
Abstract
Glenohumeral (GH) dislocations of the shoulder are prevalent in young male subjects and appear to be increasing in incidence. The classic diagnostic evaluation of labral injuries such as this involves the use of clinical testing as well as imaging modalities such as computed tomography, magnetic resonance imaging, and radiography, none of which provides a dynamic evaluation. This study was done to replicate sonographic evaluation of the glenoid labrum in a preclinical model and use the axillary scanning approach to specifically assess the integrity of the anterior inferior labrum. Using sonographic guidance, minimal amounts of differently colored dyes were injected into regions of the glenoid labrum. This replication was able to image only the posterior superior, posterior inferior, and anterior inferior aspects of the GH labrum. Bankart lesions were identified in two shoulders, confirmed on dissection. The presence of dyes in the target areas within and around the labrum was visually confirmed. These findings suggest that the concept of using an axillary scanning approach for detecting labral tears and Bankart lesions in patients with acute and chronic shoulder dislocation may be worthwhile to incorporate into a shoulder-scanning protocol.
Glenohumeral (GH) dislocations of the shoulder are believed to occur at a rate of 23.9 per 100,000 person-years, nearly twice the previously reported incidence. 1 Ninety percent of GH dislocations are classified as projecting anteriorly. 2 This occurs when the humeral head is located inferiorly and under the glenoid fossa. Posterior GH dislocations are the next most common type of classification. 2 Dislocations in the superior or inferior direction are very uncommon. Given the upswing in this type of dislocation and its prevalence in young male subjects, 1 it would seem imperative to find high-quality imaging choices to diagnose GH dislocations and treat them promptly.
The GH joint (GHJ), which is the site of dislocation, is composed of the scapular glenoid and the humeral head (Figure 1). The humeral head is much larger than the glenoid, and this incongruity between the two articulating surfaces contributes to shoulder mobility but also reduces stability. 3 A fibrocartilaginous rim known as the labrum surrounds the glenoid cavity and helps improve GHJ stability and restrict anterior and posterior excursions of the humerus by deepening the glenoid socket.4,5 The extreme forces generated during overhead activities may cause dislocation and associated labral injuries because of its close relationship with the glenoid cavity and humeral head. 6 A fracture of the anteroinferior rim of the glenoid, or an avulsion of the labrum from the rim, is called a Bankart fracture. Additionally, any fibrocartilaginous damage that does not involve the bone is referred to as a Bankart lesion. 2 Bankart pathology is associated with GH dislocations that disrupt the GHJ anteriorly. These acute dislocations and associated pathology are highly likely to recur. The current estimate is that 90% of 20-year-old athletes, up to 60% of adults at 30 years of age, and 15% of 40-year-olds are at risk for recurrent GH dislocation. 2 These are seen largely in individuals who participate in repetitive and/or forceful overhead arm movements. Superior labral tears from anterior to posterior (SLAP tears) are associated with dislocations and can even extend into the biceps tendon. Because GH dislocations are so prevalent, diagnostic tools are needed to diagnose acute trauma to the GHJ and to provide surveillance for recurrence. Most patients experience secondary GH injuries up to 2 years after surgical repair, and therefore repeat imaging is equally important.
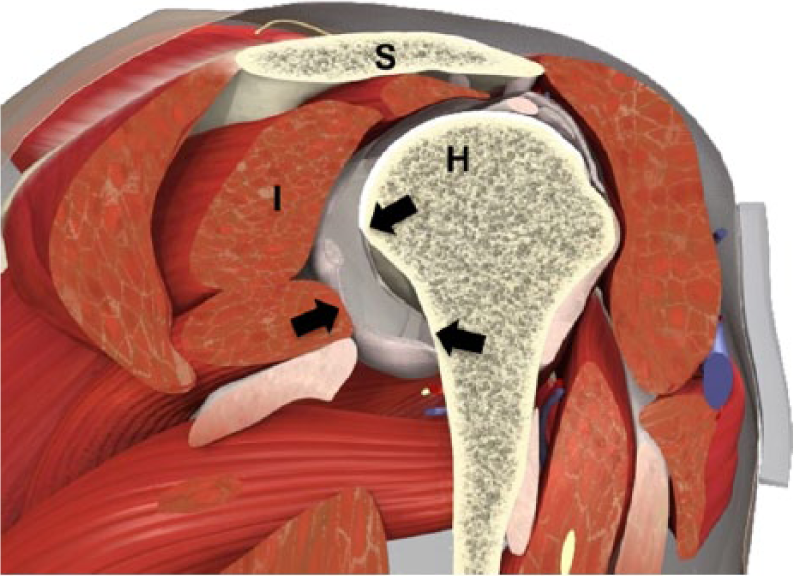
Anatomic diagram of the glenohumeral joint in an oblique sagittal view. H, head of humerus; I, infraspinatus; S, scapula (acromion). Black arrows indicate the glenoid labrum. (Permission obtained from © Primal Pictures.)
The classic diagnostic evaluation of labral injuries involves the use of clinical testing as well as imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI), and radiography. These imaging choices can be expensive and difficult to use for surveillance, but most of all, they lack the ability to provide a dynamic evaluation of the joint. Diagnostic medical sonography (DMS) is a promising alternative imaging modality that is relatively inexpensive, provides dynamic evaluation, and can be repeatedly used for follow-up evaluations. DMS provides diagnostic information on rotator cuff tears, but only a few studies have explored its use in detecting Bankart lesions. 7 Furthermore, more scientific evidence is needed to demonstrate the efficacy of DMS in the evaluation of the anterior GHJ. The purpose of this study was to replicate diagnostic medical sonographic evaluation of the glenoid labrum in a preclinical model and use the axillary scanning approach to specifically assess the integrity of the anterior inferior labrum.
Methods
This study was exempt from institutional review board approval under category 4 of The Ohio State University institutional review board exemption categories (the collection of data on existing pathologic specimens that were deidentified to the investigator). A clockwise approach to classifying the anatomic areas of the glenoid labrum was used to ensure that labral tears could be determined from normal variants.8,9 Four regions of the glenoid labrum were chosen for scanning: posterior superior, posterior inferior, anterior superior, and anterior inferior or axillary. These regions correspond to 9 to 11 o’clock, 6 to 9 o’clock, 1 to 3 o’clock, and 3 to 6 o’clock, respectively, using the glenoid as a clock face (Figure 2). Bankart lesions tend to occur with inferior GH dislocation and tears that typically occur at 3 to 6 o’clock. SLAP tears are located from the 10 o’clock to the 2 o’clock position and can be associated with posterior GH dislocation.8 -10
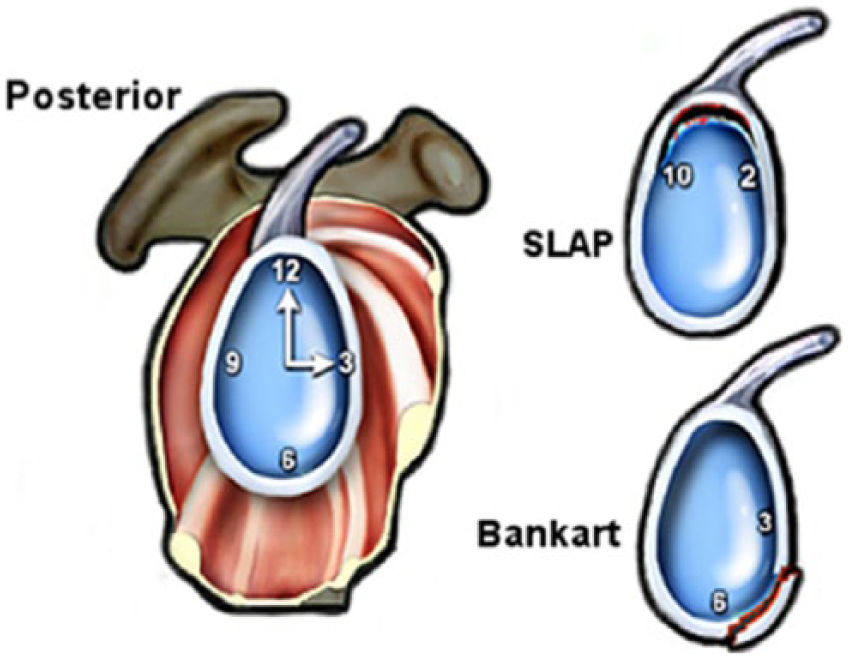
A coronal clock-face diagram used to indicate the regions of the glenoid labrum. The areas of 3 to 6 o’clock represent the anterior inferior region or axillary area, 6 to 9 o’clock the posterior inferior region, and 9 to 11 o’clock the posterior superior region. Bankart lesions tend to occur with the glenohumeral (GH) dislocation inferiorly with tears that typically occur at 3 to 6 o’clock. Superior labral tears from anterior to posterior (SLAP tears) are located from the 10 o’clock to the 2 o’clock position and can be associated with posterior GH dislocation.
A preclinical study was reported by Taljanovic et al. 11 in 2000, providing proof of concept that DMS of the shoulder could be used to evaluate the GHJ and labrum. Those investigators used arthroscopic evaluation of the glenoid labrum as the gold standard. Given the age of that study, improved technology with DMS should increase the ability to evaluate the labrum for tears that are located posteriorly and, more important, at anterior and inferior locations. To stage this replication of Taljanovic et al.’s study, cadavers were used for standardization of the scanning technique.
Specimens
Four fresh postmortem human surrogates (PMHSs) ranging in age from 76 to 95 years were stored at temperatures between 34°F and 36°F and diagnostically tested within the first 48 hours of receiving the donor body. The four PMHSs yielded eight possible shoulders for imaging and dissection. Two shoulders were excluded from the study because of known rotator cuff tears and histories of shoulder replacement surgery. The study was conducted on the six available shoulders (two male and four female). When the laboratory was not immediately available for testing, PMHSs were frozen to −20°F and thawed 12 hours prior to the experiment. Before testing, the GHJ of each PMHS was preconditioned by taking the arm through its full range of motion in internal rotation, external rotation, and abduction. 10
Ultrasound Scanning Protocol
Each PMHS was scanned using a GE Logiq 9 (GE Healthcare) by two researchers. A 9-MHz broadband linear probe was selected, using a transmit frequency of 8 MHz. The time-gain compensation was adjusted to optimize imaging of the labrum. Overall gain was set to 36, and tissue harmonic imaging with spatial compounding technology was used. All images were saved to the system’s hard drive for later analysis. Taljanovic et al.’s 11 scanning protocol was followed and covered the four regions specified above. The axillary scanning approach, as described by Sugimoto, 7 was used to evaluate the anterior inferior portion of the GH labrum.
Four regions of the GH labrum were scanned: posterior superior, posterior inferior, anterior superior, and anterior inferior (axillary). All scans were performed in the long axis to include the glenoid, labrum, and humeral head. The posterior GH labrum was always imaged first, with the PMHS in a sitting position, arms at the side, and the shoulder in neutral rotation. The axillary location for evaluation of the anterior inferior portion of the GH labrum was not accessible in this position; therefore, the cadavers were repositioned in the supine position with the arm abducted and the shoulder in maximum external rotation. This particular position of the arm is commonly used for vascular imaging of the axillary artery and vein.
Posterior scan
The scanning session started by identifying the acoustic shadow of acromion. The transducer was then moved slightly inferior so that the glenoid, labrum, and humeral head were visible on the sonogram. The posterior superior labrum was identified as a triangular hyperechogenic structure just lateral to the glenoid (Figure 3). The identity of the labrum was confirmed by observing the shape change during dynamic internal rotation of the shoulder. Following the posterior superior scan, the transducer was moved inferior and angled approximately 30° superior from the horizontal to image the posterior inferior labrum (Figure 4). This scanning maneuver produced the best-quality visualization of the posterior-inferior labrum for this particular study.
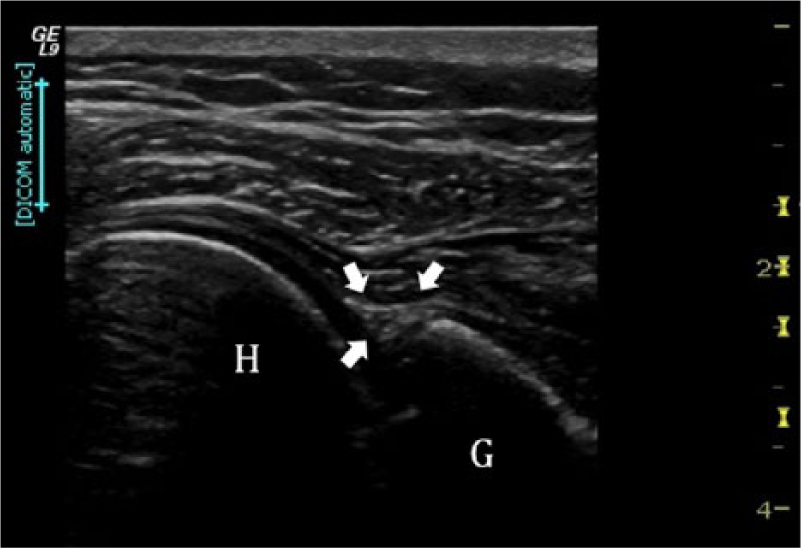
Transverse view of the posterior superior portion of the labrum (arrows) as identified by the triangular echogenic structure just lateral to the glenoid. G, glenoid; H, head of humerus.
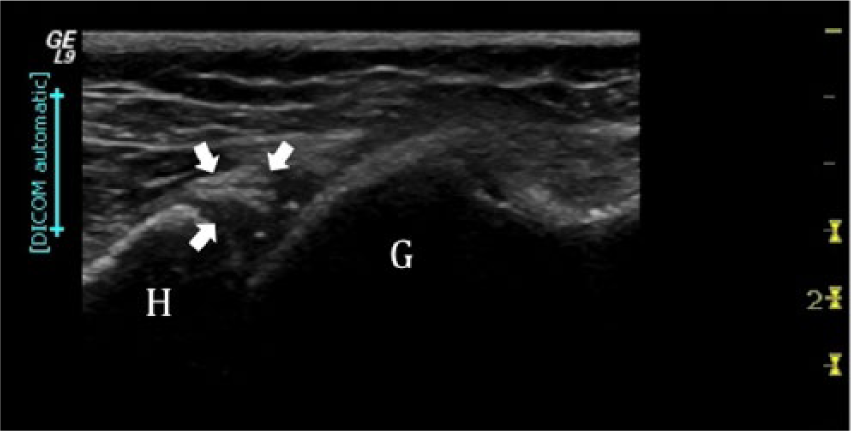
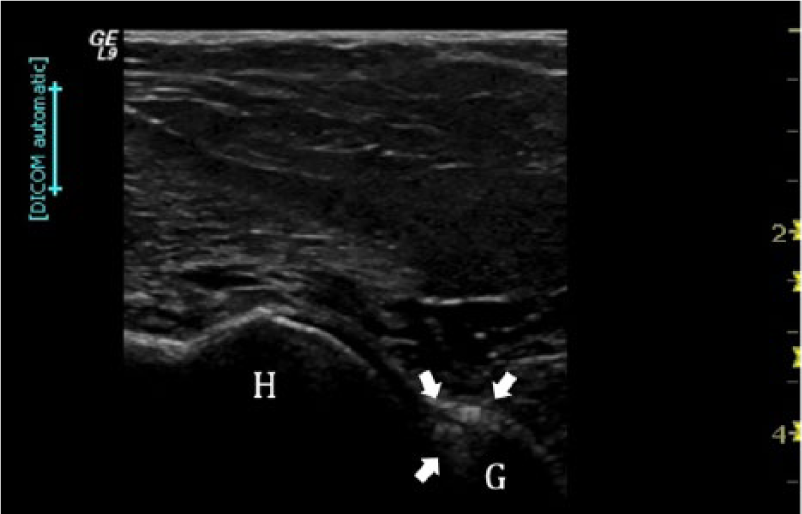
Transverse view of the posterior inferior portion of the labrum (arrows) as identified by the triangular echogenic structure just lateral to the glenoid. G, glenoid; H, humerus.
Axillary scan
Scanning began with the transducer directed along the humeral shaft and then slowly moved medially until the humeral head, labrum, and glenoid were observed on the image (Figure 5). The transducer was placed just lateral to the GHJ to visualize the humeral shaft and then moved medially from that point until the echogenic glenoid bone and the triangular labrum was observed. Anecdotally, tilting the transducer beam and head slightly superior consistently improved the image quality. Using a slightly different technique than Sugimoto, 7 the transducer beam was fanned from 3 o’clock to 7 o’clock to fully evaluate the anterior inferior labral tissue.
Transverse view of the anterior inferior portion of the labrum (arrows) as imaged through the axilla and identified by the triangular echogenic structure just lateral to the glenoid. G, glenoid; H, humerus.
The anterior superior labrum could not be consistently imaged, and a scanning protocol for this region could not be established. For this reason, imaging of the anterior superior portion of the labrum was not done for the remainder of the study.
DMS-Guided Injection and Dissection
In an early clinical study, Schydlowsky et al. 12 used cadaver injections and dissection as their validation method. This methodology was replicated by one of the authors (K.D.E.) with 35 years of experience in DMS. Minimal amounts (<1 mL) of differently colored dyes were injected under sonographic guidance using a spinal needle (20 gauge) into regions of the glenoid labrum. Diagnostic medical sonographic images were obtained as described, and the needle was introduced laterally, angled between 30° and 45° with the long axis of the probe (Figure 6). Once the location of the needle in the labrum was confirmed using real-time imaging, the researcher injected dyes into the labrum. The investigator also pushed the needle against the labrum to indent the structure during real-time observation.
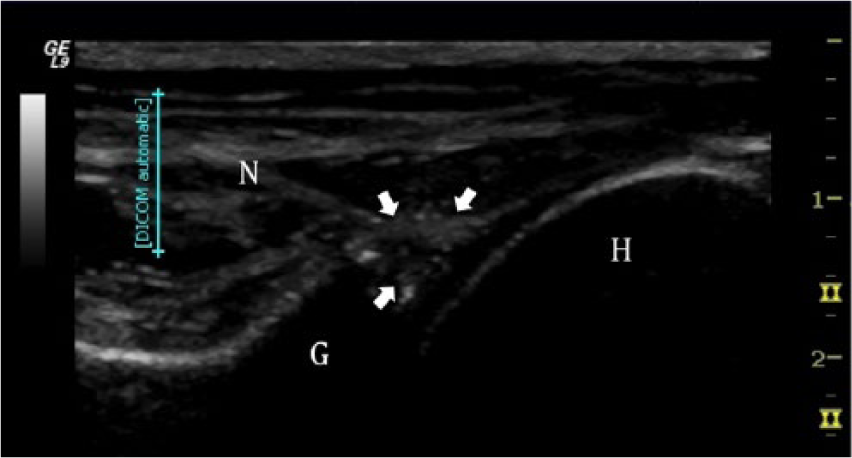
Sonographically guided injections were used to inject the labrum (arrows) with dye, allowing it to be identified during dissection. G, glenoid; H, head of humerus; N, needle.
After the dye injection, dissection of the GHJ was done. Dissection included reflecting the skin, posterior deltoid, infraspinatus, and teres minor (Figure 7). The posterior capsule was reflected by sharp dissection from its attachment on the glenoid to expose the labrum. Once the GHJ labrum was exposed, the presence of colored dyes was visually confirmed and documented (Figure 8). The labrum was then detached from the glenoid cavity using sharp dissection, and the superior side was measured (Figure 9). The length of the labrum was defined as the length from the lateral lip of the labrum to the medial tip along a path that would be consistent with the direction of the ultrasound beam. This measurement was recorded as the actual labral length and was used as the gold standard for comparison with the sonographic measurements.

During dissection, the skin, posterior deltoid, infraspinatus, and teres minor were reflected to expose the capsule and glenohumeral joint.
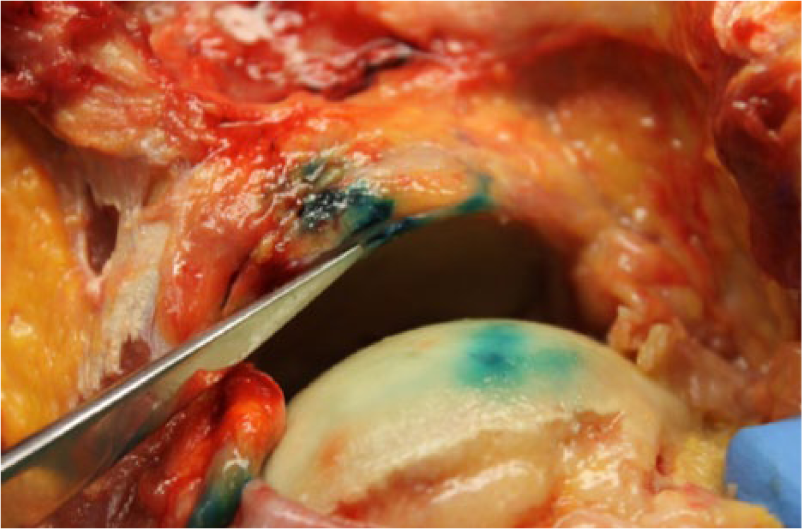
Gross image of the exposed labrum, which contains the presence of colored (blue) dye, as injected through a sonographically guided injection.

Gross measurements were made of a removed portion of the labrum and compared with measurements made from sonographic images. Note the presence of blue dye on the removed labrum, confirming injection in the proper space.
Diagnostic Medical Sonographic Measurements
Retrospectively, diagnostic medical sonographic measurements were completed on images that had been archived on the system. The investigator making these measurements (K.R.V.) was blinded to the results of any other measurements carried out in the study to eliminate as much as possible any researcher bias. Calipers were placed on the edges of the labrum in an anterior-to-posterior fashion before measurements were recorded and entered into a database. Diagnostic medical sonographic measurements were then repeated by a second investigator (A.D.) to allow an interrater reliability measure analysis.
Results
The replication of Taljanovic et al.’s 11 study and the use of Schydlowsky et al.’s 12 method for validation were important to reaffirm the concept that DMS can evaluate the GH labrum. Given that this proof of concept was introduced more than 15 years ago, technology advances theoretically would only provide better visualization of the structures in question. However, in this replication, we were able to image only the posterior superior, posterior inferior, and anterior inferior aspects of the GH labrum. Some of this was due to the advanced age and degeneration of the labrum. The freezing and thawing process also causes redistribution of the water in the tissue and affects the sonographic image quality. Despite this, Bankart lesions, confirmed on dissection, were identified in two shoulders. The presence of dyes within and around the labrum was visually confirmed (Figure 7), and the indentation made by the spinal needle in three different regions of the labrum provided visual confirmation. On the basis of the dissection results, the dyes appeared to have been injected in the predefined regions of the labrum as visualized using DMS.
Diagnostic medical sonographic measurements from the images were compared with the gross measurements that were taken from labral specimens recovered at the time of dissection (Table 1). The axillary view provided visualization of a portion of the labrum that can be difficult to evaluate but was consistently imaged in all six cadaveric shoulders. During dissection, it was noted that many of the labral samples were difficult to remove because of ossification. Such ossification of the posterior part of the capsule labrum complex would indicate the presence of Bennett lesions. 13
Gross Labral Measurements Made at the Time of Dissection Compared With Measurements of the Labrum Obtained Sonographically, With Each of the Three Scanning Approaches Investigated.
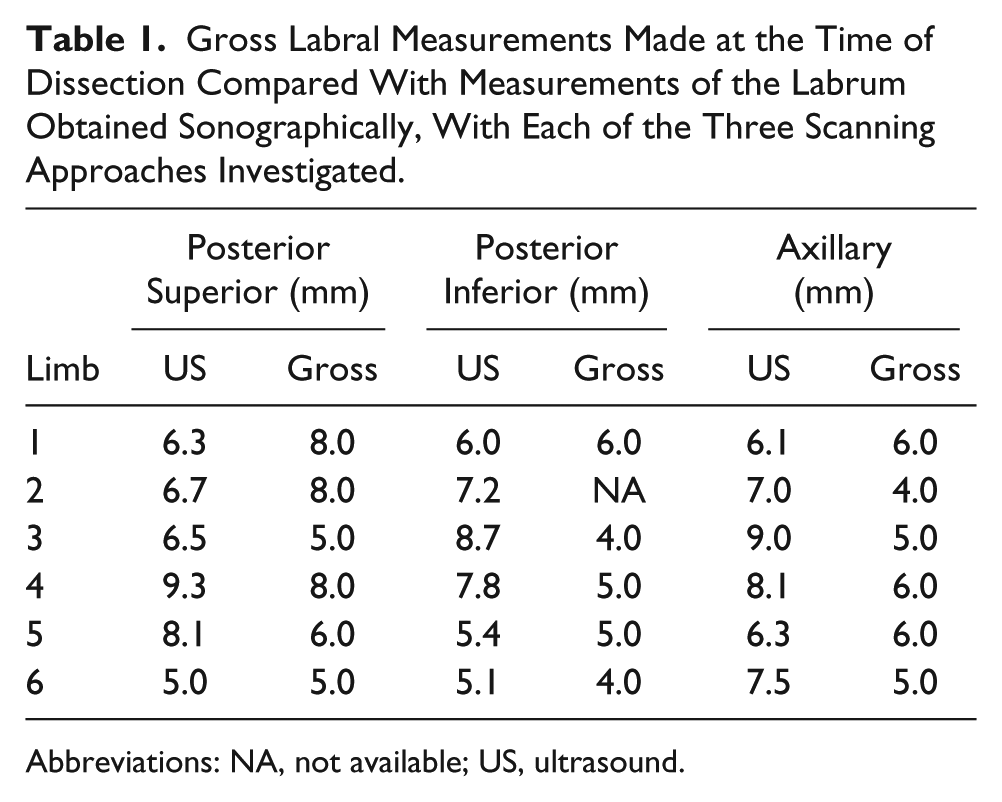
Abbreviations: NA, not available; US, ultrasound.
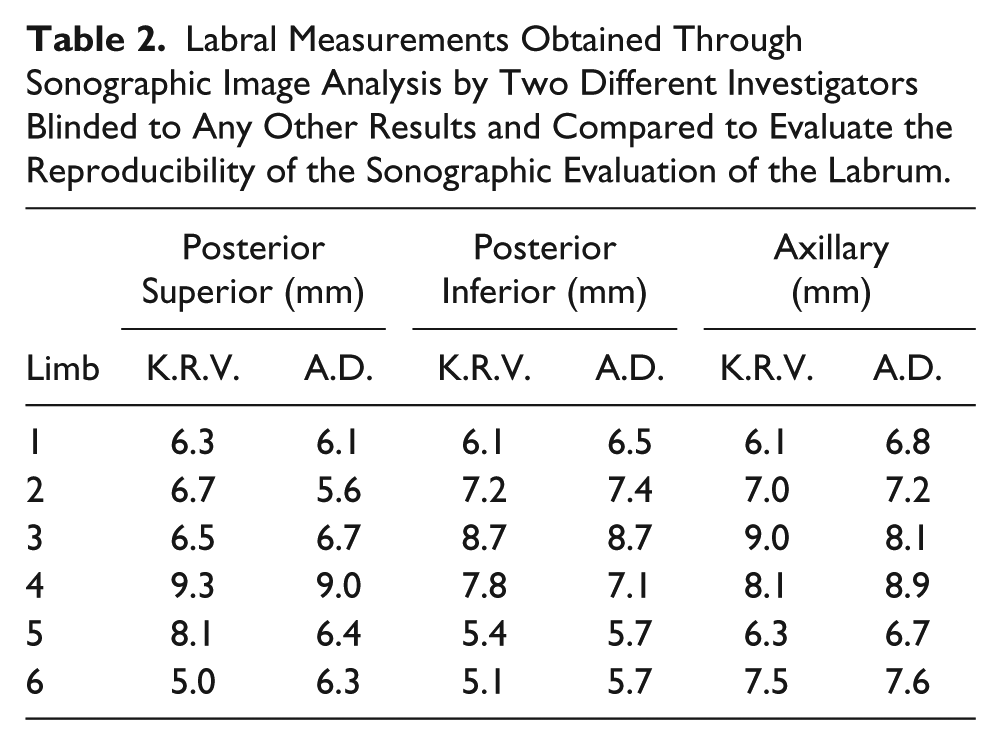
A two-tailed t test for paired variance between the diagnostic medical sonographic image measurements and the gross specimen samples was done to ensure the validity of the measurements as obtained from the diagnostic medical sonographic image (Table 1). The measurements obtained by the more senior sonographer were compared with the gross labral measurements. Student t tests were done to compare sonographic and gross measurements from the posterior superior labrum (P > .05), the posterior inferior labrum (P > .05), the axillary labrum (P < .05), and all sites combined (P < .05). Although the sample size was small and unlikely to have statistical power, an interrater reliability measurement was done using a Pearson correlation between the two researchers who performed sonographic measurement analysis (Table 2). Results for the researchers’ measurements were r = 0.72 (P > .05) from the posterior superior labrum, r = 0.95 (P > .05) from the posterior inferior labrum, and r = 0.83 (P > .05) from the axillary labrum. For all sites combined, the result was r = 0.82 (P > .05).
Labral Measurements Obtained Through Sonographic Image Analysis by Two Different Investigators Blinded to Any Other Results and Compared to Evaluate the Reproducibility of the Sonographic Evaluation of the Labrum.
Discussion
Sonography of the shoulder and the shoulder joint is gaining in clinical popularity, in part because of the dynamic ability to correlate physical findings and clinical testing with imaging. However, only a few studies, conducted in the 1990s, provide proof of concept,11,12 and therefore this replication was considered timely for the field. A few cohort studies have also been reported; however, these were based on the evidence gathered previously, and improved sonographic techniques are needed to fully address all the lesions (Bankart and SLAP tears) that occur because of GHJ dislocation.12,14,15 The goal of this study was to reaffirm the concept that multiple sonographic approaches can be used to evaluate four quadrants of the labrum. A special emphasis was placed on the anterior inferior region of the labrum because of the increased incidence of anterior inferior dislocations that can contribute to Bankart lesions.
In a recent study completed with PMHS shoulders, the ligamentous attachments were systematically detached from an inferior approach. 16 Twenty specimens demonstrated that it took at least three different areas to become detached before external rotation and abduction caused dislocation. This preclinical experiment pointed to the possibility that injuries in various locations around the GHJ are needed to result in the humeral head dislocating in an anteroinferior direction. These results indicated that the approach of this study was needed in that multiple diagnostic medical sonographic scanning approaches are necessary to properly evaluate the glenoid labrum. Although Bankart lesions occur in the anteroinferior portion of the glenoid, dislocation may result from added tears in the posterior or anterosuperior position. In a clinical study conducted by Schydlowsky et al., 17 a cohort of 29 patients were screened with DMS for anteroinferior labral lesions, and 90% of them had shoulder dislocation with tears. This small cohort study was confirmed with arthroscopy for 9 patients with acute injuries and 20 with recurrent dislocations. The combined group of patients had 26 labral lesions, and DMS was only 88% sensitive for detection, with specificity of 67%. One of the main issues causing a lack of detection of labral lesions in this cohort was the difficulty in visualization of the lesions between 5 and 6 o’clock. For this reason, in the present study, the transducer was fanned so that the GH labrum from 3 to 6 o’clock could be evaluated to increase the detection rate for Bankart lesions, because this is attributed to shoulder dislocation. The protocols used were able to successfully identify the three regions of the glenoid labrum despite the advanced age and degeneration of the labrum, as identified by the visualization of the injected dye upon dissection. The freezing and thawing process of the PMHSs also caused redistribution of the water in the tissue and affected diagnostic medical sonographic image quality. Despite this, it was possible to identify Bankart lesions in two shoulders, which were confirmed on dissection. In clinical practice, without the limitations imposed by the tissue-preserving process, labral image quality in patients should be improved.
In contrast to previously published studies, in this study, we were unable to collect any reliable sonographic imaging data with the anterosuperior approach. Although this is advocated in the literature,4,5 we had no success with this anterosuperior approach, making any SLAP tears difficult to detect in this group. The inability to collect data with this approach could have been due to a number of factors. First and foremost, imaging in this location is technically difficult because of the overlying position of the clavicle. Acquiring images around the clavicle, and the associated shadowing in this region, can prove troublesome even for the most experienced of sonographers. Second, this study was carried out in a cohort of PMHSs with an age range of 76 to 95 years. Because of tissue deterioration and other potential injuries that may have occurred over time, this may have increased the challenge of obtaining quality images of the GHJ with this approach. This replication study does provide further evidence that Bankart lesions can be visualized with an axillary approach, and by fanning the beam, more labral tears could be detected for acute and chronic shoulder dislocations. This study also takes the current evidence a step further by providing statistically significant validation when comparing measurements obtained through DMS and the gross specimen of the labrum made in this region. Additionally, it was noted incidentally that ossified areas could be seen of the posteroinferior aspect of the labrum (9–6 o’clock) that are associated with Bennett lesions, a mineralization of the posterior band of the inferior GH ligament. These were not noticed during our scanning of the posterior labrum and GHJ, but typically these lesions are best diagnosed on MRI and commonly are seen on CT. 18 In this replication study, we also used a higher frequency broadband transducer, providing the ability to shift and increase resolution for lesions at a variety of depths. The previous studies cited had only 5- to 7-MHz selection, whereas the probe used in this study had an upper limit frequency of 9 MHz, with the added advantage of more sophisticated signal-processing capabilities to enhance image quality.
Limitations
A limitation of the present study, using only a small number of specimens, was the level of evidence and associated research design, precluding generalizations to clinical practice. Because of the small sample size investigated, most statistical outcomes were deemed not statistically significant. However, the study design replicated a preclinical study, which does allow a formative hypothesis about sonographic imaging of the labrum. It is also of note that inherent differences in tissue and patient variety may hinder diagnostic accuracy. A further limitation was the age of the cadaver samples, so that no comments can be made on how the capsule-labral complex in younger individuals may differ from the more elderly sample population in this study. The removal of tissue samples was complicated by the ages of the subjects, and many of the samples were damaged during dissection; any quantitative comparisons would be better completed in vivo. Regardless, this study showed the ease of identifying the capsule-labral complex, and image quality may be improved in vivo.
Conclusions
The concept of using an axillary scanning approach for detecting labral tears and Bankart lesions among acute and chronic shoulder dislocation patients may be worthwhile to incorporate into a shoulder-scanning protocol. The increasing incidence of shoulder dislocation (acute and chronic) that occurs in the anteroinferior direction makes the detection of Bankart lesions an important diagnostic endpoint.
Footnotes
Acknowledgements
We would like to thank Mark and Michelle Whitmer for their invaluable help in the anatomy laboratory. Their dedication and support of our research is greatly appreciated. We would also like to thank our laboratory technician, Christopher Kanner, for his assistance in the development of this report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.