
Abstract
Point-of-care sonography is a valuable tool used in medical practice. A free health clinic was the venue for the authors’ approach to hands-on training for medical and nursing students. Students were surveyed before and after the event regarding their experience and their ability to successfully perform six targeted sonographic skills. The primary outcome was the change presurvey to postsurvey in the students’ assessment of their ability to perform scans on patients and identify the anatomic structures in the six skill areas. An experienced sonographer monitored each scan and confirmed skill application. One hundred nineteen sonograms were performed. Most students (23/29) did not report competence in any of the six assessed skills prior to the study. On average, students developed competence in three of six skill areas. Before the study, 3 of 29 students (10%) reported being able to perform scans on patients and identify the major anatomic structures. After the study, 20 of 28 students (71%) reported that they could perform scans and identify these structures. This change was significant (P < .0001, χ2).
Keywords
The use of point-of-care sonography in clinical practice continues to expand rapidly. Sonographic imaging devices are increasingly seen in intensive care units, emergency departments, surgical floors, and pediatrics floors. They are also gaining use in internal medicine, obstetrics/gynecology, gastrointestinal medicine, urology, and cardiology offices.1–3 It is valuable for physicians and nurses to understand the indications, limitations, and techniques for point-of-care sonography. Emergency physicians and surgeons would like more immediate answers for detrimental medical decision making. 4 The use of less invasive and non-ionizing imaging techniques is becoming more widely accepted throughout medicine. Physicians are checking for intrauterine pregnancies, gallstones, and kidneys as an extension of their physical examination with point-of-care sonography when indicated to get the answers they need to make better decisions for their patients. By educating medical and nursing students on the use of point-of-care sonography, practitioners can learn safely and more efficiently and in the future provide an extension to the quality of care to treat patients. 5
The setting for this study was a rural free health clinic staffed by more than 200 volunteers. 5 The four-day clinic is one of the largest free health care events in the United States, treating thousands of patients in the setting of a county fairground. Services rendered at the event include dental care, vision care, audiology, pharmacy, endocrinology, general medicine, otolaryngology, gastrointestinal medicine, gynecology, nephrology, neurology, cardiology, dermatology, plastic surgery, and podiatry. 6 Imaging services include plain radiography, mammography, echocardiography, and sonography. 7
This pilot study included introducing a limited number of point-of-care sonography skills to novice students. An experienced sonographer instructed them. This approach was not intended to produce competency or volume of standards as established by various professional societies. 4 Rather, it represents an effort to describe and introduce one possible approach for nontraditional users in a hands-on patient environment.
Student evaluations from prior events indicated that their sonography experience was the first and only exposure they had received to this technology during their medical and nursing school training. 8 They had observed sonograms of the kidneys, liver, gallbladder, uterus, soft tissue, and aorta. Medical and nursing students are a key component of the volunteer team at the free health care event and participate in the program either voluntarily or through an elective course at their attending university.
Materials and Methods
Study participants were 15 medical and 14 nursing students who volunteered at a free medical event. Incentive wages were not given, nor were students obligated to participate in the study while attending. This project was approved by the Internal Review Board for the social and behavioral sciences. The project was classified as exempt, and consent for our students to participate was not required.
A Web-based survey was used to collect data regarding prior knowledge in sonography (Figure 1). Students were contacted via e-mail and asked to complete an online survey pre- and postevent regarding exposure to sonography and their self-assessed ability to successfully perform six targeted sonographic skills: (1) differentiating an artery from a vein, (2) visualizing the kidneys and bladder, (3) visualizing the gallbladder, (4) visualizing the aorta, (5) assessing the abdomen and chest for free fluid, and (6) visualizing the uterus.
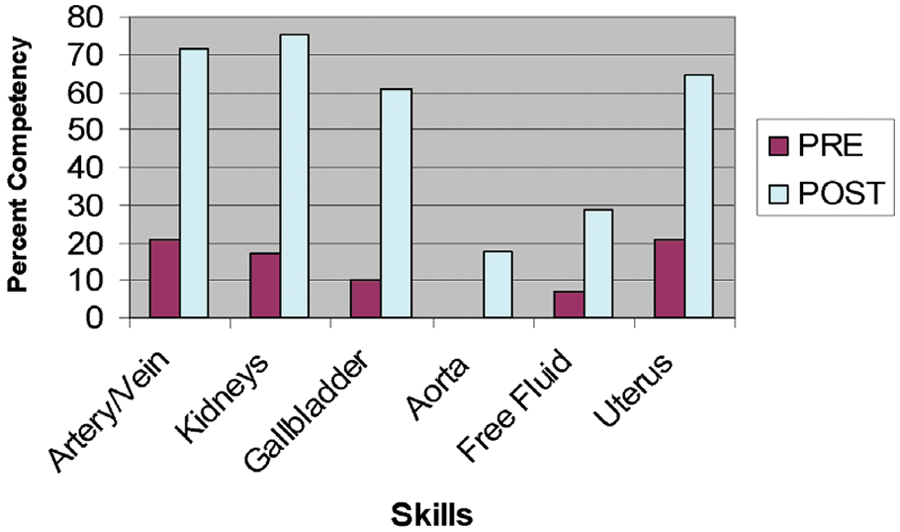
Sonography skills pre- and posttest.
After the presurvey was completed, a sonographer-instructed educational workshop included a 60-minute didactic session on physics, instrumentation, and artifacts followed by a 90-minute lab where each student scanned five of the skills. Imaging of the uterus was not per-formed during this lab session. No images were saved at this time. Handouts on sonographic terminology, specific pathology, and images were provided for review. Additional reading materials and Web sites were suggested for self-study.
During the health event, the sonology area was housed in a tent with two examination areas. The volunteer physicians at the event had the ability to refer patients for needed studies. One hundred nineteen sonograms were performed at the event.
All of the students were instructed to rotate through the sonology area for a three-hour session. During this time, the students introduced themselves to patients and explained that they would be participating in their sonographic evaluation. The patients were not the subject of research; they were not required to fill out a consent form. Students performed examinations while instructed by a sonographer and kept logs of sonograms performed. All of the sonograms performed were saved to the sonographic equipment’s internal hard drive. A Registered Diagnostic Medical Sonographer (RDMS) was present to supervise the students while they performed sonograms. The sonographer scanned each patient as well after each student to verify results. The student’s experience in performing the six targeted skills was indicated with a checkmark to their skills log and signed off by the supervising sonographer. After the event, the images saved were interpreted by an American College of Radiology (ACR) Board-Certified Radiologist, and a report was generated.
Students completed an exit survey to assess their experience not only at the event but also about the sonography rotation. The students retook their pretest to reassess their exposure and experience to the skills learned. An online survey was sent out three months after the event to evaluate how many students continued to explore their sonography skills (Figure 2).
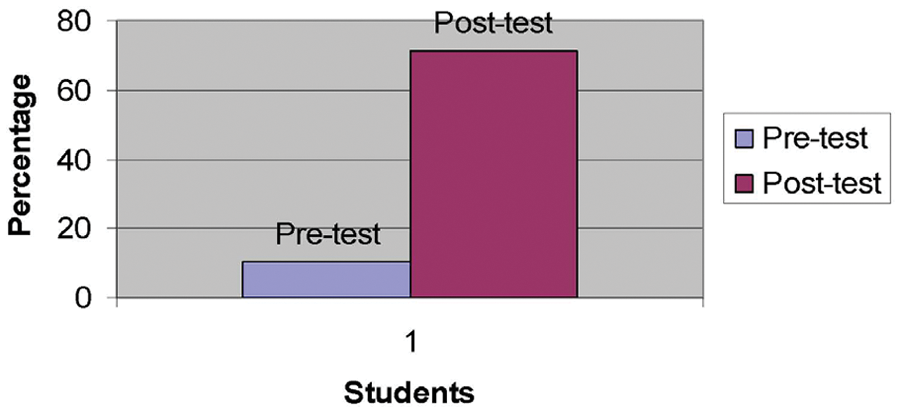
Pre- and posttest reports the ability to perform sonography scans on patients and identify major anatomic structures.
Results
The overall survey response rate (pre and post) was 92%. The primary outcome variable was the ability to perform the six basic skills as self-reported on the pre- and postsurvey. Before the study, 3 of 29 students (10%) reported the ability to perform sonograms on patients and identify major anatomic structures.
After the study, 20 of 28 students (71%) reported the ability to perform sonography scans on patients and identify major anatomic structures (Figure 2). This change was significant (P < .0001, χ2). The students’ self-reported ability in the six basic skills was consistent with that observed by the training sonographer.
On the postsurvey, students reported that sonography training was a useful clinical skill (27/28, 96%) that they expected to learn and use in their future clinical practice. At the three-month follow-up survey, 17 of 21 respondents (81%) believed that basic sonography education should be offered as an elective in medical and nursing school.
Other reported anatomical structures identified by students and sonographers included locating the ovaries, the liver and its vascular components, the thyroid gland and its relation to the internal jugular vein and carotid artery, lymph nodes in the groin, early detection of an intrauterine pregnancy and presence of fetal heart motion, testicular sonographic appearance, and the use of color Doppler. Pathology found included the following: leiomyomas of the uterus, endometrial polyps, endometrial fluid, endometrial hyperplasia, ovarian cysts, polycystic ovaries, gallstones, gallbladder polyp, kidney stones, chronic renal parenchyma disease, epididymal cyst, fatty infiltration of the liver, hemangioma of the liver, thyroid nodules, and palpable lipoma.
Discussion
Sonography education is part of the medical school curriculum at a limited number of medical schools.9,10 Some point-of-care sonography skills taught early in medical and nursing education could provide a foundation for all medical subspecialties. This was a pilot study that included introducing a limited number of point-of-care sonography skills to novice students. This approach was not intended to produce competency or volume of standards as established by various professional societies. 4 Rather, it represents an effort to describe and introduce one possible approach for nontraditional users in a hands-on patient environment. Most sonographic medical education is sought out during postgraduate medical education and thereafter in the form of weekend didactic courses or courses taught by equipment manufacturers themselves. 11
Currently, there is not a standard approach to the initial exposure of novice medical or nursing students to learn sonography. Nursing and medical school faculties are looking for innovative ways to teach. In 1998, schools of medicine put a greater emphasis on self-directed learning, problem-based learning, education in community-based and managed-care settings, and education for continual improvement. 12 Sonography education can be used to demonstrate all of these values. Furthermore, the earlier medical and nursing students are introduced to this technology, the earlier they can implement it and the more experience they will have prior to independent practice.
During medical school, students can elect to do a rotation in radiology. As a part of that rotation, these students have a chance to learn and practice sonography guided by radiologists and sonographers. If radiologists and sonographers do not teach this skill, others will. 13 Sonographers’ level of expertise is crucial in the education of these soon-to-be medical professionals. A crucial piece is missing in the implementation of the learned skill when this happens. Sonography cannot be truly understood by reading a book, viewing a video, or watching someone else do it. Hands-on training and support to reinforce the skill are needed to ensure sonograms are performed appropriately. 14 The current study shows it is feasible for sonographers to educate nonconventional users in their sonography education and that it would be of high value in medical curricula.
Sonographic imaging and interpretation is a specialty field that requires extensive training and experience to master. 15 No brief course or curriculum can reproduce or be a substitute for this training and experience. Hospitals, as well as national and international safety guidelines, strongly recommend the use of sonography equipment in central venous access, a critical procedure with significant potential complications that was routinely performed “blindly” before clinical use of sonographic imaging. Using a sonography machine to see and access the vein greatly increases the safety of this procedure. According to the American College of Emergency Physicians, to prepare physicians to use sonography for central venous access, a uniform, validated educational model must be developed. It is also recommended that a clerkship be provided to fourth-year medical students for emergency sonography that would entail online didactic instruction to maximize the students’ hands-on experience. The goal would be to obtain 100 scans within this time period. 4
Sonography education is a part of some first-year curriculum in some medical schools, with students using handheld sonographic imaging devices.9,10
One major limitation of this study is the reliance on survey data and student self-reports. This study was performed at a four-day event with a limited number of student participants and sonographic examinations. Some student participants were not able to practice all six skills based on the indicated examinations during their rotations through the sonology area. It is also possible that the students reported competence on the survey that they did not actually possess. It is notable, however, that an RDMS sonographer was present at the bedside for each patient scanned and that this sonographer repeated the scan to verify students’ findings in real time. This confirmation was reflected on the students’ log and signed off by the supervising sonographer. Survey data reported in this study were entirely consistent with skill acquisition logged examinations.
This interdisciplinary approach proved to be a valuable introduction of novice medical and nursing students to six clinical point-of-care sonographic skills during a free health care event. This was a valuable way to educate the limited number of students attending. The students expressed a better understanding of patient clinical assessment and anatomy after this experience. Although this study did not perform standardized assessment of students’ skill, such assessment will be important to future studies in this area. This initial effort establishes the feasibility of using free health care events as a venue for exposing nursing and medical students to sonography early in their training.
Footnotes
Appendix
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This study was funded by the University of Virginia, Academy of Distinguished Educators for Undergraduate Medical Education Research. This project was approved by the Internal Review Board for the social and behavioral sciences. The project was classified as exempt and consent for our students to participate was not required.