
Abstract
The objective of this study was to determine if point-of-care sonography of the shoulder would change diagnosis or management in patients presenting to a sports medicine clinic with shoulder pain. We performed an observational, nonrandomized, nonblinded study of provider behavior when evaluating patients presenting to a sports medicine clinic with shoulder pain. The provider completed a questionnaire regarding the most likely diagnosis and management plan after he or she had performed a physical examination and radiograph(s). Following the physical examination and radiograph(s), a bedside ultrasonographic examination (BUS) was done and the provider completed a second questionnaire regarding the findings on sonography and revisions, if any, to the diagnosis and management plan. Data were collected on 42 patient encounters. BUS led to a change in diagnosis in 53% of cases. BUS led to a change in management plan in 60.4% of patients. BUS increased provider confidence in the diagnosis from 3.7 ± 0.19 (95% confidence interval [CI]) to 4.5 ± 0.21 (95% CI) on a 1 to 5 scale, with 1 being least confident and 5 being most confident. The addition of bedside sonography to the physical examination and radiographic studies of patients with undifferentiated shoulder pain resulted in a significant number of changes to the diagnosis and management plan as well as significantly increased diagnostic confidence.
The use of point-of-care musculoskeletal sonography in sports medicine practice has increased dramatically. To our knowledge, the effect of sonography on the diagnosis or management of musculoskeletal conditions when added to current evaluation methods has not been studied.
The ability to diagnose and intervene in musculoskeletal pathology at the bedside has made sonography an important part of sports medicine practice. Sonography has a higher sensitivity than the physical examination for the diagnosis of rotator cuff tears. 1 Sonography has compared favorably with magnetic resonance imaging (MRI) and operative findings for the diagnosis of partial and complete thickness rotator cuff tears.2–4 Subacromial bursitis, impingement, and pathology of the long head of the biceps tendon, with the exception of partial-thickness biceps tendon tears, can be evaluated with high sensitivity with sonography.5–7 Trained nonradiologists can accurately evaluate the rotator cuff with sonography, making this a promising tool for the sports medicine clinician. 8 These characteristics suggest that point-of-care sonography may provide benefit to patients undergoing evaluation for shoulder pain.
Clinician-performed sonography has been shown to change diagnosis and management decisions in emergency medicine and rheumatology. In patients presenting to the emergency department with joint pain or erythema, sonography changed management in 65% of cases. 9 Soft tissue sonography changed diagnosis and management in adult and pediatric populations with cellulits.10,11 The literature surrounding the effect of musculoskeletal sonography on diagnosis and management, however, is limited. In a rheumatology clinic setting, sonography allowed the clinician to better define the source of pain in patients with an acute flair of knee osteoarthritis. 12 In a rheumatology practice, sonography findings influenced treatment in 27% of patients with a variety of disease processes. 13 We hypothesized that the addition of bedside sonography to history, physical examination, and radiographs of patients presenting with shoulder pain would result in changes in the diagnosis and the management plan and improve provider confidence in diagnosis.
Materials and Methods
Providers at two university sports medicine clinics participated when evaluating patients with a new chief complaint of shoulder pain. Patients with prior MRI or sonography of the shoulder were excluded. The study was a nonblinded, nonrandomized, observational study of provider behavior when evaluating a convenience sample of patients presenting to two university sports medicine clinics with a primary complaint of shoulder pain. The University of Utah Institutional Review Board approved the study protocol prior to data collection. Provider forms were collected between August 15, 2012, and November 15, 2012. Sports medicine attending physicians and fellows performed ultrasonography as part of their standard evaluation. The provider completed a questionnaire regarding the most likely diagnosis, the provider’s confidence in the diagnosis, and the management plan after he or she had performed a history and physical examination and viewed a three-view shoulder radiograph. The provider then performed a limited diagnostic bedside ultrasonography (BUS) of the shoulder. Following sonography, the provider completed the questionnaire recording the findings on sonography and revisions to the diagnosis and management. Provider confidence in diagnosis following sonography and the provider’s impression of the utility of sonography for the patient evaluation were recorded. Study data were collected and managed using REDCap electronic data capture tools hosted at University of Utah. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources. 14 Descriptive statistics were evaluated and confidence intervals (CIs) reported using an α level of ≤0.05 for all tests.
Results
Data were collected on 42 patient encounters. Providers completing surveys were attending physicians and primary care sports medicine fellows with backgrounds in emergency medicine, family medicine, and physical medicine and rehabilitation. There were 25 (59.5%) male and 17 female patients. The ages ranged from 15 to 80 years.
After physical examination and radiographic review, provider confidence in the diagnosis was reported at 3.7 ± 0.19 (95% CI) on a 1 to 5 scale, with 1 being least confident and 5 being most confident. After BUS was performed, provider confidence in diagnosis improved to 4.5 ± 0.21 (95% CI) (P < .01). Provider assessment of clinical usefulness of sonography was 3.7 ± 0.31 (95% CI), with a score of 1 being least useful and 5 being most useful. BUS led to a change in diagnosis in 53% of patients and a change in management plan in 60.4% of patients. The most common changes in management plan were “new injection” at 31% frequency, “new MRI” at 28% frequency, and “cancel MRI” at 21% frequency. The most common finding on sonography was a normal examination of the shoulder (Table 1). The most common diagnosis prior to sonography was rotator cuff tear, with a frequency of 33%. The most common diagnosis following sonography was rotator cuff tear, with a frequency of 45%.
Sonography Findings.
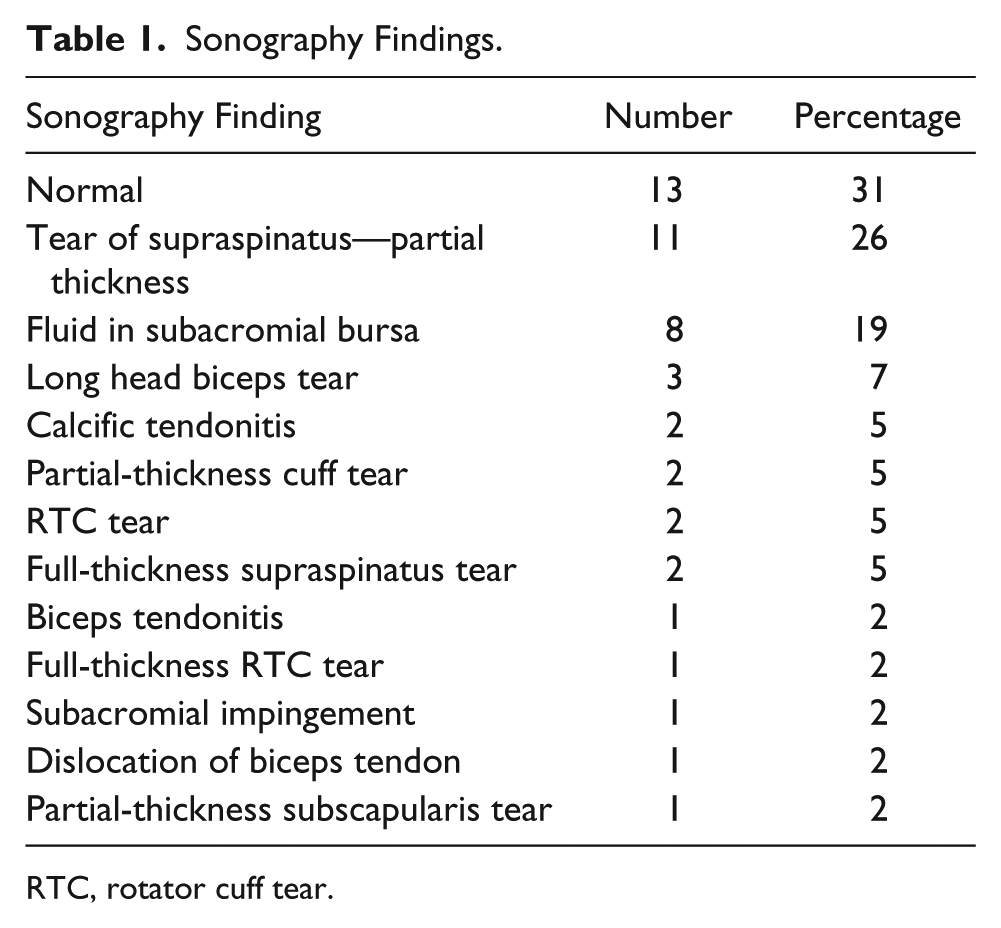
RTC, rotator cuff tear.
Discussion
In this limited observational trial, the use of bedside musculoskeletal sonography resulted in significant changes in diagnosis, management, and providers’ diagnostic confidence in patients presenting to two sports medicine clinics with undifferentiated shoulder pain. Prior studies have demonstrated the high sensitivity and specificity of sonography in the diagnosis of common conditions of the shoulder.2–8 Bedside musculoskeletal sonography is inexpensive, does not involve ionizing radiation, and has become more accessible across many specialties, including sports medicine. These attributes make clinician-performed sonography a natural adjunct to current evaluation involving history, physical examination, and, often, radiographs. Our study adds to the existing literature with descriptive information on the possible changes in diagnosis and management of shoulder pain using point-of-care sonography.
The results show a change in diagnosis in 53% of cases and a change in management in 60% of cases. The change in diagnosis often resulted in a more specific diagnosis than reported after radiograph and physical examination. The most common change in management was a new sonography-guided injection (31%), suggesting that sonography allowed the provider to intervene on specific pathology visualized. The most common change in diagnosis was the new diagnosis of rotator cuff tear in patients previously thought to have an alternative diagnosis such as rotator cuff tendinopathy or impingement syndrome.
Sonography resulted in a new order for an MRI in 28% of patients and the elimination of an MRI order in 21% of patients. A potential explanation of this finding is that the use of sonography may allow the clinician to order advanced imaging in a more directed way. Of note, at our institution, MRIs are requested by orthopedic surgeons for full-thickness rotator cuff tears visualized on sonography in patients being considered for an operative intervention. In other settings, and as orthopedic surgeons become more comfortable with sonography, some of these patients with acute full-thickness rotator cuff tears may have been considered for operative repair without further imaging.
This study has several important limitations. The observational design has the risk of introducing selection bias in the patients included by the provider and in the study forms completed and returned. Providers participating in the study had completed variable levels of training in musculoskeletal sonography, introducing the possibility of variability in the quality and the accuracy of the examinations performed. Most encounters were recorded from a single clinic with one supervising attending physician (38/42 [90.4%]). The results observed were affected by this attending’s practice patterns and experience, limiting the ability to generalize these results to other settings.
Conclusion
Bedside sonography performed by sports medicine physicians resulted in significant changes to diagnosis and management when added to history, physical examination, and radiographic studies. Given the low cost, lack of ionizing radiation, and demonstrated change in diagnosis and management, sonography may be a useful addition to patients presenting to a sports medicine clinic with shoulder pain. Blinded prospective studies are needed to determine the subsets of patients who are likely to benefit from initial sonographic evaluation.
Footnotes
Acknowledgements
This work was presented at the 2013 American Medical Society for Sports Medicine Annual Conference, April 17-21, 2013, San Diego, CA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.