
Abstract
Objective:
There has always been some issues in the accurate diagnosis of pneumonia, a common cause of emergency department (ED) visits and revisits, which is typically made based on the patient’s clinical syndrome. This is made more difficult due to the traditional chest radiography having limited accuracy. This prospective multicenter study was conducted to determine the diagnostic accuracy of a point-of-care lung sonography performed by emergency physicians for the diagnosis of pneumonia in an acute care setting. This was compared with chest computed tomography (CT), the diagnostic gold standard.
Methods:
ED patients who presented with signs and symptoms of pneumonia were eligible to enroll in the study. After enrollment, point-of-care lung sonography was performed on patients by emergency physicians who had passed a focused teaching course on lung sonographic findings of pneumonia. All enrolled patients were followed up. Patients who underwent a chest CT during their hospital admission course were finally included and analyzed.
Results:
Emergency physicians who performed a point-of-care lung sonography had a sensitivity of 100%, specificity of 75%, positive predictive value of 88.88%, negative predictive value of 100%, and an overall accuracy of 90% in the diagnosis of pneumonia.
Conclusion:
These emergency physicians could accurately diagnose pneumonia, with a point-of-care lung sonography, after completing a focused sonography course.
Pneumonia is a common cause of emergency department (ED) visits and revisits, hospital admissions and readmissions, sepsis, nosocomial infections, and death, especially in elderly patients with comorbid conditions.1–4 There has always been some issues in the accurate diagnosis of pneumonia, and it is mainly made based on the patient’s clinical syndrome. Chest radiography (CXR) has limited (65%) diagnostic accuracy in this field,5,6 predisposes the patient to ionizing radiation, needs special patient positioning, and requires expertise for correct interpretation. Computed tomography (CT) is considered the gold standard in diagnosing pneumonia; however, it is a less available, more expensive, and time-consuming choice. CT is associated with high ionizing radiation exposure and more operational difficulties, especially in critically ill patients.7,8
Although lungs were not traditionally considered a diagnostic target for sonography, except in some limited entities like evaluating the pleural effusion and sonography-guided biopsies, it has been applied to different pulmonary pathologies in both traumatic and nontraumatic patients.9,10 Interestingly, the diagnosis of pneumonia has not been an exception, as a meta-analysis on the role of lung sonography in the diagnosis of pneumonia found a sensitivity of 97% and specificity of 94% for this modality. 11 A systematic review in this area showed a high sensitivity (94%) and specificity (96%) for the diagnosis of pneumonia in adults by sonography. But in most of these studies, lung sonography is performed by high-skilled experienced sonographers or radiologists, rather than emergency physicians. 12
This prospective multicentered study was conducted to determine whether lung sonography could be useful in the ED, with emergency physicians, to quickly assist in the accurate diagnosis of pneumonia.
Methods
Study Design and Setting
This prospective multicentered study was conducted across three tertiary-level teaching hospitals, EDs, posting an annual census between 40 000 and 70 000 patients. The sites were able to conveniently enroll patients from May 2019 to April 2020. The institutional ethics committee approved this multicentered study. The work was carried out in accordance with the Declaration of Helsinki (1989). In addition, an informed written consent was obtained from all patients or their legal guardians.
Participants
Adult (>18 years old) patients admitted to the ED, with a suspected primary pneumonia, were eligible to participate. The study included patients who underwent chest CT during their hospital admission course. Those patients who were triaged and discharged, as well as patients without a chest CT, were excluded from the study. Pregnant women and patients, referred with a diagnosed pneumonia, were also excluded from the study.
Intervention
Eight emergency physicians, who had the experience of performing at least 100 previous lung sonograms, (generally in trauma patients), attended a 4-hour didactic and practical course on the basics of chest sonography, which included sonographic findings of pneumonia. Patients suspected to have pneumonia, who were admitted to the ED, were evaluated by these physicians, as early as possible. A primary impression of pneumonia was considered, for these patients, based on their history and physical examination findings. Point-of-care sonography was performed for the enrolled study patients, and the results were interpreted by the emergency physician, who completed the course.
A review of all patients was made until discharge. Patients who underwent a CT, during their hospital admission, were included in the study. Results of the lung sonogram were compared with the results of CT. The accuracy of the lung sonogram was determined by comparing with the CT, given it is considered the gold standard. In patients with any indication for immediate therapeutic intervention, including patients with hemodynamic instability, the lung sonogram was done after stabilizing the patient. This was done so that it would not interrupt the treating medical team’s activities. Any diagnostic or therapeutic interventions were performed for patients as needed. The results provided by the emergency physician, performing the lung sonogram, did not affect the clinical decisions of patients enrolled in the study. Four radiologists interpreted the lung sonograms, and they were blinded to the results of the ED lung sonogram and the patients’ clinical conditions.
In patients for whom CXRs were obtained, the posteroanterior and lateral views were obtained in the upright or sitting position. The anteroposterior view was taken in the supine position, for patients unable to tolerate the upright or sitting positions.
Sonography Protocol
The area between the parasternal and anterior axillary line, extending from the clavicle to the diaphragm, was considered anterior hemithorax and scanned in the second (or third) and fifth (or sixth) intercostal spaces. The area between the anterior and posterior axillary lines, extending from the axilla to the lower costal margin, was considered lateral hemithorax and scanned in upper and lower halves. The area between the posterior axillary and paravertebral lines, extending from the neck base to the diaphragm, was considered posterior hemithorax and scanned below the level of the tip of scapula.
The anterior and lateral sides of the hemithorax were studied while the patient was in the supine position, and the posterior hemithorax was studied in the sitting position. If the patient could not tolerate the supine position, the anterior and lateral sides of the hemithorax were studied in the semi-sitting position. In those cases where the patient could not tolerate sitting, the posterior hemithorax was studied in the lateral decubitus position.
Step-by-step scanning of four to five areas in each hemithorax was started by placing the probe in the second (or third) and fifth (or sixth) intercostal spaces, approximately in the midclavicular line for anterior hemithorax evaluation. The examination was continued by placing the probe in the upper and lower halves of the lateral hemithorax. In cases where there was no sonographic evidence of pneumonia, in anterior and lateral hemithoraces, the posterior hemithorax was also scanned. This was accomplished by having the patient lie in the lateral decubitus or sitting position.
Sonography was performed with SonoAce X8 (Medison, South Korea) equipment and 7.5 MHz linear-array probe. The probe was placed horizontally (obliquely), perpendicular to the chest wall (sliding and angling as needed) and pointing the transducer indicator, to the patient’s right side. All sonographers were blinded to the results of patients’ CXR, CT, and laboratory tests.
A lung sonogram was considered positive for pneumonia if any of these findings were found: (1) focal alveolar pattern, (2) focal interstitial pattern, (3) positive air/fluid bronchogram, and (4) necrotic areas. The alveolar pattern (hepatization) is the liver-like appearance of the lung, due to subpleural lung consolidation. This can be caused by air bronchograms that appear as echogenic branching structures or multiple echogenic spots (showing air trapped in small airways), which move with breathing. An interstitial pattern is defined as the presence of three or more B-lines or comet tail artifacts. B-lines are vertical narrow-based rays radiating from the pleural line to the edge of screen, moving with lung sliding. These erase normal A-lines and are seen when the alveoli are filled with extravascular water instead of air. The pleural line is an echoic line between two rib shadows sliding with breathing. In normal air-filled lung parenchyma, nothing is visualized beyond pleural line (Figure 1). In patients with localized pathologies like pneumonia or lung contusion, interstitial syndrome is seen locally. It is also noted in patients with generalized pathologies like pulmonary edema, acute lung injury, or acute respiratory distress syndrome in whom the interstitial syndrome is seen diffusedly. The increased appearance of B-lines denotes there is excess extravascular water in the lung field (Figure 2). 12
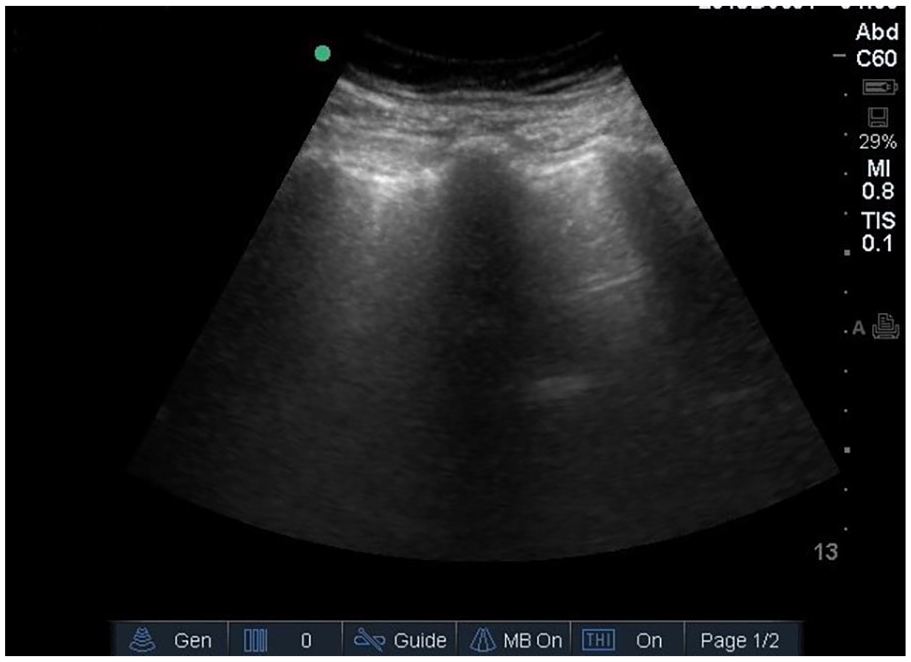
Normal lung sonographic image.
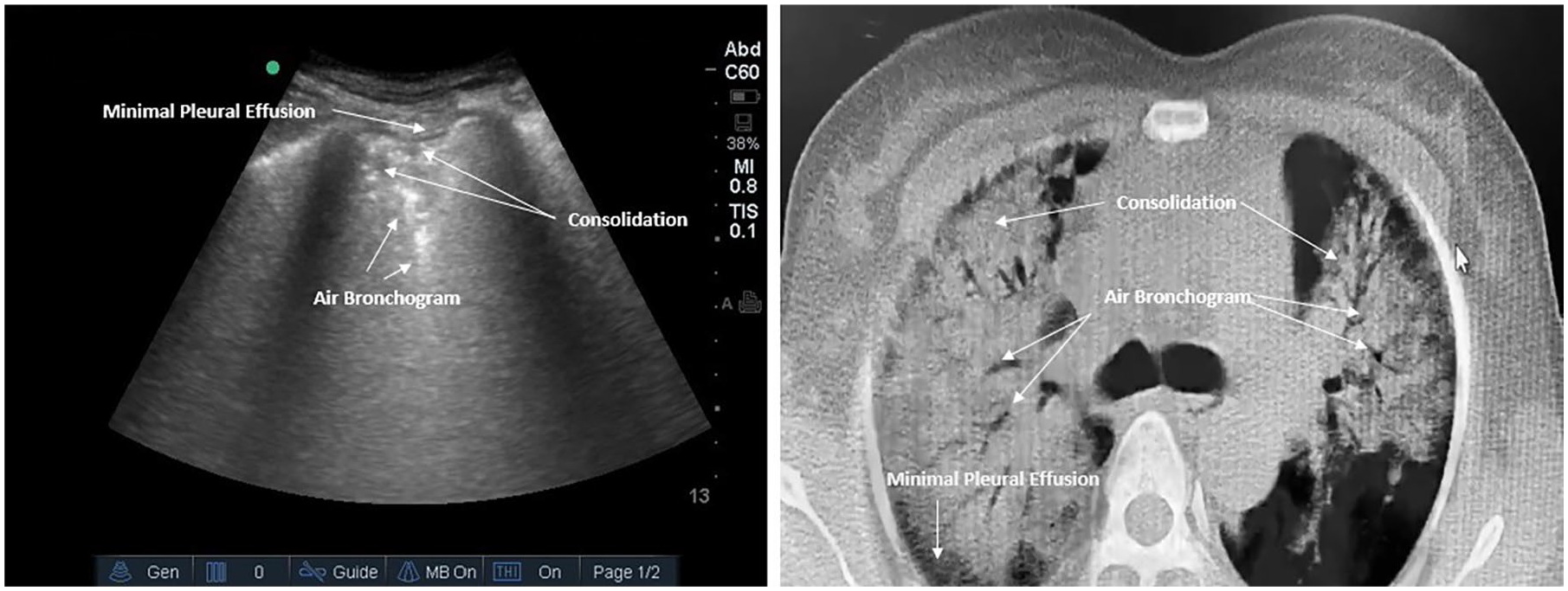
Lung sonogram (left) and chest CT (right) findings in a patient with pneumonia. Pleural effusion is seen in black both in sonography and in CT scan, air bronchogram appears echogenic on the sonography and radiolucent in CT, and consolidation is seen as anechoic in sonography and radiopaque on the chest CT. CT, computed tomography.
Data Analysis
Descriptive data are reported as mean (±SD), maximum, and minimum. Categorical data are presented as percentages. Sensitivity, specificity, positive and negative predictive values, and overall accuracy of point-of-care lung sonography are calculated. All analyses are done by SPSS statistical software SPSS, version 18 (SPSS, Inc., Chicago, IL).
Results
There were 164 patients assessed for eligibility to join the study. In this cohort, one patient was pregnant. In addition, five patients were referred for admission with a known diagnosis of pneumonia. Within the group, four patients left the hospital against medical advice, before completing the study. There were eight patients who refused to participate in the study. Of those invited, 146 patients were successfully enrolled in the study. A chest CT was done for 55 of the 164 patients, during their hospital admission. For those same 55 patients, a CXR was also obtained. The basic characteristics of this cohort and their findings are summarized in Table 1.
Baseline Data of Studied Patients.
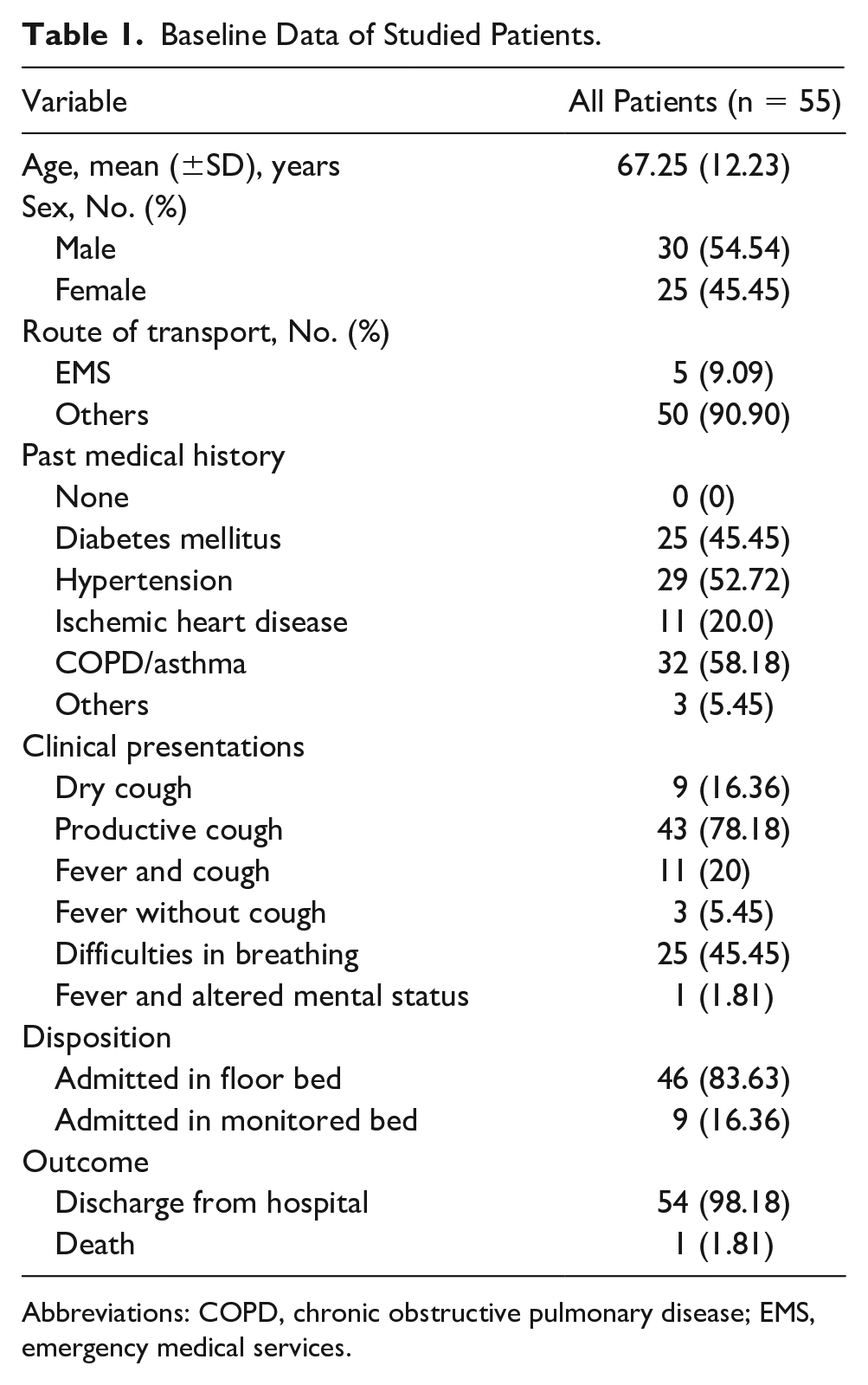
Abbreviations: COPD, chronic obstructive pulmonary disease; EMS, emergency medical services.
Diagnostic Results
The chest CTs were positive for pneumonia in 40 patient cases. All of those 40 pneumonia cases were correspondingly diagnosed with lung sonography. There were 15 patients with a negative chest CT for pneumonia. In 5 of those 15 patient cases, the lung sonogram was interpreted as falsely positive. The results of the chest CT, lung sonogram, and CXR are compared in Table 2. The sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy of the lung sonography and CXR, compared with chest CT scan, are summarized in Table 3. The lung sonographic findings are summarized in Table 4.
Comparison of Positive/Negative of Pneumonia Results From CT Scan, Sonography, and Chest Radiography.
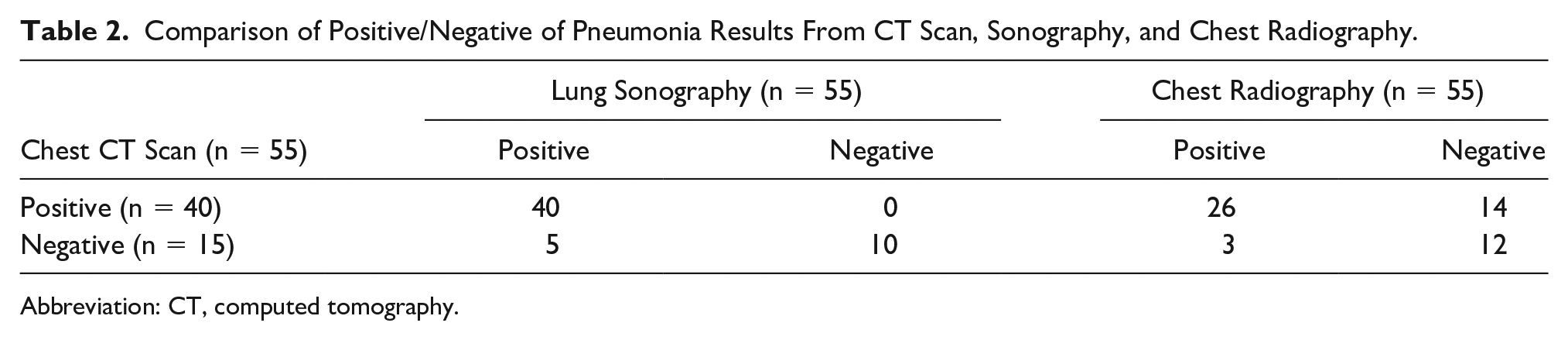
Abbreviation: CT, computed tomography.
Accuracy of Lung Sonography and Chest Radiography in Diagnosis of Pneumonia (In Comparison With Computed Tomographic Scan).

Lung Ultrasound Findings in Patients With Positive CT Scan and CXR.
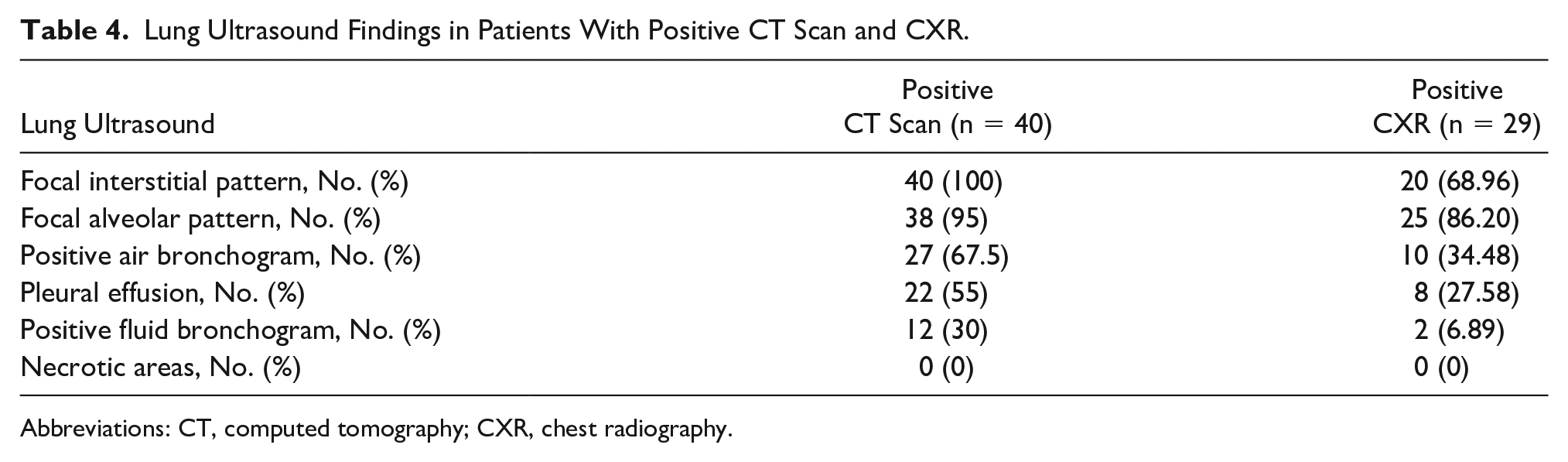
Abbreviations: CT, computed tomography; CXR, chest radiography.
Discussion
This cohort study showed that an emergency physician who performed point-of-care lung sonography has a very good accuracy in diagnosing pneumonia compared with chest CT, which is the gold standard. According to these study results, lung sonography was also superior to the diagnostic accuracy of CXR, in patients with pneumonia. In this study, lung sonography had a sensitivity and negative predictive value of 100%. These results demonstrate that this safe, portable, and available modality has the potential to accurately differentiate patients with pneumonia from those who do not.
These findings may be so promising because the CXR which is the traditional, routine radiologic diagnostic technique in diagnosing the pulmonary pathologies has limited accuracy in this field.13–17 Lichtenstein et al showed in a study of patients with acute respiratory distress syndrome (ARDS) and 10 healthy volunteers that a portable CXR had a diagnostic accuracy of 47% for pleural effusion, 75% for alveolar consolidation, and 72% for alveolar-interstitial syndrome, while in the same study lung sonography had a diagnostic accuracy of 93% for pleural effusion, 97% for alveolar consolidation, and 95% for alveolar-interstitial syndrome. 10 Sonography has some other advantages over a CXR. It is a rapid, safe, noninvasive, and available point-of-care diagnostic technique, which can be used by most practitioners after obtaining a short course focused training. It is a fast procedure and takes no more than 13 minutes to complete, while CXR and a chest CT may take more time (which is so important in overcrowded resource-limited EDs). Another advantage is that it does not expose the patients to ionizing radiation, which is very important in pregnant women. In addition, it does not require that patients be transported to a radiology department, and according to some studies it is more accurate than a CXR in diagnosis of retro-cardiac consolidations. 12
This study, in the ED, showed that emergency physicians accurately found sonographic signs of pneumonia after a focused teaching course. These are comparable findings to studies such as the systematic review by Orso et al. In that review, the authors looked at 17 publications, for a total sample of 5108 patients, with community-acquired pneumonia, reporting to the ED. 18 Orso et al found a sensitivity of 92% and specificity of 93% for lung sonography in detecting the signs of pneumonia. 18 This study concluded that although lung sonography has been accurate in diagnosing pneumonia in adult ED patients, most of the studies reviewed lacked a robust methodology. Therefore, more rigorous clinical trials were recommended to confirm these clinical results. 18 Another systematic review of lung sonography, performed by trained ED physicians, was conducted on 742 patients with clinically suspected community-acquired pneumonia. 19 In the five studies reviewed, a chest CT was performed on 71 patients and used a hospital discharge diagnosis as the reference standard. The authors were able to calculate a pooled sensitivity and specificity for lung sonography of 95% and 90%, respectively. 19 These results were better than that of a CXR, in those study patients. That particular systematic review also reported a small number of well-designed studies performed in the ED, as a research limitation. 19
In this study, the focal alveolar pattern, the focal interstitial pattern, and the positive air/fluid bronchogram were used for the diagnosis of pneumonia, which have different diagnostic values. Alveolar and interstitial patterns are nonspecific signs of pneumonia, which are also seen in other lung pathologies like atelectasis, pulmonary edema, and acute lung injury (ALI)/ARDS. According to some studies, dynamic air bronchogram has a specificity of 94% and positive predictive value of 97% in diagnosing pneumonia. In this study, the focal interstitial pattern was the most useful sign in diagnosing pneumonia in comparison with a chest CT. This study was focused on adult patients, but a review of eight pediatric studies (1013 patients) demonstrated a sensitivity of 93.0% and specificity of 96.0% for a lung sonographic diagnosis of pneumonia. That pediatric study also reported on the pulmonary consolidation, air bronchograms, abnormal pleural line, and pleural effusion as being the most useful sonographic findings for diagnosing pneumonia. 20
Although varied study results on the diagnosis of pneumonia with lung sonography have been promising, there are some reported limitations. Many of the clinical limitations are based on the varied characteristics of patients. For example, some studies have shown that the location of infection is important when assessing a patient for pneumonia. In addition, there have been some concerns about the ability of sonography in detecting deep consolidations and alveolar lesions versus superficial ones. 21 The research indicates that about 8% of the patients with community-acquired pneumonia have a negative sonographic result, although clinically suspected of having the disease. 22 This condition necessitates performing chest CT and underlines the importance of looking at sonography as a tool with some inherited limitations. 22
Limitations
This study was performed in a tertiary-level educational hospital. The ED physicians were experienced in using lung sonography as a part of their daily practice of performing many focused assessments with sonography for trauma (FAST) examinations. Other studies in different settings with different operators including internal/infectious disease medicine residents or specialists who meet the patients with pneumonia frequently can be useful too. Studies on other lung sonography protocols may also help to find more simple and accurate methods of sonography in diagnosing pneumonia. We included patients with positive CT scans for pneumonia, and this can increase the rate of positive and negative predictive values falsely.
Conclusion
Emergency physicians can accurately diagnose pneumonia with a point-of-care lung sonogram, compared with a chest CT, after completing a focused sonography course.
Footnotes
Ethics Approval
The institutional ethics committee approved this multicentered study. The work was carried out in accordance with the Declaration of Helsinki (1989).
Informed Consent
Informed written consent was obtained from all patients or their legal guardians.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because the study was not performed on animal sample and it followed the Declaration of Helsinki.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.