
Abstract
Empyema necessitatis is a rare complication of empyema, in which the pleural infection spreads outside of the pleural space to involve the soft tissues of the chest wall, and is difficult to diagnose with sonography alone. In the case presented, sonography to evaluate a focal anterior chest wall pain in a patient resulted in findings consistent with an abscess and prompted additional workup. Further testing included sonography-guided aspiration and computed tomography scan to establish the diagnosis followed by surgical debridement.
Keywords
Empyema necessitatis was first described by Gullan De Baillon in 1640 as an uncommon complication of empyema in which inflammation associated with an underlying pulmonary bacterial infection bridges the pleural space and involves the thoracic wall. The overall mortality rate in the preantibiotic era was 66%, with mortality rates varying from 87% in cases of Mycobacterium tuberculosis–related empyema necessitatis to 28% in cases of Streptococcus pneumoniae–related empyema necessitatis. 1 It is a life-threatening condition if not treated promptly and properly, but current treatment with antimicrobials and surgical debridement has drastically reduced mortality. We report a case in which sonography permitted a prompt diagnosis and definitive treatment of this disease.
Case Report
A man in his early 50s presented to a cardiology department with anterior upper chest wall pain, the onset of which occurred after pushing a heavy door. The pain was constant but was exacerbated while lifting or pushing objects; during the time of experiencing this exacerbated pain in the upper chest, the pain would radiate into his left arm. The patient denied any trauma to his chest or shoulder. He was suspected of having a strain in his left pectoral muscle and was started on a series of nonsteroidal anti-inflammatory medication for the pain and referred to a physical medicine and rehabilitation physician.
On physical examination, the patient had a palpable mass at the level of the first intercostal space on an anterior mid-clavicular line, with mild edema and tenderness over the left anterior chest wall. Strength testing was 4/5 strength (movement possible against some resistance by the examiner) on arm adduction; range of movement of the left shoulder was normal. The neurovascular system was intact.
Sonographic evaluation with a 12-MHz linear array transducer was performed by a physical medicine and rehabilitation physician with four years of experience in musculoskeletal (MSK) sonography. The examination showed a mixed-echogenicity collection with poorly defined margins in the first intercostal space on a mid-clavicular line, with mild edema beneath the pectoralis major and minor muscles, compromising the posterior muscular fibers (Figure 1). Graded compression was performed, revealing a swirling appearance, and a hypoechoic fluid collection was noted. Color Doppler imaging did not show any evidence of increased flow at the periphery or within the abscess. Sonography-guided aspiration was performed, which resulted in a positive bacterial culture for Staphylococcus epidermidis.
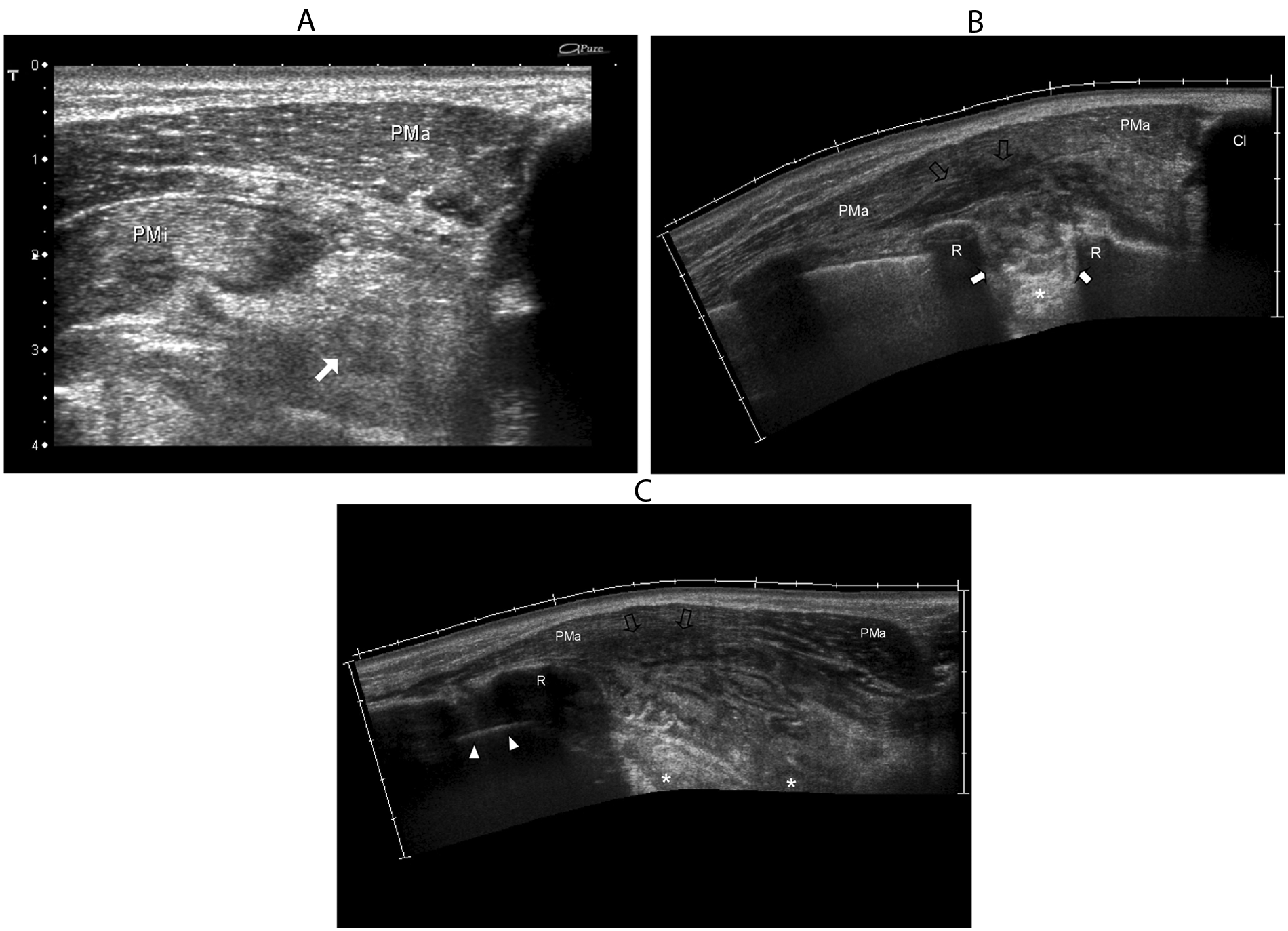
Sonographic appearance of the left anterior chest wall. (A) Mixed-echogenicity fluid collection (white arrow) beneath the pectoralis major muscle (PMa) and the pectoralis minor muscle (PMi). Panels B (sagittal) and C (axial) present extended field-of-view images of the abscess that show its location in the first intercostal space at the left anterior chest wall. There is a mixed echogenicity within the abscess (white arrows) and an area of edema (void arrows) within the posterior fibers of the PMa. Panel C shows an irregular fluid-filled hypoechoic area with posterior acoustic enhancement containing a variable amount of echogenic debris or pus (asterisk) indicating compromise of the pleural space. Arrowheads: pleura. Cl, clavicle; R, rib.
A computed tomography (CT) scan was performed to establish the exact margins of the abscess. The CT showed that between the first and second left rib, an oval mass of obtuse angles was present with homogeneous density (80 Hounsfield units) and well-shaped margins, consistent with an empyema (Figure 2). The patient underwent surgical exploration eight days after his first consultation, which confirmed the sonographic and CT imaging findings. A complete debridement of the abscess was done, with a surgical drain placed for a pleural effusion. The patient antibiotic regimen was begun prior to surgery and continued to completion during the postoperative period. On clinical follow-up two months after surgery, the patient was asymptomatic and had full range of motion in the left upper extremity with normal strength and no respiratory difficulty or fever.
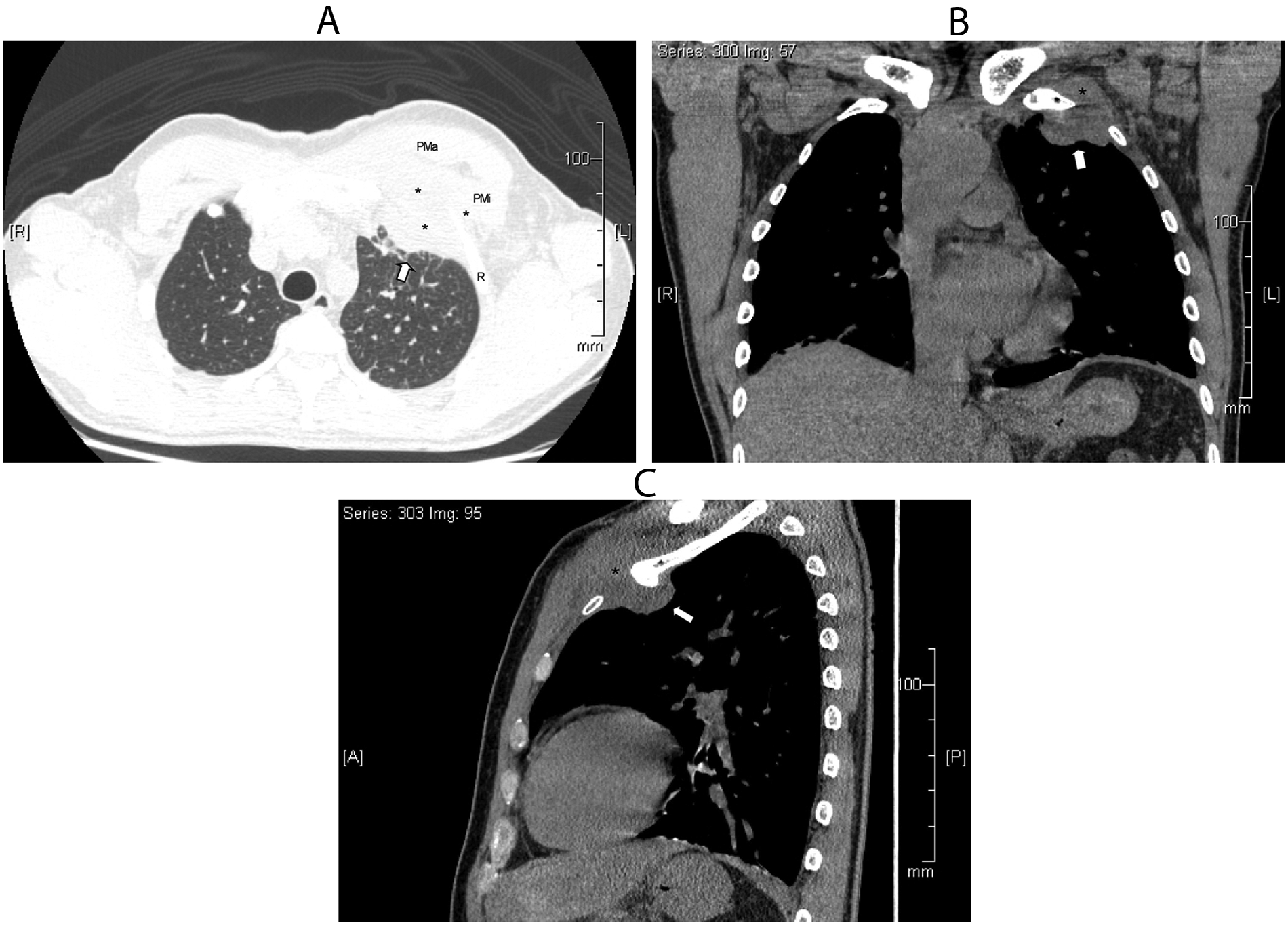
Nonenhanced computed tomography (CT) scan of the chest. (A) Cross-sectional CT image showing the empyema necessitatis (arrow), a bacterial lesion that extends from the left upper lobe of the lung into the extrathoracic soft tissues beneath the left upper pectoralis muscle (asterisks). Panels B (coronal) and C (sagittal) show compromise of the pleural space and extrathoracic tissue. PMa, pectoralis major; PMi, pectoralis minor.
Discussion
Empyema necessitatis is rare, and in this case, it was also caused by an unusual pathogen for this entity, S epidermidis. Empyema necessitatis may be asymptomatic, but it is important to note that it can present with mild chest pain and a nonproductive cough. The most common location is the anterior chest wall between the mid-clavicular and anterior axillary lines. 2 It is an uncommon complication of empyema in which inflammation associated with an underlying pulmonary bacterial infection bridges the pleural space and involves the thoracic wall. Ultrasonographic evaluation identified the extrathoracic manifestation of the primary lesion in this case and permitted sonography-guided puncture and culture of the collection. In addition to using sonography, a CT scan demonstrated a pleural effusion connected to the chest wall mass, which is pathognomonic for empyema necessitatis. 3
Because of its unusual symptomatic presentation, the patient initially underwent a cardiologic evaluation and eventually was referred to a physical medicine and rehabilitation physician with a suspected strain of his pectoral muscle. At that juncture, the utilization of high-resolution sonography helped to assess the separated muscular components, myotendinous junction, and enthesis of the muscles accurately. Sonographically, an abscess may have many different presentations depending on the interaction of the sound beam with the tissues beneath the transducer. Infected fluid collections can appear anechoic, hypoechoic, or hyperechoic or be of mixed echogenicity. When hyperechoic internal echoes are seen, they are typically secondary to gas bubbles or aggregates of fibrin and white blood cells. Fluid-filled levels can be noted within the collection with dependent layering of the more echogenic particulate material. In highly echogenic collections, a slight pressure with the probe or the examiner’s fingers may help to confirm the liquid nature of the mass by causing fluctuation and movement of the particles. Also with an abscess, the margins can be well circumscribed or poorly defined and present with a thickened hyperechoic rim. Power Doppler imaging may be helpful in distinguishing these from hematomas. 4 Color Doppler imaging will show increased flow in the inflammatory region at the periphery of the abscess, with absent flow within the fluid collection. A definitive diagnosis is only possible with fluid aspiration. 5 If the abscess lies in proximity to the bone, sonography may reveal the osseous origin of the infection by depicting hypoechoic subperiosteal fluid. 6
Sonography in conjunction with a CT scan often provides the best outcomes for a patient with a possible empyema. The typical empyema is lenticular, and it appears as a fluid density collection in the pleural space, sometimes with loculations in the fissures or gas bubbles in the pleural space, all of which strongly suggest an empyema in the proper clinical context. Typically, they form obtuse angles with the adjacent lung, which is displaced and compressed. The pleura itself may be thickened due to fibrin deposition and in-growth of vessels. In this case, confirmation of a soft tissue abscess was made by sonography-guided puncture and culture.
The majority of reported empyema necessitatis cases are caused by M tuberculosis, but Actinomyces species have replaced S pneumoniae as the second most common cause. Less common etiologic agents include Staphylococcus aureus, Streptococcus milleri, Fusobacterium nucleatum, Mycobacterium avium, Mycobacterium intracellulare, Burkholderia cepacia, and Blastomyces spp.1,3,5 No previous report had been found in the literature of S epidermidis as an etiologic agent. Staphylococcus epidermidis, a gram-positive and coagulase-negative staphylococci, 1 lives typically on the human skin and mucosa, the most common cause of infections on catheters and implants. 2 It is one of the five most common organisms that cause nosocomial infections due to the increase in usage of biomaterials in the clinical environment (prosthetic valves, cerebrospinal fluid shunts, joint prosthesis, vascular prostheses, pacemakers, etc).3,7
Conclusion
Empyema necessitatis should be considered if a patient presents with a palpable chest mass with edema. It is important to take a patient history to document any unusual signs and symptoms that may be of clinical significance. This report describes a case of left anterior chest pain due to an empyema necessitatis with the unusual underlying etiologic agent S epidermidis. High-resolution sonography was able to investigate the chest mass thoroughly, which facilitated an accurate preoperative diagnosis and aided in the appropriate management for the patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.