
Abstract
Secondary hyperparathyroidism (SHPT) is one of the most common abnormalities of mineral metabolism in patients with chronic kidney disease. This case study is a report of a patient referred for sonography based on computed tomography findings of multiple supraclavicular lymph nodes. Sonography was able to localize two enlarged parathyroid glands (adenomas) and to guide fine-needle aspiration for histopathologic tissue diagnosis in this patient with SHPT.
Secondary hyperparathyroidism (SHPT) is one of the most common abnormalities of mineral metabolism in patients with chronic kidney disease (CKD). It is characterized by hyperplasia of the parathyroid glands and increased plasma levels of parathyroid hormone (PTH). The resulting disturbances in vitamin D, phosphorus, calcium, and PTH metabolism lead to bone disorders and multiple cardiovascular complications that contribute to the excessive morbidity and mortality of patients with end-stage renal disease (ESRD). 1 Sonography has been shown to be a valuable modality for the detection of enlarged parathyroid glands in patients with SHPT. 2
Case Report
A man in his 60s with a history of ESRD secondary to focal segmental glomerulosclerosis underwent a computed tomography (CT) pulmonary embolus study for new onset of atrial flutter. Incidental findings of multiple suspicious supraclavicular lymph nodes led to a referral for a neck sonogram. Sonography of the thyroid and neck was performed using a Philips iU-22 ultrasound system (Philips Medical, Bothell, Washington) with a 5- to 12-MHz linear transducer and a 5- to 8-MHz curvilinear transducer. Bilateral hypoechoic solid nodules corresponding to the CT findings were noted posterior to each thyroid lobe (Figure 1). The right nodule measured 1.3 × 1.2 × 1.2 cm, and the left nodule measured 1.8 × 1.1 × 1.6 cm (Figures 2 and 3). Both nodules showed mild peripheral color Doppler flow (Figure 4) and were considered suspicious for parathyroid adenomas. Exophytic thyroid nodules and lymphadenopathy were thought to be less likely. In addition, an ill-defined slightly heterogeneous isoechoic nodule was found in the mid-portion of the right thyroid lobe. This nodule measured 1.2 × 1.1 × 0.9 cm and had peripheral color Doppler flow but no other suspicious sonographic features. No abnormal central or lateral lymph nodes were noted during this examination.
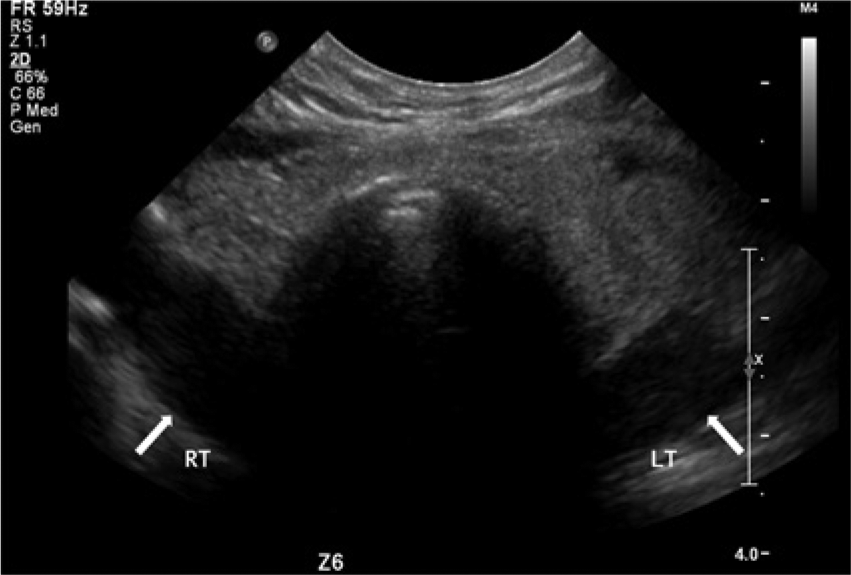
Transverse image of the neck showing bilateral hypoechoic masses (arrows) posterior to the thyroid gland.
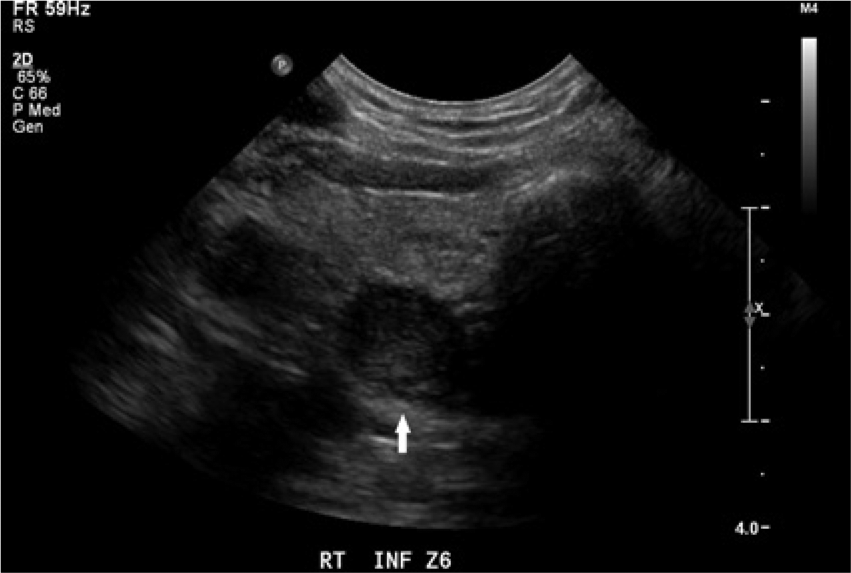
Transverse image of the right thyroid gland showing a round hypoechoic mass (arrow) posterior to the gland.
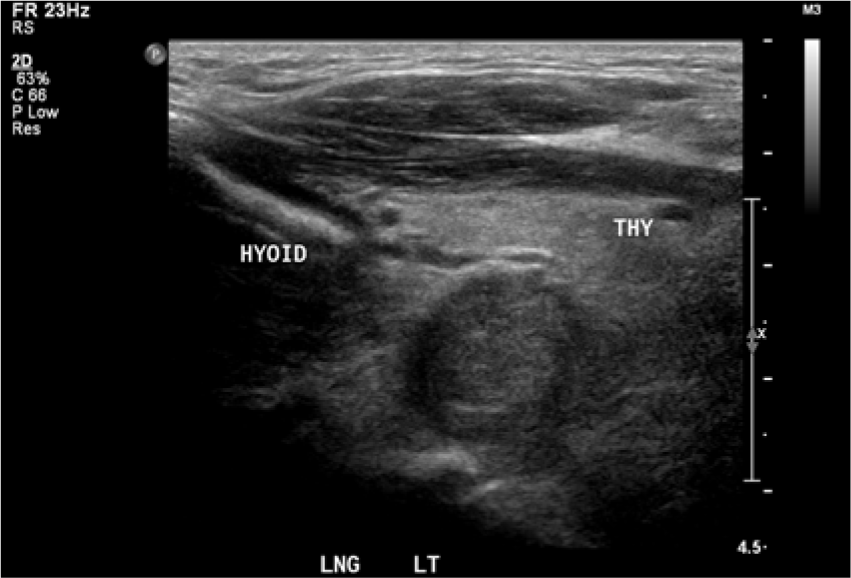
Longitudinal image of the hypoechoic mass inferior to the hyoid bone and posterior to the left thyroid gland.
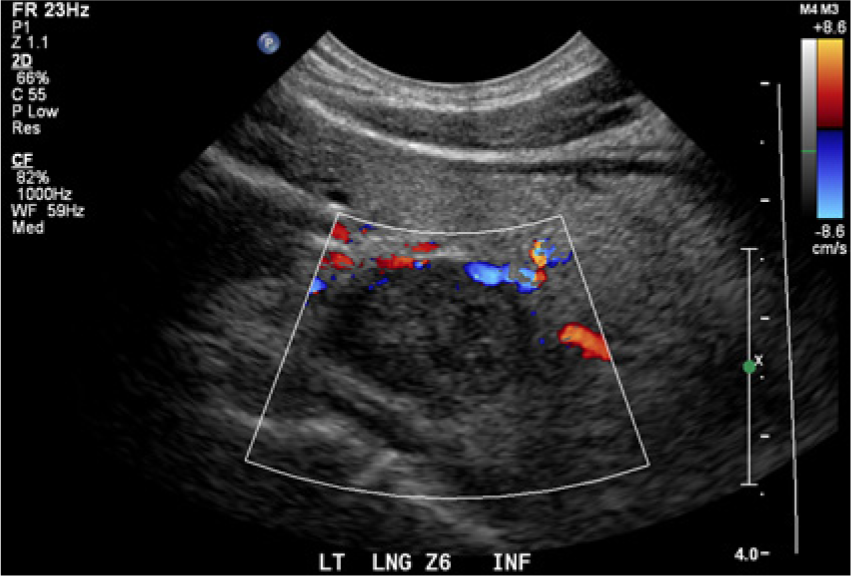
Color Doppler longitudinal image of the mass inferior to the left thyroid gland showing peripheral flow.
Ultrasound-guided fine-needle aspiration was performed on each nodule. Biopsy confirmed the bilateral posterior nodules to contain parathyroid cells. The mid-right thyroid nodule was found to be a benign follicular nodule with focal cystic degeneration. At the time of the sonogram, the patient’s laboratory values showed high parathyroid hormone, calcium, and phosphorus serum/plasma levels, which were all consistent with a diagnosis of SHPT. The patient also had elevated serum urea nitrogen and creatinine levels and a low glomerular filtration rate (GFR). He is currently being treated with chronic hemodialysis (HD), B complex vitamin, and sevelamer carbonate (Renvela; Sanofi-Aventis, Bridgewater, New Jersey) to treat his CKD and cinacalcet (Sensipar; Amgen, Thousand Oaks, California) to reduce the PTH level.
Discussion
Parathyroid hormone is secreted by the parathyroid gland and functions to maintain ionized calcium and phosphate within a normal reference range by stimulating specific receptor-mediated responses in cells throughout the body. If a decrease in circulating ionized calcium occurs, PTH increases, which triggers three major processes aimed at restoring a normal circulating concentration: receptor-mediated tubular reabsorption of calcium occurs in the kidneys, stimulation of osteoclast resorption to release skeletal calcium occurs in the bones, and production of vitamin D and an increase in calcium absorption occur in the bowel. Once an appropriate calcium level is achieved, PTH secretion is decreased via a classic endocrine feedback loop. A disruption of any component of this regulatory system may cause excessive secretion of PTH and hyperparathyroidism. 3
Secondary hyperparathyroidism is a common complication in CKD, characterized by an increase in PTH and disorders of parathyroid cell proliferation. 4 The prevalence of SHPT increases as the GFR decreases. 5 Secondary hyperparathyroidism develops in CKD as an adaptive response to the lowered ionized calcium level that occurs as a result of deteriorating renal function. A combination of additive factors contributes to the increase in PTH, since GFR decreases with progressive stages of CKD. As GFR falls, phosphate is increasingly retained and hypocalcemia progresses, both of which stimulate the synthesis and secretion of PTH. The circulating vitamin D level decreases in response to a reduction in functional renal tissue. 3 Parathyroid gland hyperplasia occurs as the parathyroid gland compensates for the low serum calcium levels. 6 Secondary hyperparathyroidism is a significant contributing factor in metabolic bone, multiple cardiovascular complications, fractures, and the increased morbidity and mortality of patients on hemodialysis. 4
Chronic renal failure is best treated with renal transplantation, which should successfully restore vitamin D metabolism and prevent the progression of SHPT. 6 When renal transplantation is not an available option, alternative treatment of SHPT includes oral or intravenous administration of calcium or non–calcium-based phosphate binders to reduce blood serum levels. 1 The administration of vitamin D analogues may be used to prevent the progression of bone disease. Cinacalcet is a calcimimetic drug that is used in the treatment of CKD to reduce the secretion of PTH in patients undergoing hemodialysis or peritoneal dialysis. Typically, however, combinations of medications are needed to successfully treat patients with SHPT. 3 In addition, two surgical options are available to treat SHPT. These include total cervical parathyroidectomy with immediate heterotopic transplantation of parathyroid tissue to a distant site, often the forearm, or a subtotal parathyroidectomy, leaving a remnant of well-vascularized parathyroid tissue in the neck. 6
Most individuals have two superior and two inferior parathyroid glands. The superior glands are usually located posterior to the middle or superior portion of the thyroid gland. There is more variability in the location of the inferior glands, but they are most often found inferior or just posterior to the lower pole of the thyroid gland. The average size of a normal parathyroid gland is 5 × 3 × 2 mm. Thus, normal parathyroid glands are rarely visualized sonographically because of their small size and insufficient acoustic differentiation from surrounding tissue. In contrast, parathyroid adenomas and hyperplasia are usually hypoechoic because of their compact cellularity relative to thyroid tissue. Parathyroid adenomas are usually well-circumscribed solid masses that are ovoid, bilobed, triangular, or longitudinal in shape. 7 Parathyroid adenomas generally have a similar appearance to hyperplastic glands but tend to be somewhat more echogenic. Patients with SHPT do not always have symmetric enlargement of the parathyroid glands. 2 Sonographic evaluation of SHPT is usually accurate in showing the number and size of parathyroid glands as well as their echostructural and vascular patterns. Sonography has been found to correlate well with the severity of SHPT and is an effective means of monitoring the therapeutic outcome of patients with moderate disease. 8
Conclusion
Secondary hyperparathyroidism is a common complication in CKD. This diagnosis is important for the management and treatment of bone and cardiovascular problems that may result from SHPT and lead to early mortality. Sonography aids in the detection and diagnosis of SHPT and in the monitoring of these patients during their treatment. Sonography provides a simple and effective means to differentiate thyroid and lymph node pathology from parathyroid adenomas or hyperplasia in patients with SHPT.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.