
Abstract
Objective
This retrospective study investigated the characteristics of secondary hyperparathyroidism (SHPT) by examining the presence of the calcium-sensing receptor (CaSR) and the rate of cell proliferation and apoptosis in parathyroid glands.
Methods
Eighteen diffuse and 57 nodular hyperplastic parathyroid glands from 24 patients with SHPT were compared with 14 primary adenomas and 33 normal parathyroid glands using immunohistochemical staining of CaSR and a marker of proliferative activity (Ki67 antigen). Apoptosis was measured using the terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick end labelling assay.
Results
The mean ± SE labelling index (LI) of CaSR (12.8% ± 1.5%) in nodular hyperplasia was significantly lower than that in normal parathyroid glands (26.8% ± 0.8%), whereas the mean ± SE LI of CaSR in diffuse hyperplasia was similar to that in normal parathyroid glands (23.3% ± 1.8%). The mean ± SE LI of Ki67 antigen was significantly higher in primary adenoma and nodular hyperplasia than in normal parathyroid glands.
Conclusion
These results indicate that downregulation of CaSR, and a higher rate of proliferation over apoptosis, could contribute to the pathological progression of SHPT.
Keywords
Introduction
More than a century after its identification, secondary hyperparathyroidism (SHPT) is still observed in the majority of patients with chronic kidney disease (CKD) stages 4–5.1,2 The main pathogenic factors include the deficiency of active vitamin D production, hypocalcaemia and phosphorus retention. 3 The sustained hyperfunction of the parathyroid gland is attributable to the progressive proliferation of parathyroid cells.4,5
Research has demonstrated that the calcium-sensing receptor (CaSR) plays a central role in regulating parathyroid hormone (PTH) concentrations. 6 PTH secretion is inhibited via the CaSR when it is activated by elevated concentrations of ionized calcium. 7 Prolonged hypercalcaemia eventually leads to reduced parathyroid cell proliferation, which is an effect that is also likely to be mediated by the CaSR. 8 Conversely, low serum levels of ionized calcium reduce activation of the CaSR, and PTH secretion increases. 9
The precise mechanism involved in the control of parathyroid cell growth is not yet completely understood. In particular, the association between proliferation and apoptosis during disease progression remains unknown.10,11 Understanding how proliferation and apoptosis affect parathyroid hyperplasia will likely provide valuable insights into the pathogenesis of SHPT and help improve its treatment.
The present study determined the characteristics of SHPT in patients with CKD by comparing concentrations of CaSR protein in normal parathyroid glands with those in parathyroid glands from patients with SHPT or primary adenoma. Rates of proliferation and apoptosis were also measured in the same parathyroid gland samples.
Patients and methods
Study Population
This retrospective study was conducted at the Department of Surgery, Korea University Guro Hospital, Seoul, Korea, between January 2004 and December 2007; it included tissue samples from consecutive patients who underwent total parathyroidectomy with autotransplantation for severe SHPT and those who underwent parathyroidectomy for primary hyperparathyroidism with a single adenoma. Normal parathyroid glands were obtained from patients who underwent thyroidectomy for thyroid carcinoma, and were used as control samples. There were no additional inclusion or exclusion criteria for the study.
All patients provided written informed consent for samples to be taken and the study protocol was approved by the Ethics Committee of the Korea University Guro Hospital.
Immunohistochemical Analyses of CaSR and Cell Proliferation
Formalin-fixed, paraffin wax-embedded tissue block sections (3 -µm thick) were examined to ensure the integrity of each tissue specimen. The sections were deparaffinized in xylene and dehydrated through a graded series of ethanol. Sections were treated with 0.1 mmol/l citrate, pH 6.0, in an 800 -W microwave oven for 15 min for antigen retrieval. Internal peroxidases were blocked with 3% hydrogen peroxide (H2O2) in methanol for 5 min at room temperature, then incubated with the primary antibodies for 30 min at room temperature: mouse antihuman CaSR antibody (1 : 50 dilution; Santa Cruz Biotechnology, Santa Cruz, CA, USA); and mouse antihuman antiKi67 antibody (1 : 500 dilution; DAKO, Glostrup, Denmark). The slides were then thoroughly washed in 10 mM phosphate-buffered saline (PBS, pH 7.4), followed by treatment with a DAKO EnVision™ system peroxidase kit (DAKO) according to the manufacturer’s instructions. Sections were immunostained using the streptavidin–biotin complex method and were counterstained with haematoxylin and eosin.
TUNEL Assay for Apopototic Cells
Apoptotic cells were detected using a terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick end labelling (TUNEL) assay, using a commercially available kit (Trevigen, Gaithersburg, MD, USA) according to the manufacturer’s instructions. After blocking internal peroxides with 3% H2O2 in methanol for 5 min at room temperature, 50 µl of Labeling Reaction Mix (Trevigen, Gaithersburg, MD, USA) was added and incubated in a humid chamber at 37°C for 1 h. The slides were then covered with 50 µl of streptavidin–horseradish peroxidase solution, incubated for 10 min at room temperature and then for 10 min at 37°C in a humid chamber. After treatment with horseradish peroxidase convertor, sites of apoptosis were visualized with 3,3′-diaminobenzidine and H2O2. Slides were counterstained with methyl green for 2 min.
Quantitative Analyses
Slides were examined under a light microscope (magnification × 100). The numbers of cells staining positive for CaSR, Ki67 antigen and TUNEL were determined by counting a minimum of 1000 cells per slide using Image-Pro® Plus software, version 6.0 (Media Cybernetics, Rockville, MD, USA). The percentage of the positive immunoreactive area per total area (CaSR) and the number of positive immunoreactive nuclei per 1000 parenchymal cells (Ki67 antigen, TUNEL) were expressed as the labelling index (LI).
Biochemical Analyses
To determine preoperative plasma calcium, phosphate, alkaline phosphatase and intact PTH levels, peripheral venous blood samples were taken prior to surgery. The samples were immediately anticoagulated with ethylenediaminetetra-acetic acid and centrifuged at 500 g to obtain plasma. PTH levels were determined with an Elecsys® biochemical analyser (Roche Diagnostics, Indianapolis, IN, USA). Plasma calcium, phosphate and alkaline phosphatase levels were measured using standard laboratory techniques.
Statistical Analyses
All statistical analyses were performed using the SPSS® statistical package, version 12.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Between-group differences were compared using one-way analysis of variance followed by Student's t-test with Tukey’s correction. A P-value < 0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of patients with secondary hyperparathyroidism (HPT) or primary adenoma compared with normal parathyroid glands from patients who underwent thyroidectomy for thyroid carcinoma.

Data presented as mean ± SE.
SHPT group compared with normal parathyroid glands and primary adenoma groups (and compared with primary adenoma group only for plasma intact PTH); one-way analysis of variance followed by Student's t-test with Tukey’s correction.
PTH, parathyroid hormone; NA, not available; NS, no statistically significant differences (P ≥ 0.05).
Preoperative levels of plasma phosphate and corrected plasma alkaline phosphatase were significantly higher in patients with SHPT compared with patients with primary adenoma or normal parathyroid glands (P < 0.05 for both comparisons). The preoperative concentration of intact PTH was significantly higher in patients with SHPT compared with patients with primary hyperparathyroidism (P < 0.05).
The LIs for CaSR, Ki67 antigen and TUNEL assay for each parathyroid specimen type are presented in Table 2. Immunostaining for CaSR protein was mainly localized to the cytoplasm (Figure 1). The LI for CaSR in nodular hyperplasia was significantly lower than in normal parathyroid glands (P < 0.05), but was significantly higher than in primary adenoma (P < 0.05). There were no significant differences in the LI for CaSR between diffuse hyperplasia and normal parathyroid glands or nodular hyperplasia.
Immunohistochemical analysis of calcium-sensing receptor staining (original magnification × 100): (A) normal parathyroid gland showing extensive positive (i.e. brown) staining of cytoplasm; (B) primary adenoma showing sparse cytoplasmic staining; (C) secondary hyperparathyroidism with diffuse hyperplasia showing nearly all of the cytoplasm stained (brown); (D) secondary hyperparathyroidism with nodular hyperplasia displaying sparse cytoplasmic staining (brown). Sections were counterstained with haematoxylin and eosin. Labelling indices (LIs) for the calcium-sensing receptor (CaSR), Ki67 antigen and TUNEL assay results for patients with secondary hyperparathyroidism (HPT) and primary adenoma compared with normal parathyroid glands from patients who underwent thyroidectomy for thyroid carcinoma. Data presented as mean ± SE. TUNEL, terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick end labelling. P < 0.05 vs normal parathyroid glands and primary adenoma groups, bP < 0.001 vs normal parathyroid glands group, cP < 0.01 vs diffuse hyperplasia group, dP < 0.05 vs normal parathyroid glands, primary adenoma and diffuse hyperplasia groups; one-way analysis of variance followed by Student's t-test with Tukey’s correction.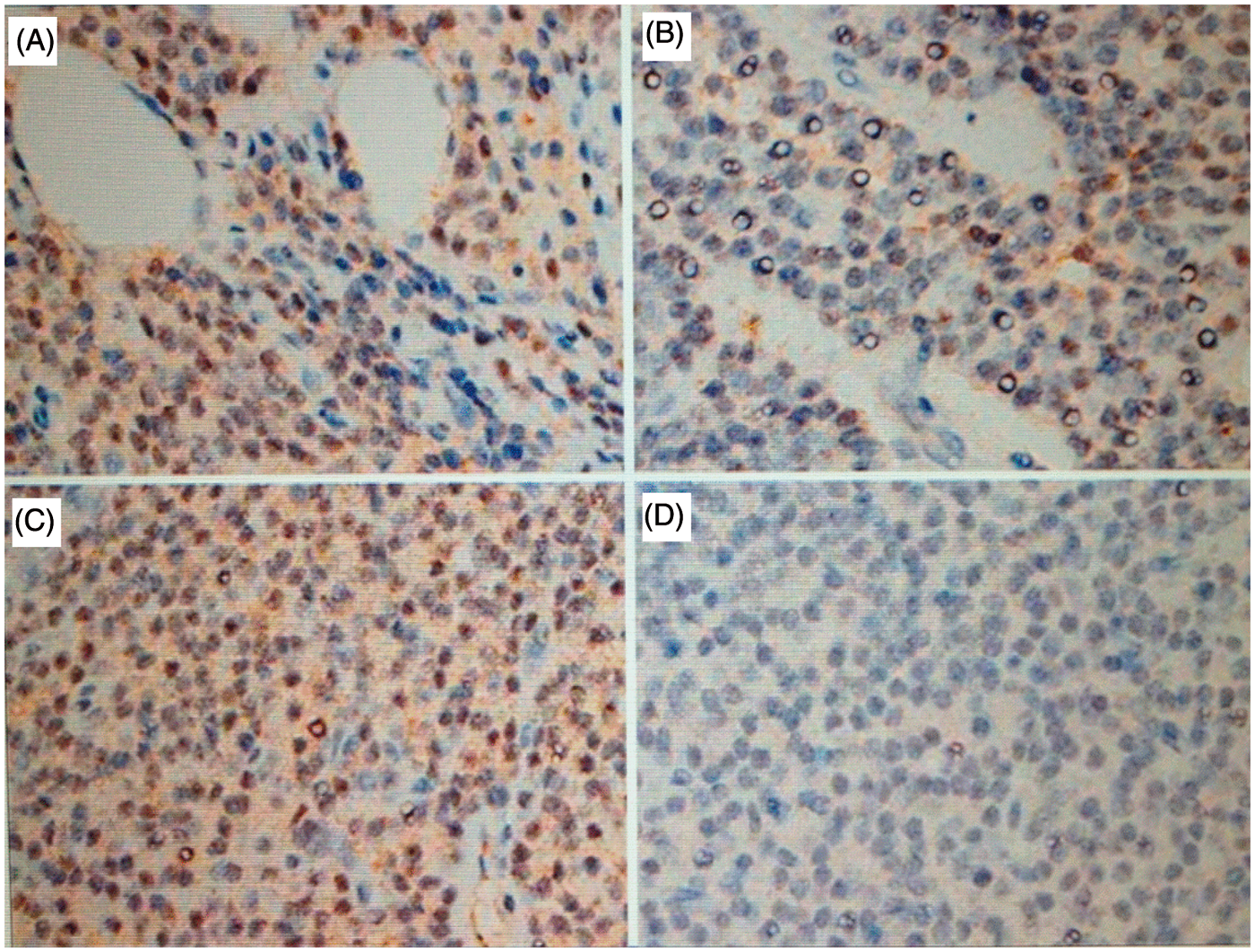

Immunostaining for Ki67 antigen was localized to the nucleus (Figure 2). The LIs for Ki67 antigen were significantly increased in primary adenoma and nodular hyperplasia, compared with normal parathyroid glands (P < 0.001 for each comparison; Table 2). The LI for Ki67 antigen in diffuse hyperplasia was comparable with that observed for normal parathyroid glands, but was significantly lower than that for nodular hyperplasia (P < 0.01 Table 2).
Immunohistochemical staining analyses for Ki67 antigen staining (original magnification × 100): (A) normal parathyroid gland showing few nuclei with positive staining (i.e. brown); (B) primary adenoma showing many nuclei with staining (brown); (C) secondary hyperparathyroidism with diffuse hyperplasia showing only one nucleus in the field staining positive; (D) secondary hyperparathyroidism with nodular hyperplasia showing staining in some nuclei. Sections were counterstained with haematoxylin and eosin.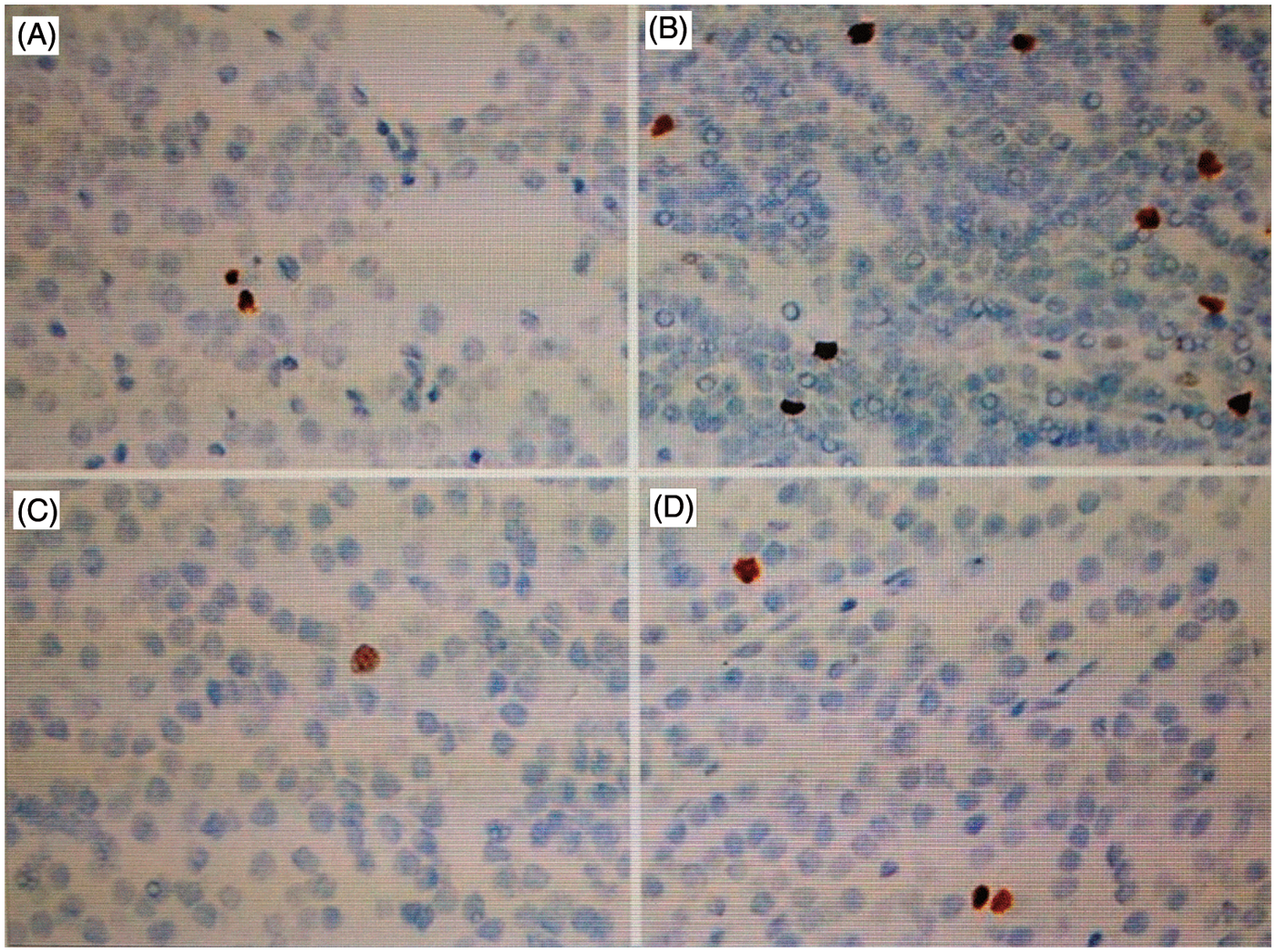
The TUNEL assay revealed distinct patterns of nuclear staining in positive and negative cells (Figure 3). The TUNEL LI for nodular hyperplasia was significantly higher than for the other specimen types (P < 0.05 for each comparison; Table 2). The LIs of Ki67 antigen in primary adenoma and nodular hyperplasia were higher than those obtained by TUNEL analysis (P < 0.001 for each comparison; Table 2).
Analysis of apoptosis using deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick end labelling (TUNEL) assay (original magnification × 100). Nuclear staining of positive cells was demonstrated by distinct black spots; negative cells had diffuse staining. (A) Normal parathyroid gland showing no apoptotic cells; (B) primary adenoma showing one positively-stained nucleus; (C) secondary hyperparathyroidism with diffuse hyperplasia showing one positively-stained nucleus; (D) secondary hyperparathyroidism with nodular hyperplasia showing several nuclei with positive staining. Sections were counterstained with methyl green.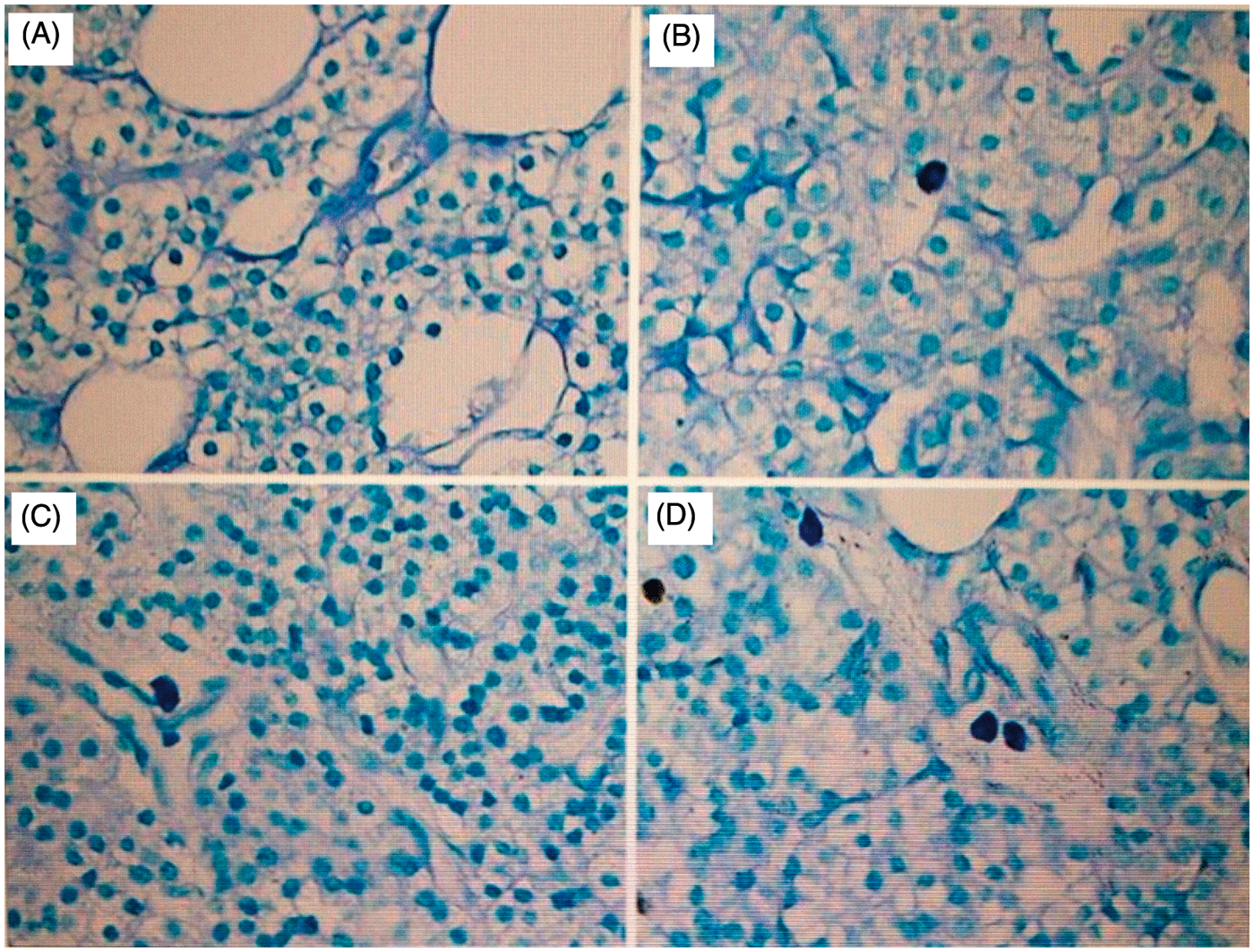
Discussion
In humans, parathyroid growth in response to chronic renal failure progresses through several stages, from diffuse hyperplasia to nodular hyperplasia and finally to the formation of adenomas. 12 Diffuse hyperplasia is initiated by hypocalcaemia and phosphorus retention, and becomes more severe as a result of calcitriol deficiency;13,14 the hyperplasia becomes nodular and the glandular enlargement becomes asymmetrical. The nodules consist of cells that are closely packed, with increased expression of proliferation markers and decreased CaSR.14,15
The present study findings demonstrated that a reduced intracellular concentration of CaSR was characteristic of nodular hyperplasia of the parathyroid glands, in patients with CKD. The amount of CaSR protein in advanced SHPT is reduced in nodular hyperplasia more markedly than in diffuse hyperplasia. 6 Nodular hyperplasia is usually present in patients with higher concentrations of serum COOH-terminal immunoreactive PTH. 16 These findings suggest that nodular hyperplasia represents an advanced stage of hyperplasia and is present in patients with more severe stages of hyperparathyroidism.
Abundant numbers of apoptotic cells were found in nodular SHPT samples in the present study. The number of apoptotic cells in SHPTs has been shown to be significantly higher than in normal parathyroid glands. 17 It has also been suggested that the rate of parathyroid cell proliferation would, theoretically, be higher than the rate of apoptosis in the areas of hyperplasia that are characteristic of SHPT. 18 For hyperplasia of the parathyroid glands to occur, the rate of proliferation must be greater than the rate of apoptosis.
Increased Ki67 antigen and TUNEL assay staining were both observed in nodular hyperplasia compared with diffuse hyperplasia, in the present study. This was consistent with previous research findings.19,20 The current findings from the TUNEL assay suggest that apoptosis in nodular hyperplasia occurs more frequently than in diffuse hyperplasia. Furthermore, the LI of the Ki67 antigen was higher than the TUNEL LI in nodular hyperplasia, suggesting a greater rate of proliferation compared with apoptosis.
Current treatment options for SHPT include modulation of calcium and phosphorus balance by dietary intake and dialysis, use of active vitamin D compounds (such as calcitriol and vitamin D analogues), phosphate binders and calcimimetics.21,22
Over the last decade, evidence has accumulated for the modulating ability of the type II calcimimetic agent, cinacalcet, for the CaSR in hyperparathyroid individuals. 23 Timmers et al. 24 suggested that cinacalcet therapy should be considered in patients with intractable hypercalcaemia. Furthermore, the addition of vitamin D to calcium may oversuppress PTH, with potentially negative consequences.25,26 Results of a randomized trial indicate that cinacalcet may favourably affect the progression of cardiovascular calcification, compared with traditional therapy using vitamin D sterols. 27
Despite medical therapy, parathyroid hyperfunction persists, eventually becoming extremely severe and requiring surgical parathyroidectomy. Reasons for the failure of receptor therapy include intrinsic factors (linked to the large volumes of the glands themselves with nodular hyperplasia), and a reduced density of vitamin D receptors and CaSR. 28 It has been reported that cinacalcet might be less effective in patients with severe SHPT who have multiple enlarged parathyroid glands and much lower levels of CaSR protein. 29
The present study provided insight into the pathogenesis of parathyroid hyperplasia and suggested that a calcimimetic compound might be refractory to patients with nodular hyperplasia in severe SHPT. In cases like this, parathyroidectomy is recommended. If patients with SHPT are resistant to calcimimetic compounds; they should undergo an evaluation of CaSR and hyperplasia by performing a fine-needle biopsy of the parathyroid glands.
In conclusion, the present study demonstrated decreased CaSR protein in nodular hyperplasia compared with normal parathyroid glands. A calcimimetic compound should be used carefully in patients with nodular hyperplasia and severe SHPT. In addition, the rate of cell proliferation appeared to be greater than the rate of apoptosis in nodular hyperplasia, which could contribute to the pathological progression of SHPT.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.