
Abstract
Objective
This study was performed to describe a new technique for reduction of anterior glenohumeral dislocation in four non-sedated patients in whom traditional techniques were unsuccessful.
Methods
Four patients with clinically and radiographically proven acute anterior glenohumeral dislocations were admitted to the emergency department. An oral analgesic and local infiltration of lidocaine into the glenohumeral joint were administered prior to the reduction attempts. Four to six reduction attempts using a variety of traditional maneuvers were unsuccessful before applying our technique. The glenohumeral joint was then successfully reduced using our technique and confirmed on radiographs. A sling was placed for post-reduction pain relief.
Results
All four patients underwent successful closed reduction, proven clinically and by radiographs, after the first attempt using our technique. No complications occurred.
Conclusion
Our maneuver provides safe and successful closed reduction for irreducible acute anterior glenohumeral dislocation.
Keywords
Introduction
Anterior glenohumeral (GH) dislocation is the most common traumatic dislocation, and numerous techniques have been described for the reduction of such dislocated joints. 1 Because relaxation is a key factor for successful reduction, all dislocated joints should ideally be reduced under general anesthesia with adequate analgesia and muscle relaxation. In practice, most departments attempt initial reduction in the emergency room without sedation. 2 Reduction of an anterior GH dislocation can be a major challenge to the physician, especially in a young, muscular, nonsedated patient. In addition, uncooperative patients and first-time dislocators can make closed reduction quite difficult. We herein describe a new technique for reduction of irreducible GH dislocation. The efficacy of our maneuver was proven in four patients in whom traditional closed reduction maneuvers were unsuccessful.
Patients and methods
The publication of these retrospective data was approved by the local Institutional Review Board of Emek Medical Center. Patient consent was not required because of the retrospective nature of the study. Four patients with clinically and radiographically proven acute anterior GH dislocations were admitted to the emergency department (Table 1). An oral analgesic and GH joint infiltration with lidocaine were administered to all patients prior to reduction attempts. Four to six reduction attempts using a variety of traditional maneuvers were unsuccessfully attempted before applying our technique. The GH joint was then successfully reduced using our technique and confirmed on radiographs. The patients were given a sling for post-reduction pain relief.
Demographic data
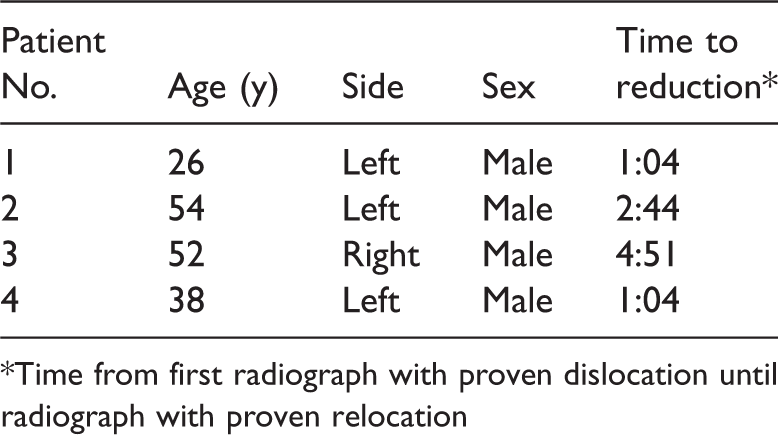
*Time from first radiograph with proven dislocation until radiograph with proven relocation
Reduction technique
The maneuver used in this study was based on the traction–counter-traction principal and required two or three physicians. The patient lay supine on the table. A bed sheet was applied to the patient’s axilla for counter-traction. Physician 1 grasped the patient’s wrist with both hands and applied steady longitudinal traction with the arm in 45° of abduction. Physician 2 applied counter-traction using the bed sheet. Counter-traction could also have been performed using the sole of Physician 1’s foot as described in the Hippocratic maneuver. 2 Physician 3 applied a second bed sheet around the patient’s forearm as proximal to the axilla as possible and applied steady traction perpendicular to the forearm axis (Figure 1). After 3 minutes of steady traction, Physician 1 gradually adducted the forearm until the humeral head was relocated (Figure 2). Importantly, Physician 3 maintained forearm movement and traction perpendicular to the forearm axis.

Starting point: 45° of abduction

Relocation: 15° of abduction
Anatomy
More than 95% of GH dislocations are anterior. Violent external rotation in abduction levers the head of the humerus out of the glenoid socket, avulsing anterior bony and soft tissue structures in the process (Bankart lesion). 3 The posterior part of the humeral head exits the joint and often collides with the anterior rim of the glenoid, creating a bony indentation at the back of the humeral head (Hill–Sachs lesion). 4 , 5 The GH joint consists of the small scapular glenoid fossa and a relatively large humeral head. This inherently unstable joint is stabilized by four rotator cuff muscles. In anterior GH dislocation, the rotator cuff muscles stretch and spasm, causing pain. It is theorized that spasm of the long head of the biceps brachii muscle acts as a “bowstring,” keeping the humeral head out of the glenoid fossa. 6 The biceps brachii theory also explains the medial location of the humeral head in relation to the glenoid, which can be seen on an anteroposterior radiograph of a dislocated GH joint. The position of the humeral head in relation to the glenoid rim dictates the direction of traction for successful reduction.
Results
Four patients with anterior GH dislocation were enrolled in our study. All four underwent successful closed reduction, proven clinically and by radiographs, after the first attempt at using our technique. No complications were recorded.
Discussion
More than 50 GH dislocation repositioning techniques exist. 7 , 8 The wide range of techniques can be divided into three groups: traction, leverage, and biomechanical techniques. 6 ,8–11 The classic traction–counter-traction technique (Hippocratic maneuver) relies on disimpaction of the humeral head to relocate it. 1 Although traction in the longitudinal axis with the arm in 45° of abduction disimpacts the head, it relies mainly on the physician’s force to overcome the muscle spasm, which will disimpact the head distally enough to bring the humeral head back into place. In young, muscular, painful, first-dislocator males, muscle spasm may overcome the physician’s force, preventing the humeral head from relocating.
Our technique takes into account the anatomic location of the dislocated humeral head in relation to the glenoid and the vectors of the forces acting on the humeral head. The traction–counter-traction performed by Physicians 1 and 2 disimpact the humeral head by overcoming the proximal pull of the deforming forces around the shoulder and creating a potential space for the humeral head to relocate. However, this is not enough in some cases.
Physician 3 applies a bed sheet around the patient’s forearm as proximal to the axilla as possible and applies steady traction perpendicular to the forearm axis. This traction is designed to overcome the pull of the humeral head medially, which may significantly add to the reduction (Figures 1, 2). In addition, the gradual adduction (Figures 1, 2) (from 45° of abduction as a starting point) exposes the rounded, relatively smooth articular surface of the humeral head to the articular surface of the glenoid. As a consequence, the humeral head glides easily into its natural place.
The four patients in the present study had undergone four to six unsuccessful reduction attempts using a variety of traditional maneuvers (Hippocratic traction–counter-traction, 7 , 8 , 10 Kocher, 12 Milch, 13 and scapular manipulation 14 , 15 ) before we applied our technique. All previously mentioned techniques were described as successful in a variety of studies, but no consensus on the optimal technique for reduction of anterior GH dislocation has been established. 2 Our technique offers a simple, nontraumatic solution for reduction of anterior GH dislocation. The technique involves no sharp movements or extreme positions of the arm, which may produce a fracture. In addition, the technique can be extremely useful when sedation is not available.
There are some disadvantages to our technique. Application of the maneuver requires two to three physicians and cannot be carried out by a single physician. In addition, patient cooperation is still needed to some degree because application of the maneuver may be painful.
The limitations of our study are the small group of patients and its retrospective nature. Nevertheless, this case study presents an easily applied reduction maneuver in patients with anterior GH dislocation in whom traditional maneuvers were unsuccessful.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Footnotes
Funding
No benefits in any form were received or will be received from a commercial party related directly or indirectly to the subject of this article.