
Abstract
Metamizole-induced agranulocytosis is a rare adverse drug reaction with common infectious complications. In this context, pyomyositis of the extremities has not yet been described. Usually, pyomyositis is treated with a combination of antibiotics and surgical intervention. Sonography is described as diagnostic tool for pyomyositis but without defined concrete characteristics for follow-up. This case report describes a widespread pyomyositis due to a metamizole-induced agranulocytosis, which was treated conservatively, using sonography for surveillance.
Metamizole is a frequently used basic non-opioid analgesic acting by cyclooxygenase inhibition. Due to fewer renal adverse effects, metamizole is favored over non-steroidal anti-inflammatory drugs in patients with impaired renal function. However, metamizole-induced agranulocytosis is a rare adverse drug reaction with ongoing debates about safety and incidence. 1 There are regional differences in incidence, but especially in Switzerland, there was a significant rise in reports of agranulocytosis, during 2010 to 2017. It is associated with a relevant mortality of 20%, mostly because of infectious complications. 2 The following risk factors elevate the likelihood of this adverse event: a history of allergies, previous leucopenic episodes, hepatitis C infection, and concomitant cytostatic agents. 3 So far, association to pyomyositis in these situations has only been reported in the cervical region of the neck. 4
Pyomyositis was formerly described as tropical pyomyositis. Despite the high incidence in tropical areas, it also appears in other regions such as middle Europe. 5 Associations with HIV-infection, hematologic disorders, and chemotherapy-induced agranulocytosis have been reported.6–8 The main treatment includes a combination of antibiotic drug therapy and surgical intervention.9,10 Reports of patients having been treated without surgical intervention are rare and are mainly related to children. 11 Sonography is described as diagnostic tool in primary pyomyositis, especially in children. 12
Case Report
A 56-year-old woman presented to our emergency department 7 weeks after hip arthroplasty due to a general deterioration in condition, which had started 1 week before with fever, diffuse myalgia, arthralgia, and unproductive cough. The patient’s medical history was remarkable for an HIV infection diagnosed in 1992, degenerative bone disease, and bronchial asthma. Due to the total hip arthroplasty, the patient took metamizole up to 4000 mg/day, until the day of presentation.
She presented in a reduced general state of health, hemodynamically stable with a peripheral oxygen saturation of 95% on ambient air and a body temperature of 37.3°C. The clinical examination showed fine expiratory pulmonary crackles and a systolic heart murmur. Laboratory investigation revealed a C-reactive protein of 284 mg/L, pancytopenia (Hemoglobin 104 g/L, neutropenia < 0.1 g/L, and thrombocytopenia 117 g/L) as well as elevated d-dimer of 1112 mcg/L. Urine, blood, and stool cultures were negative and the HIV virus load was unmeasurably low. The serological examination for hepatitis B and C was negative. Investigating the chance for Epstein-Barr virus and cytomegalovirus, there was only an elevation of immunoglobulin G, indicating a previous infection. Computed tomography of the lung showed multiple nodular compressions, without signs of pulmonary embolism. In the transesophageal echocardiography, no valvular vegetations were visible and the magnetic resonance tomography of the spine showed no signs of spondylodiscitis. Bone marrow biopsy revealed findings compatible with toxic damage.
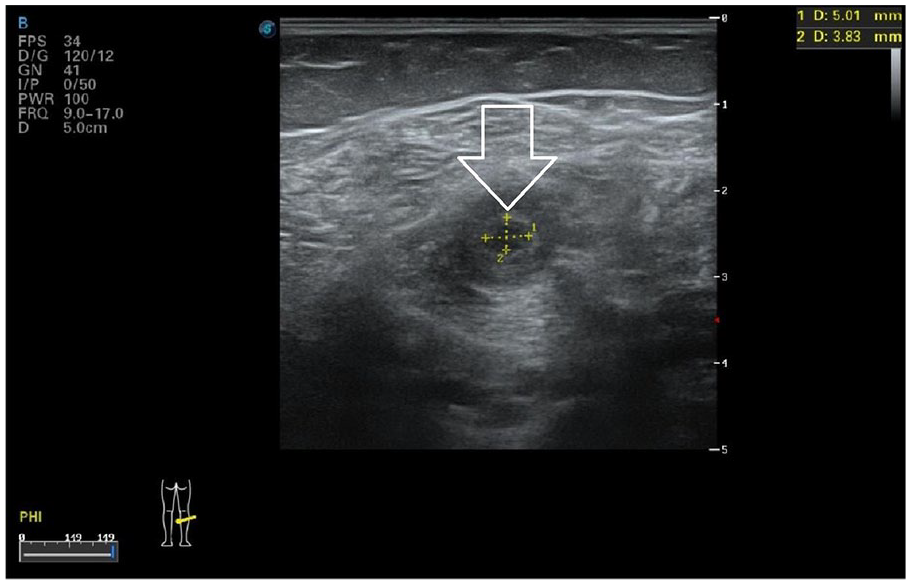
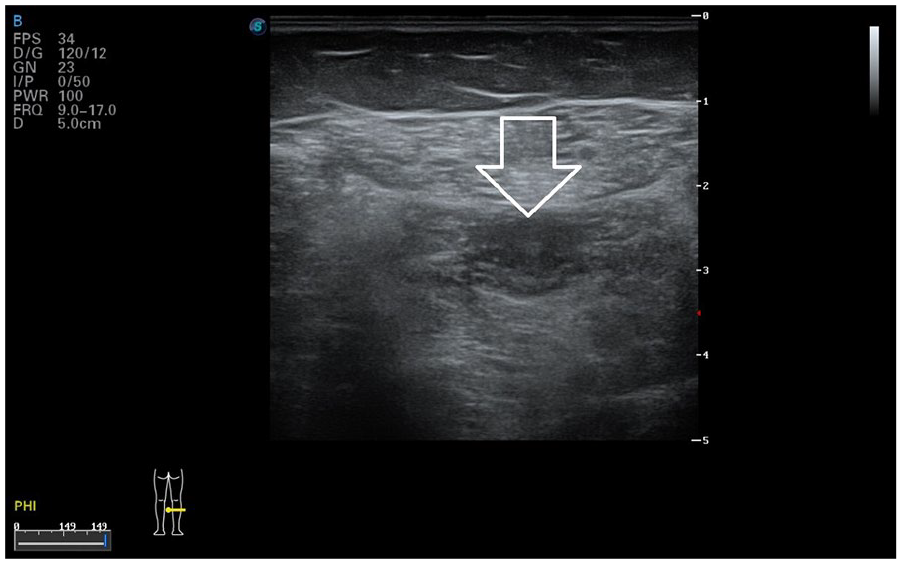
In the following days after presentation, the patient developed painful, slightly red areas of swelling in the region of the neck and all 4 extremities. On the corresponding sonogram of the affected areas, a lot of intramuscular hypo- and hyperechogenicities were found. The larger foci appeared as oval, anechoic lesions, surrounded with hyperechoic tissue, and hypervascularisation (see Figure 1). Besides the typical abscess-like lesions, smaller foci were identified that appeared only hypoechoic without anechoic parts (see Figure 2). In some areas, these alterations were very small and without optical manifestations on skin level, but still explained the pain at this location. In some body regions, only asymmetric diffuse hyperechogenicitiy of the muscle was present (see Figure 3). Complimentary magnetic resonance tomography of the largest muscle abscess of the left lower leg confirmed characteristics of purulent material (see Figure 4). In summary, the findings were interpreted as metamizole-induced agranulocytosis, with consecutive pyomyositis of multiple foci. In common practice, abscesses in pyomyositis are surgically drained. In the present case, surgical consultation advised against drainage due the multiple foci. To monitor the healing process, a close follow-up with sonography was planned.
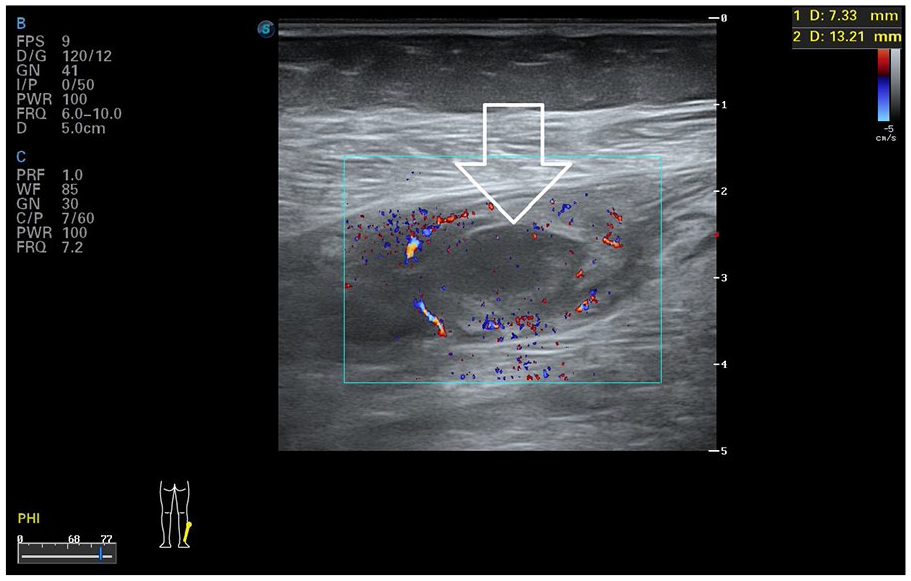
Sonography with color Doppler of the muscular abscess of the left lower leg with the clinical important anechoic central area. In common practice, the situation for a surgical drainage.
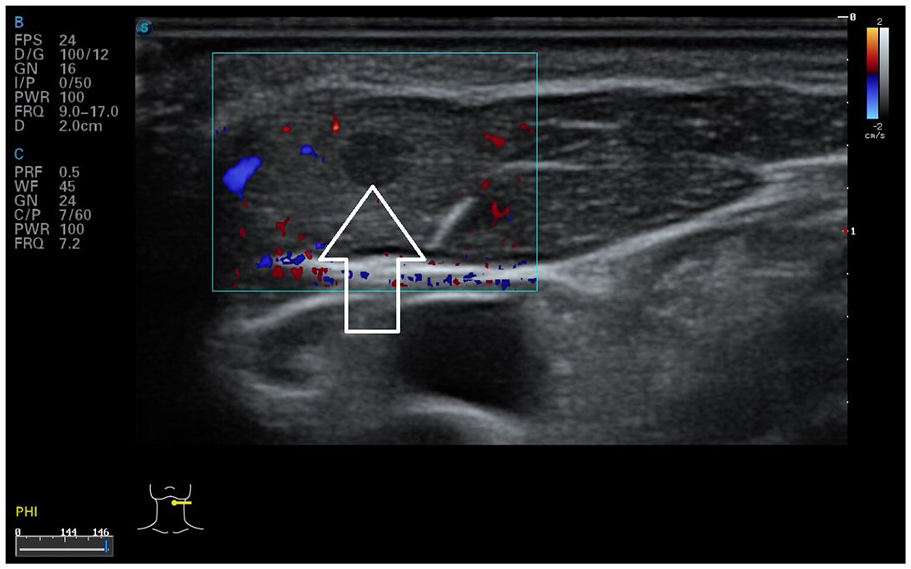
Sonography with color Doppler of a small hypoechoic lesion in the left muscle sternocleidomastoideus without anechoic area. There were no visible alterations on skin level at this place.
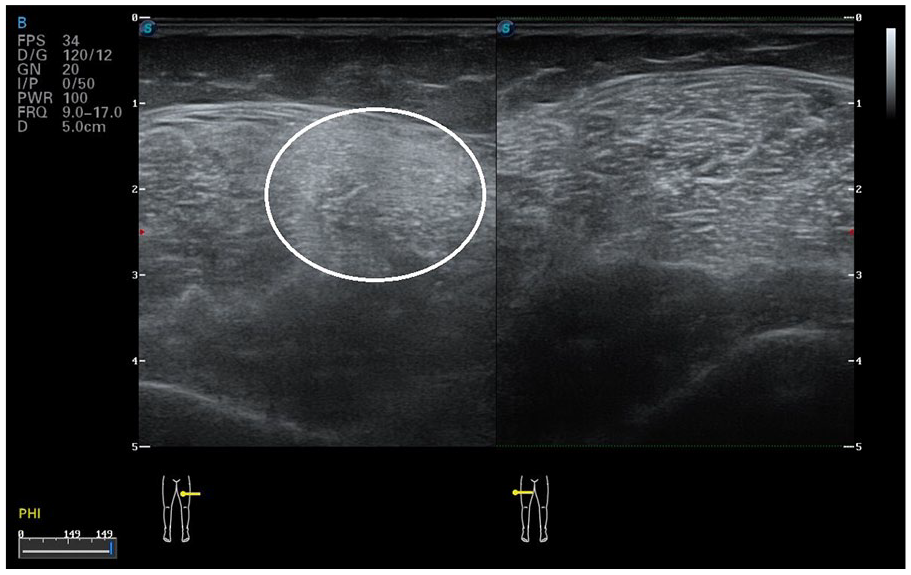
Sonography of the asymmetric diffuse intramuscular hyperechogenicity in the left upper leg which shows a fast resolution under antibiotic therapy.
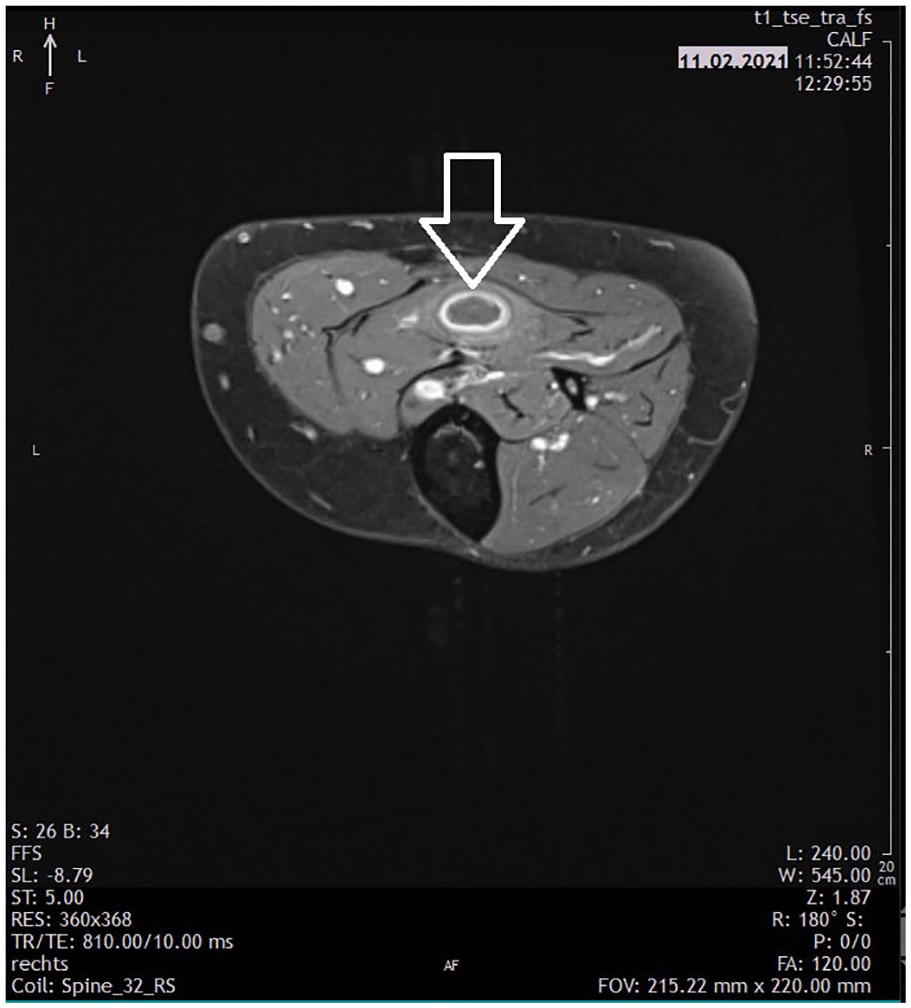
T1-sequence of the magnetic resonance tomography (MRT) of the muscular abscess of the left lower leg.
With prompt cessation of metamizole intake, the administration of granulocyte colony-stimulating factor (G-CSF) and an extended antibiotic therapy with cefepime, normalization of neutropenia and regression of the inflammatory markers were achieved. The patient was discharged in better condition on the 18th day of hospitalization.
In a weekly manner, evolvement of the lesions was monitored by sonography. During the following weeks, the major lesions decreased in size but kept their anechoic centers (see Figure 5). The smaller foci without anechoic areas showed a much faster healing process than the ones with anechoic areas. The diffuse asymmetric muscular hyperechogenicity resolved earlier than the abscess-like lesions. After 6 weeks of overall antibiotic therapy (1-week cefepime, 5 weeks amoxicillin-clavulanate), there were only minimal residual findings on sonography, without anechoic areas (see Figure 6). Thus, the antibiotic treatment was discontinued. The following healing process showed no deterioration. Six months later, the patient reported no clinical signs or relapsing symptoms.
Sonography of the muscular abscess of the left lower leg 3 weeks later. We saw a shrinking but still visible anechoic area and that was why we continued antibiotic therapy.
Sonography of the residuum of the muscular abscess on the left lower leg at termination of antibiotic therapy. There was no more anechoic central area.
Discussion
The infectious complications of metamizole-induced agranulocytosis are known and relevant. 2 Because data on agranulocytosis-associated widespread peripheral pyomyositis are rare; therefore with this patient, extensive diagnostics were performed to identify the etiology of pyomyositis and rule out differential diagnoses in this patient. Since no sources for septic embolization were identified, the association of pyomyositis to agranulocytosis seemed reasonable. Reports on the appearance of pyomyositis in the context of chemotherapy-induced agranulocytosis supported this hypothesis. 8 Because there is a fair amount of described metamizole-induced agranulocytosis, without remarkable notification of peripheral pyomyositis, it can be assumed that spontaneous resolution is the usual course of the condition. Nevertheless, the condition of pyomyositis should be considered early since the significant mortality of agranulocytosis is mainly due to infectious reasons.
In the present case, the identification of multiple peripheral foci, of purulent material, justified a conservative treatment and the need for surgical intervention was waived. Sonography offered a good option to handle surveillance of this clinical situation. The incomplete resolution of the anechoic areas would have been noticed during follow-up and secondary surgical treatment could have been initiated. Sonography allowed for a safe monitoring of the patient’s healing process. It can be hypothesized that the need for antibiotic treatment is linked to the presence of anechoic areas and therefore sonography can help determine the duration of antibiotic therapy. The observation of a faster regression of lesions with only hypoechoic or hyperechoic areas may be supported by this hypothesis.
It was of special interest, that even in slightly painful or areas only tender to touch, sonographic correlations without any visible alterations on skin level were identified. Sonography seems a very sensitive method to detect even the smallest number of inflammatory alterations in muscular tissue. Therefore, it can be assumed that pyomyositis in agranulocytosis might occur more often than previously described, but remains undetected since major pain, visible alterations on skin level or other complaints are not necessarily present.
Even though, this is an individual case with a hypothesis based on the author’s experience throughout the follow-up process, it seems reasonable to consider this approach, particularly in cases of multiple foci of pyomyositis. In case of multiple foci with purulent material and a hemodynamically stable patient, conservative management with antibiotic therapy alone and close follow-up should be evaluated. Naturally, weekly follow-up with sonography is necessary in this case to ensure proper healing. As soon as the anechoic areas are no longer sonographically visible, antibiotic therapy can be terminated.
Conclusion
This case report demonstrates the option of successful handling diffuse secondary pyomyositis, without surgical treatment in adults. Since this is an individual case, it is clearly not possible to generalize and draw conclusions for all patients. Sonography was a very useful tool in the follow-up of a successful healing process in this patient. Therefore, it may be reasonable to consider sonography as not only a diagnostic tool in pyomyositis, 12 but also for surveillance. This case description together with documentation of the lesions, their evolvement over time, and their polymorphism might serve as a guidance in the interpretation of the sonographic findings in pyomyositis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was not sought for the present study because it doesn’t apply.
Informed Consent
Oral and written informed consent for publication was obtained from the patient.