatment. Antibiotic treatment was prescribed upon admission and continued for 7 days. Antibiotic treatment was replaced by a cardioactive agent when pulmonary hemorrhage arose, and packed red blood cells were administered because of a low hematocrit level. He continued to have an elevated prothrombin time, low platelets, and a low hematocrit, requiring intermittent transfusions of fresh frozen plasma.
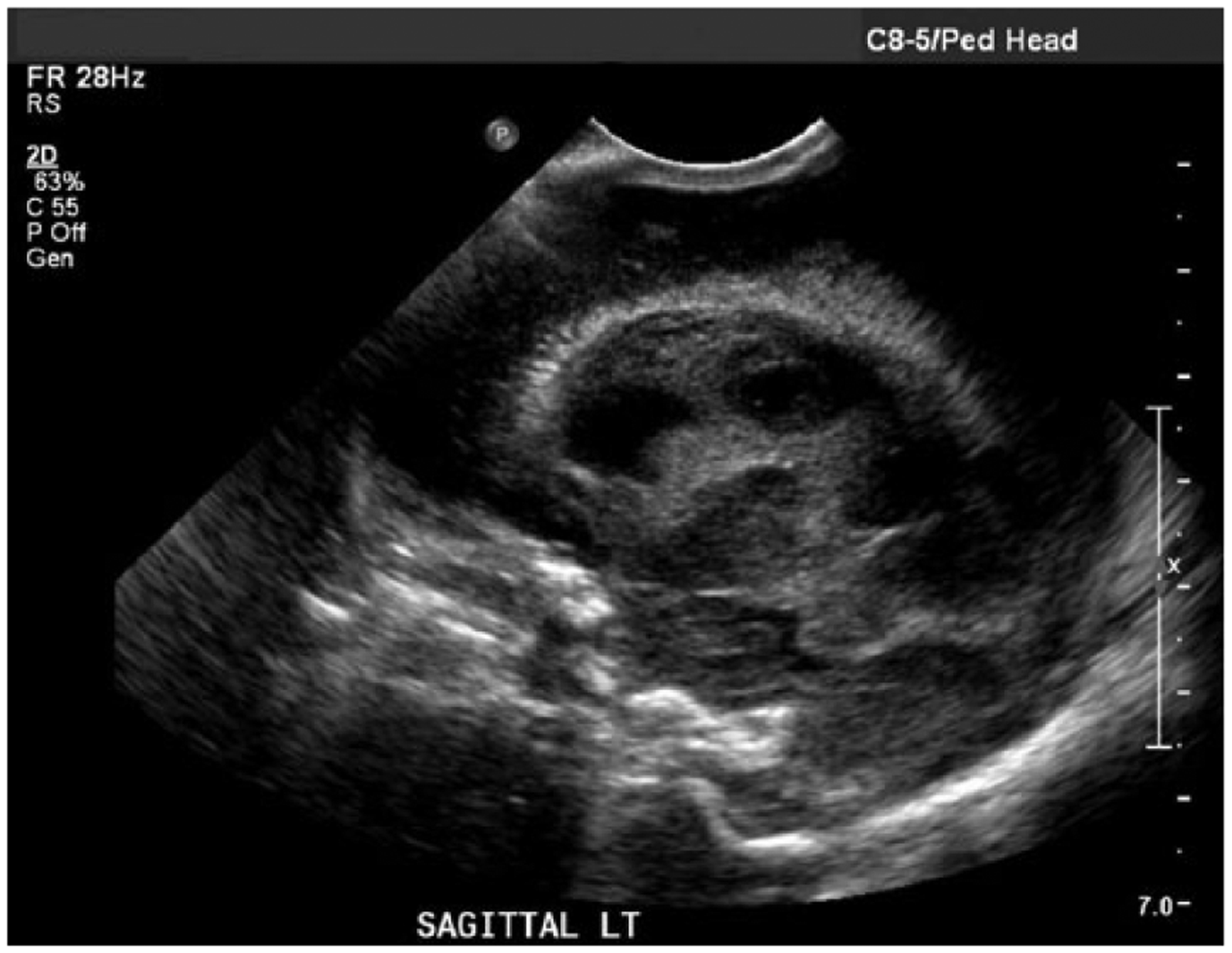
A transcranial sonogram was ordered to evaluate brain structures when intracranial hemorrhage became a concern. The sonogram was performed using a Philips iU-22 ultrasound system (Philips Medical, Bothell, Washington, USA) with a 8-5 MHz curvilinear transducer and a 12-5 MHz linear transducer. Sonography showed bilateral grade IV hemorrhage with enlarged ventricles, left IPH, and a slight midline shift from left to right. A repeat sonogram was performed on the next day and showed increased parenchymal hemorrhage with midline shift and severe hydrocephalus of the entire ventricular system (Figures 1 and 2). Five days later, another sonogram showed bilateral grade IV intracranial hemorrhage with evolving clot in the left lateral ventricle. Ventriculomegaly and blood in the third and fourth ventricle, along with multiple echogenic areas throughout the brain parenchyma, were also noted (Figures 3, 4, and 5).
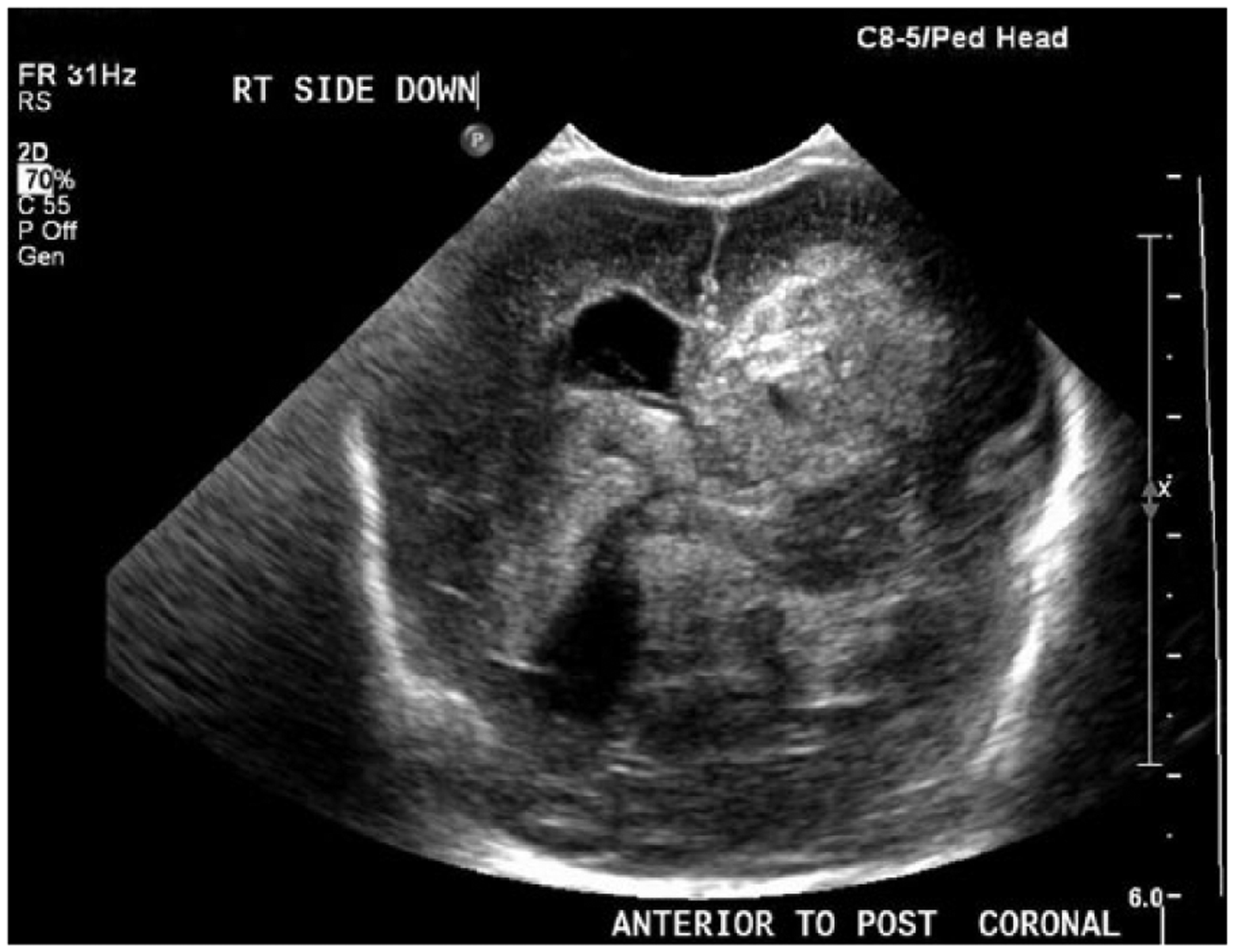
Gray-scale coronal image of the neonate’s brain showing brightly echogenic intraparenchymal and intraventricular hemorrhage on day three of life.

Gray-scale sagittal image of left side of the neonate’s brain showing brightly echogenic intraparenchymal and intraventricular hemorrhage on day three of life.

Gray-scale coronal image of the neonate’s brain showing mixed hypoechoic and anechoic intraventricular and intraparenchymal hemorrhage on day eight of life (compare to Figure 1).
Gray-scale sagittal image of left side of the neonate’s brain showing mixed hypoechoic and anechoic intraventricular and intraparenchymal hemorrhage on day eight of life (compare to Figure 2).
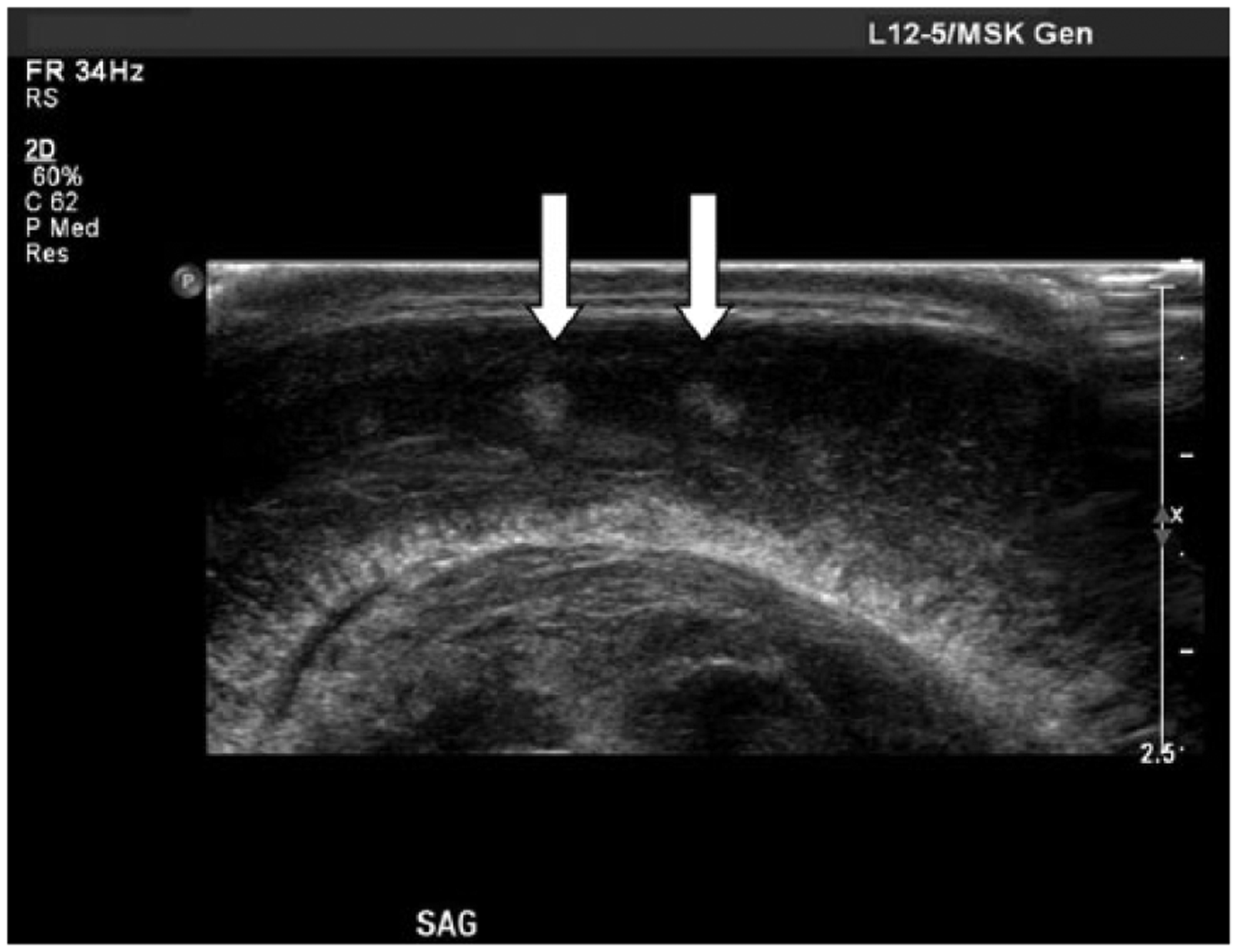
Gray-scale sagittal image of the neonate’s brain showing echogenic areas (arrows) corresponding to possible microabscesses throughout the brain parenchyma on day eight of life.
Concern for possible seizures and the findings on the transcranial sonogram along with the baby’s development of decerebrate posturing prompted the neonatologist to recommend electroencephalography (EEG). The EEG showed flattening with definitive presence of seizures, prompting initiation of a barbiturate. The baby’s clinical status started to worsen during the eighth day of life with bradycardia, desaturation, and abdominal duskiness. On the thirteenth day of life, the baby’s blood culture came back positive for Candidiasis albicans fungemia. Antifungal treatment was started immediately. Because of the presence of fungemia, bilateral grade IV hemorrhage, seizures, respiratory distress, and intestinal ischemia, the overall prognosis was poor and the family elected to withdraw care. An autopsy was declined; therefore, no further follow-up was available.
Discussion
The majority of structural lesions associated with the central nervous system in premature neonates are some type of cerebral hemorrhage. Cerebral hemorrhage, also known as intracranial hemorrhage, consists of germinal matrix hemorrhage, intraventricular hemorrhage, and IPH. 1 The most common type of intracranial hemorrhage is found within the germinal matrix. 6 A grading system was developed by Burstein et al., based on computed tomographic (CT) and sonographic findings, to classify the severity and extent of cerebral hemorrhage.6,7 This system categorizes grade I hemorrhage as being isolated to the germinal matrix, grade II as intraventricular hemorrhage without ventricular dilation, grade III as intraventricular hemorrhage with ventricular dilation, and grade IV as intraventricular hemorrhage extending into the surrounding cerebral parenchyma. 6
Grade IV hemorrhage, or IPH, is the most severe type of intracranial hemorrhage, accounting for 11% to 26% of all cerebral hemorrhages. 1 The sonographic appearance of IPH is usually echogenic in the early stages but may become more echolucent over time. Because of clot retraction and liquefaction over a prolonged time, the intracranial hemorrhage sonographic appearance becomes more hypoechoic or even anechoic.7,8 The degree of the hemorrhage also may cause midline shift, along with depression of the sylvian fissure.8,9 Intraparenchymal hemorrhage has a mortality rate of 25% to 69%. 9
Cerebral circulation, neurovascular integrity, and coagulation problems may lead to intracranial hemorrhage in preterm newborns, although perinatal asphyxia and birth trauma are more critical. Fetal intracranial hemorrhage may be seen in utero and is often associated with placental abruption and intrauterine growth restriction. 10 Grade IV hemorrhage can lead to coagulation disorders, increased intracranial pressure, and developmental and neurologic problems.6,11 The treatment of premature infants weighing less than 1500 g with intracranial hemorrhage consists of assisted ventilation, anticonvulsants to control seizures, and blood transfusions if hemoglobin levels are too low.
Fungemia, more commonly known as candidemia or candidiasis, is a fungal infection characterized by the presence of yeast in the blood that may involve brain, eyes, lungs, liver, spleen, kidneys, bones, and joints. 3 Prolonged use of antibiotics, steroids, and invasive medical procedures such as venous catheterization may also be the cause of fungemia in neonates. 3 C albicans is an uncommon disease that is known to have a high morbidity and mortality; it is the most common type of candidiasis in premature infants weighing less than 1500 g at birth.3,4 The mortality rate is between 40% and 50% in infants born before 26 weeks gestation, with a birth weight of 1000 g or less. 11
Amphotericin B or fluconazole are typically used as therapy for C albicans.4,11 Depending on the severity of candidiasis, the length of treatment usually varies from four to six weeks. 11 Echogenic microabscesses scattered throughout the brain parenchyma may be shown by cranial sonography. These may appear as punctuate calcified lesions in the brain parenchyma. Periventricular calcifications and hydrocephalus with echogenic debris have also been reported. 11 Candidal infection may have a considerable effect on the neurodevelopmental outcome of neonates. Premature newborns with parenchymal candidal association tend to have poor prognosis as opposed to those with just ventricular involvement. 4
Conclusion
Intraparenchymal hemorrhage and C albicans have a poor prognosis in very low birth weight premature infants; therefore, the recognition of intracranial hemorrhage type and early detection of fungal infection have important clinical effects. Although sonography cannot diagnose candidiasis, it can detect echogenic areas in the brain parenchyma that may aid in the proper diagnosis. Sonography is the initial imaging modality used to differentiate grades of intracranial hemorrhage in preterm neonates.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.