
Abstract
Uterine arteriovenous malformation and arteriovenous fistula are rare vascular lesions that have only recently been described in literature. They are two differentials in reproductive-age women with acute onset of abnormal vaginal bleeding. The sonographic and clinical presentation of these two pathologies can be both varied in appearance and impossible to distinguish from each other. However, a detailed history along with specific sonographic investigation using color and pulse-wave Doppler, as well as a transvaginal scanning technique, can lead to strong suspicion of these vascular malformities. A successful sonogram can provide essential evidence to justify further investigation with a more invasive angiography procedure. This will not only confirm a diagnosis but also give important information regarding the size and exact location of the lesion. These facts will help the interventional radiologist and treating physician decide if different types of embolization are possible or if hysterectomy is necessary.
In the investigation of abnormal vaginal bleeding in nongravid patients, sonography is routinely requested. Although a thorough history and review of symptoms are paramount to accurate diagnosis, a meticulous sonographic interrogation of the uterus is equally important. The sonographer’s systematic transvaginal examination, complete with Doppler and gray-scale analysis of the uterus, can provide a probable diagnosis noninvasively and quickly in patients with pelvic vascular abnormalities. This information can prevent unnecessary tests as well as continued significant blood loss. The attending physician also has a foundation for deciding on the medical plan for monitoring or treating the patient. Specifically, the following cases demonstrate the potential of the pelvic sonogram to reveal abnormal communications between the vascular networks of the uterus such as arteriovenous fistulas (AVFs) or arteriovenous malformations (AVMs).
Case 1
A nongravid Hispanic female presented to the emergency room with acute onset of profuse vaginal bleeding with passage of large clots for six hours. Her last menstrual period had been less than two weeks prior. She was found to have severe anemia with diminished blood pressure, and her history was negative for any type of surgery, instrumentation, trauma, or bleeding disorder. A pelvic sonogram was ordered to assess the etiology of the bleeding.
With a GE-Logiq 9 (General Electric Medical Systems, Wauwatosa, Wisconsin), the transabdominal sonogram was completed using a curved 2- to 5-MHz transducer. The first sonographic finding was a slightly enlarged uterus at 4.1 × 12.2 × 6.2 cm. A more detailed view of the uterus and ovaries was then attained using an endovaginal 4- to 10-MHz transducer, revealing complex fluid in the endometrium (Figure 1). When color Doppler was applied to this fluid, a Y-shaped vascular lesion with hyperperfusion and a mosaic pattern was discovered. It was located in the posterior uterine myometrium at the uterine fundus, extending from the endometrium to just superficial to the serosal surface (Figure 2). This lesion was undetectable by gray-scale imaging. Pulse-wave Doppler demonstrated increased velocities, with the highest measured at 113 cm/s. The velocity in the feeder vessel measured 27.8 cm/s. These waveforms demonstrated low-resistance, stenotic flow patterns with blending of arterial and venous waveforms (Figure 3).
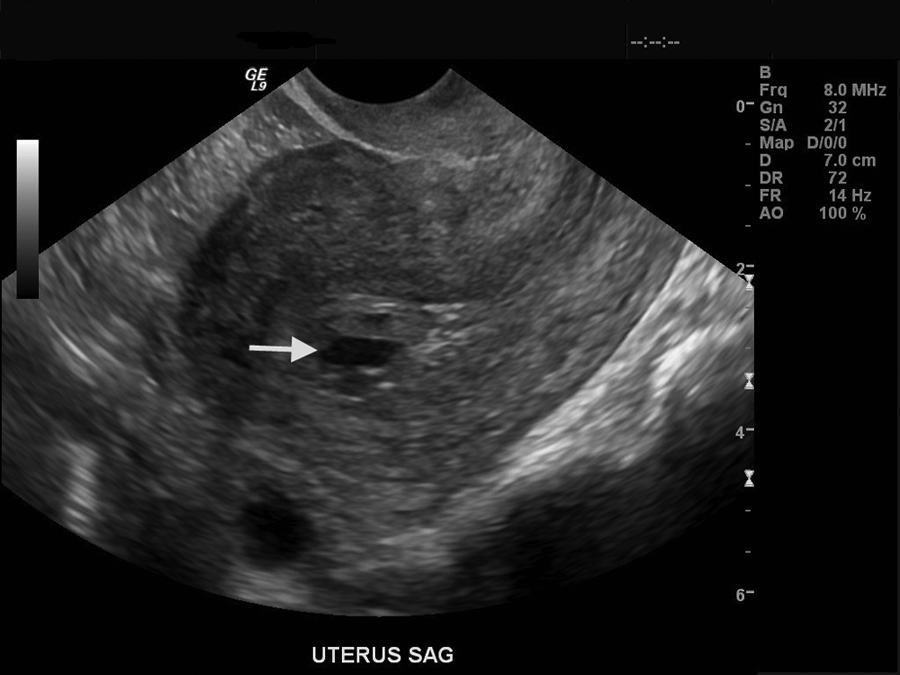
Transvaginal image of a uterus with a complex fluid-debris level (white arrow) in the endometrial canal.
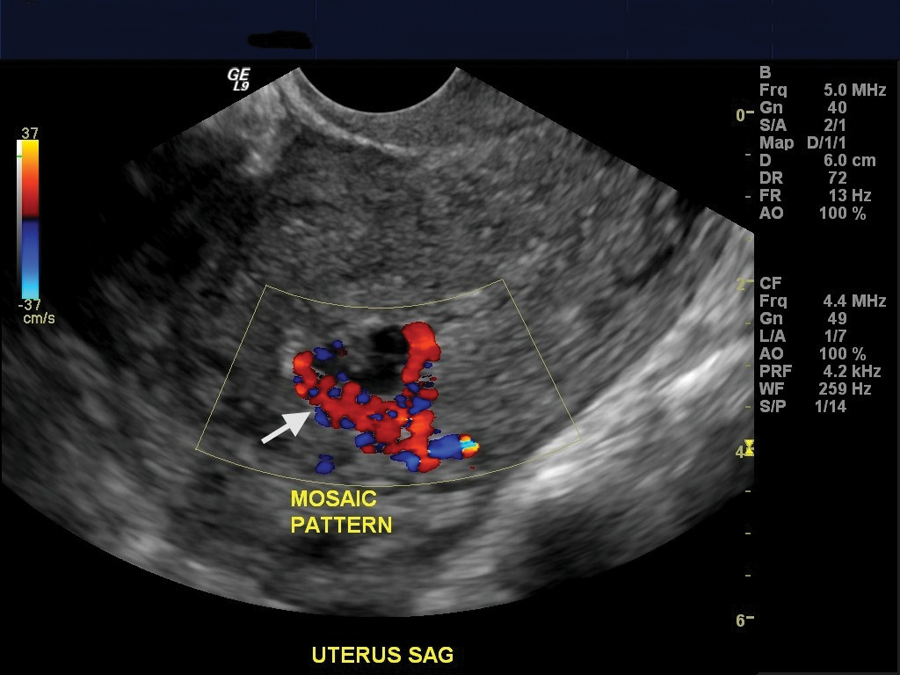
Transvaginal image of a uterus with color Doppler demonstrating color mosaic pattern (white arrow) of perfusion.
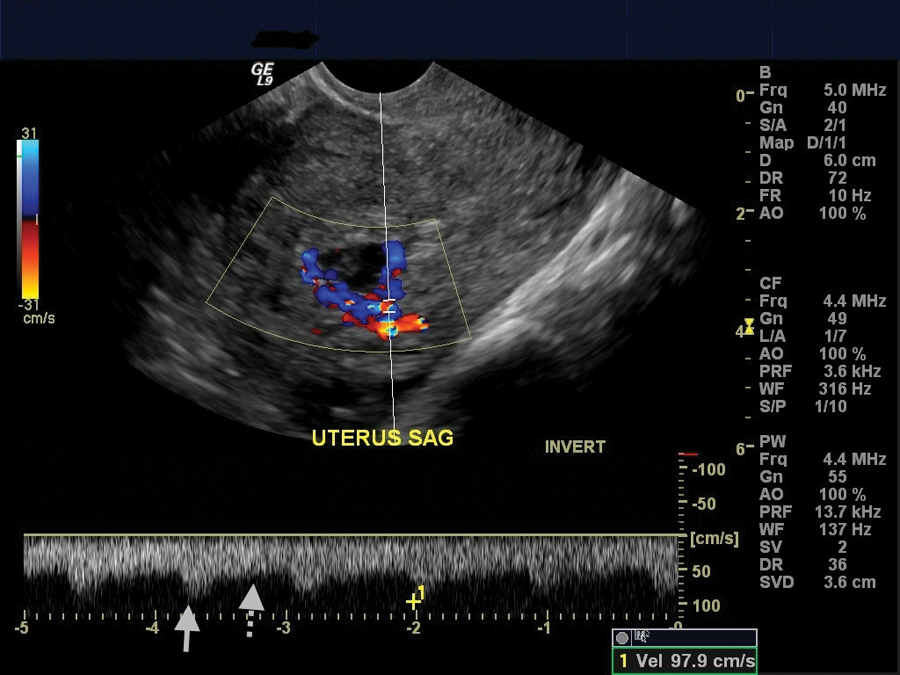
Transvaginal image of a uterus using color Doppler and pulse-wave Doppler to demonstrate a high-velocity (white arrow), low-resistance (dotted white arrow) waveform.
Subsequent to the abnormal sonogram, a pelvic arteriogram including the internal iliac and uterine arteries bilaterally was performed. These tests positively diagnosed a left uterine artery AVM (Figure 4). Because of the patient’s desire to preserve fertility, a bilateral uterine artery embolization was performed. Gelfoam slurry was used as the embolic agent until stasis of blood flow was achieved. The patient was discharged and has had no recurrence of abnormal vaginal bleeding.
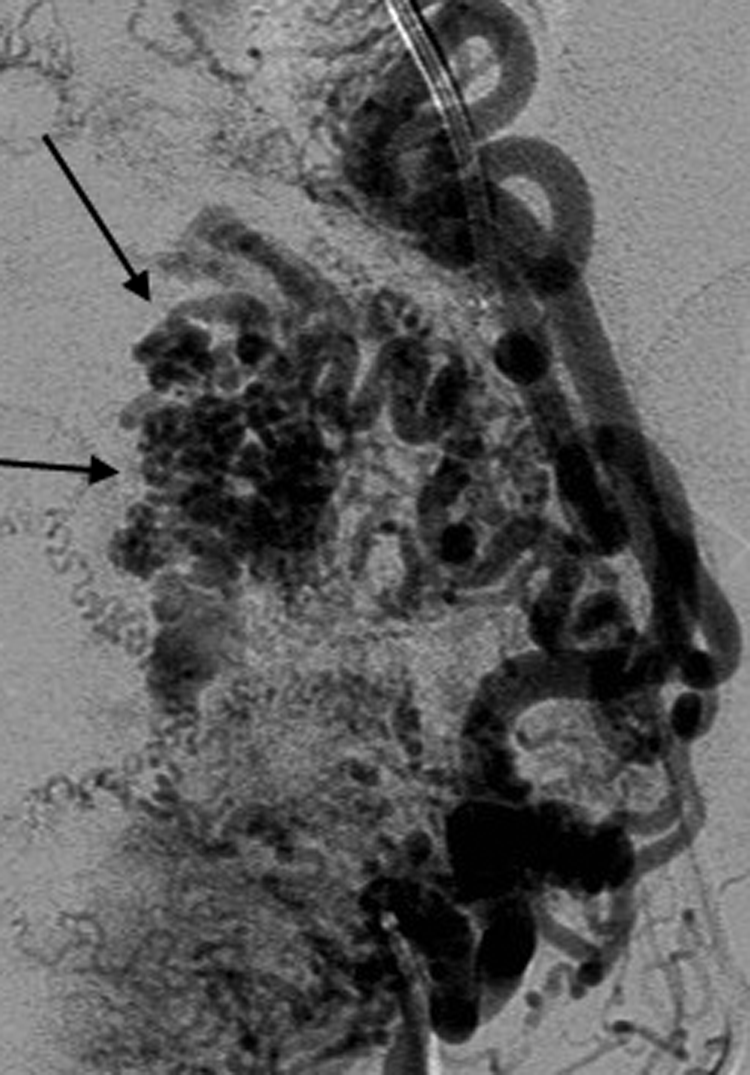
Pelvic angiogram demonstrating central nidus (black arrows) or jumble of vessels.
Case 2
A nongravid African American female presented to the emergency room with vaginal bleeding and passage of large blood clots for seven days, progressively increasing in volume. Her history was significant for an elective abortion with a dilation and curettage 70 days prior. Because of the patient’s anemia, two units of blood were transfused. In an effort to noninvasively treat uterine bleeding, she also received intravenous conjugated estrogen. A pelvic sonogram was ordered to evaluate for any etiologies that might be contributing to the patient’s clinical status. Using a Philips iU22 (Philips Healthcare Systems, Bothell, Washington), the transabdominal portion of the examination was completed using a curved 2- to 5-MHz transducer. To further characterize the uterus, an endovaginal 3- to 10-MHz transducer was employed. The sonographic findings demonstrated a normal-sized uterus with a complex fluid-debris level in the endometrial canal (Figure 5). Color Doppler was employed to further investigate this fluid, and a hypervascular, isoechoic lesion was discovered in the posterior uterine fundus extending from the endometrium to the deep myometrium (Figure 6). Pulse-wave Doppler was used to measure the increased velocities, with the highest measured velocity of 89 cm/s. Similar to the first case, the Doppler characteristics were a color mosaic pattern with high-velocity, low-resistance flow and loss of differentiation between arterial and venous waveforms (Figure 7). 1

Transvaginal image of uterus with a complex fluid-debris level (white arrows) in the endometrial canal.
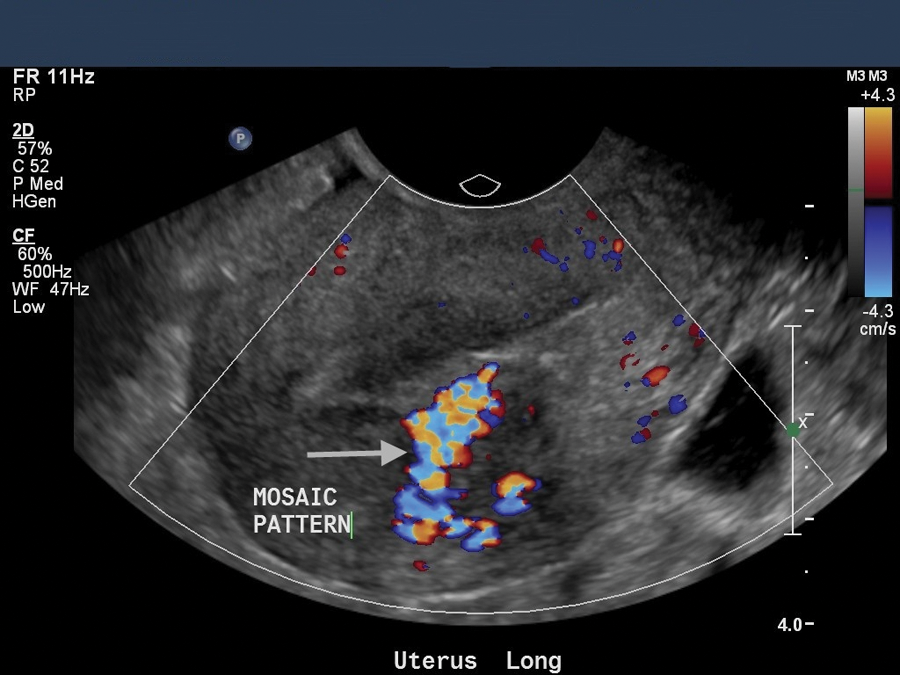
Transvaginal image of uterus with color Doppler demonstrating a color mosaic pattern (white arrow) of perfusion.
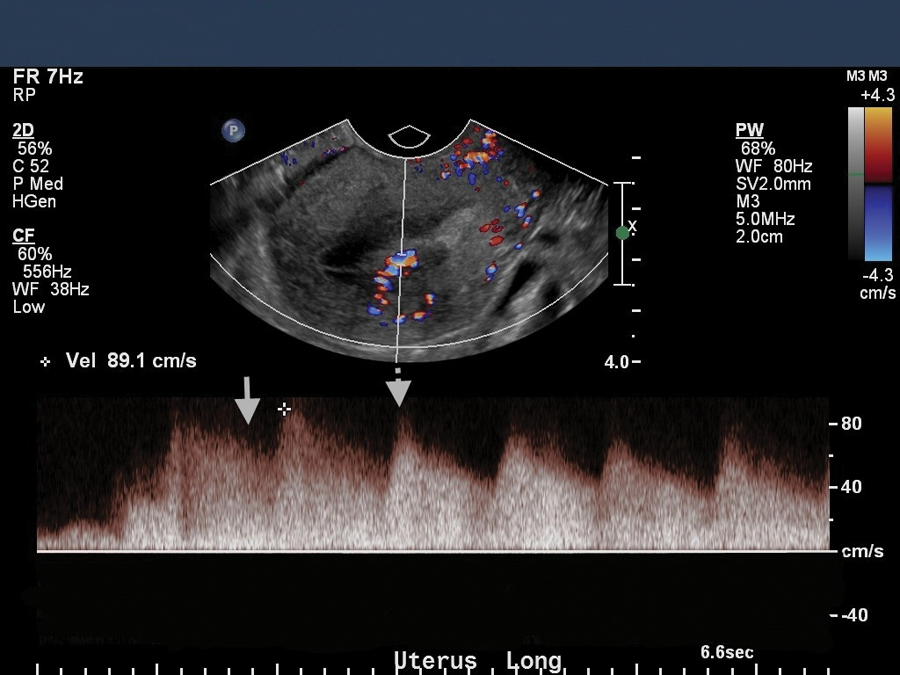
Transvaginal image of uterus using pulse-wave Doppler demonstrating high velocity (cursor), low resistance (white arrow), and loss of arterial or venous waveform differentiation (dotted white arrow).
The following day, when the hormone therapy failed to diminish or stop the vaginal bleeding, a pelvic arteriogram including the iliac and uterine arteries bilaterally was performed, resulting in a positive diagnosis of left uterine artery arterial AVF with an associated pseudoaneurysm (Figure 8). An embolization was requested so that surgical treatment could be avoided. Because of the distal location of the AVF, a microcatheter was unable to be advanced to the lesion and a microcoil embolization was not possible. Instead, embolization was performed bilaterally with gelfoam slurry. The patient was discharged and has had no recurrence of abnormal vaginal bleeding.
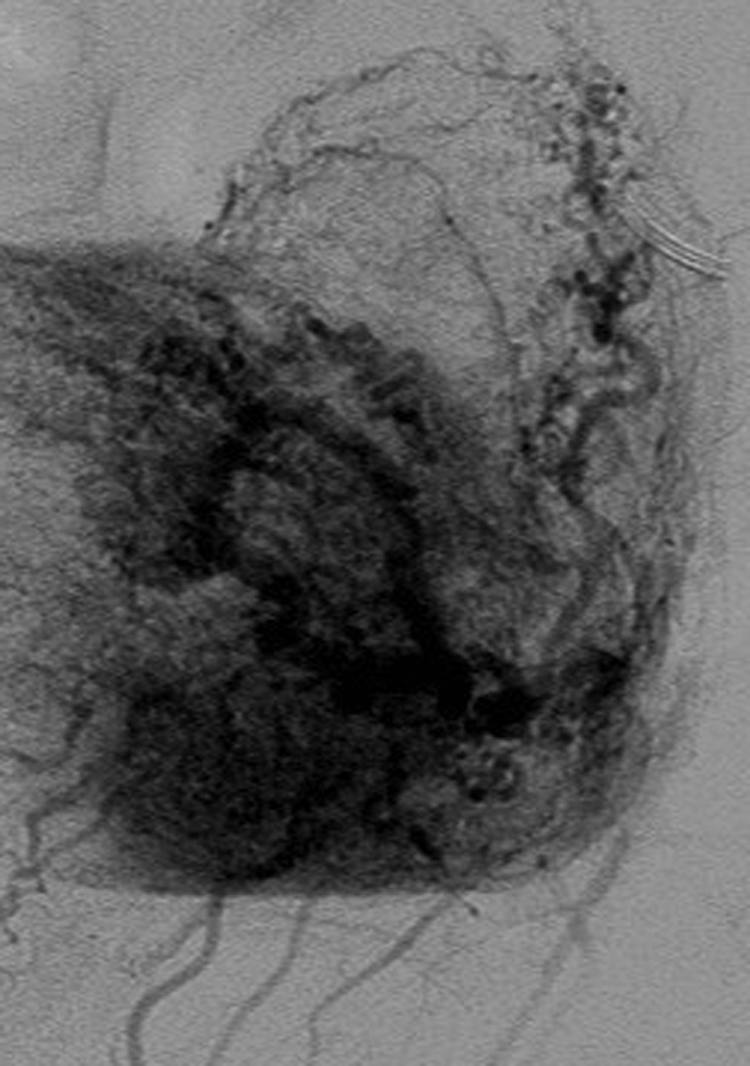
Pelvic angiogram without a characteristic central nidus.
Discussion
In the circulatory system, the vessel sequence for blood flow from the arterial system to the venous system is normally artery to arteriole to capillary to venule to vein. This allows for the dissipation of high arterial pressures, as well as providing the physiologic platform for the exchange of oxygen and nutrients across capillary networks. AVFs and AVMs circumvent this coordinated exchange by allowing direct connections between the larger arteries and veins. This forces flow from a high-pressure system directly into a low-pressure system without the benefit of intermediaries. These vascular anomalies can be asymptomatic based on where the vascular abnormality occurs or can cause increased cardiac output complications or even high-pressure hemorrhage. 2 The common symptoms of both uterine AVFs and AVMs are excessive vaginal bleeding, dyspareunia, pain, audible bruit, pulsatile mass on clinical vaginal examination, and excretory dysfunction of the digestive and urinary systems. 3 The most important part of attaining the history in these patients is to ascertain without doubt whether there has been any surgery, instrumentation applied, or trauma by asking questions using specific examples.
In addition to being similar clinically, sonographically the findings are nearly identical with demonstration of high-velocity, low-resistance blood flow in a swirling or mosaic pattern. Reported studies indicate that for AVMs and AVFs, the resistive indices range from 0.25 to 0.55, and the velocities range from 40 to 100 cm/s. 4 Other reported characteristics are the sonographic appearance of hypoechoic lesions or serpiginous anechoic areas that fill in with color Doppler. The appearance is a result of the size and location of the vessels affected. 2 In many cases, without the use of color or pulse-wave Doppler, the lesion is undetectable, and the evaluation of flow velocity and characteristics is impossible. According to the American College of Radiology uterine assessment guidelines, 5 these tools can be useful in detecting vascular uterine lesions based on studies done by numerous outside sources.2,6–8 This guideline, as well as the use of transvaginal sonogram, is part of the pelvic sonogram protocol at the institution where these case studies occurred.
Although the symptoms and sonographic presentation of these vascular anomalies in the uterus can be identical, the etiologies are different and discrete. Uterine AVM, such as the one diagnosed in the first case, is a rare, mostly congenital vascular malformity characterized by a lesion in which there are multiple abnormal connections or shunts between arteries and veins. These form embryologically when there is atypical differentiation of the capillary plexus. This causes an abnormal area of perfusion, which typically has multiple feeding vessels and a central nidus, or tangle-like web of inappropriate vascular connections. 1 This hallmark appearance is documented by angiography as a region of radio-opaque contrast “blush” (corresponding to the region of mosaic-pattern filling seen by color Doppler imaging; Figure 2). These connections are usually present throughout the entirety of the patient’s life, but they may become pathologic in response to a change in hormones or following trauma. 9 As a major change in patient hormone level occurs during pregnancy, the growth of these vascular malformations during pregnancy can cause an increased risk for hemorrhage; however, they rarely have been diagnosed in gravid patients. This is thought to be a result of an abnormal uterine environment reducing the possibility of normal embryonic implantation in early pregnancy. 10 The true incidence of this malformity is unknown, with the first reported case in 1926 by Dubreuil and Loubat. 11
Uterine AVF, as seen in the second case, is also a vascular lesion found mostly in women of reproductive age with abnormal vaginal bleeding. It is not congenital but environmental in etiology. The defect is typically caused by trauma; uterine inflammation resulting from infection or endometriosis; a uterine intervention such as surgery, dilation and curettage, or cesarean delivery; a malignancy such as carcinoma of the cervix or endometrium or trophoblastic disease; or fibromas. 1 Although AVMs have multiple feeder vessels, an AVF typically only has a single abnormal connection providing direct communication between an artery and a vein, but because of their low vascular resistance, they can be supplied by both uterine arteries. The distinguishing central nidus or jumble of vessels is therefore not identified on angiography.4,12
Angiography is not only the gold standard for a definitive diagnosis but is also used to guide the treatment of both conditions. 4 Traditionally, treatment for vascular anomalies of the uterus was hysterectomy, at which time diagnosis was confirmed. With advances in interventional radiology and increased understanding of these pathologies, embolization is now the standard treatment in a patient who wishes to sustain fertility. This is a procedure where a substance or a coil is used to produce a clot, which effectively closes off a defective vessel. Ethanol and glue, as well as microcoils, are an example of permanent methods for embolization. Gelfoam is a type of pliable sponge, which serves as a temporary clotting agent. The decision of which embolytic agent and method to use is based on the location or accessibility of the anomaly and the relative size of the vessel(s) involved. Complications include tertiary tissue damage and emboli dislodgement, collateral formation, or recanalization, requiring a repeated procedure or hysterectomy. 9 Advancements in the diagnosis and treatment of uterine AVFs and AVMs have provided these patients and their treating physicians with more varied and less invasive options.
Conclusion
Although their sonographic appearance and clinical symptoms are similar, AVF and AVM of the uterus have unique and specific etiologies. A detailed history can help to discern between the two, and pelvic angiography will provide the final diagnosis. Because these pathologies can be occult if color and pulse-wave Doppler are not employed, the sonographer should always use these capabilities. The omission of these tools in sonographic evaluation of abnormal vaginal bleeding can be irresponsible in these potentially life-threatening pathologies. Present medical trends predict the field of sonography becoming more relied upon in the future to replace diagnostics previously achieved with more expensive or invasive modalities or modalities that expose patients to radiation. As a consequence, the ability of the sonographer to provide useful information to the interpreting and treating physicians is paramount. This is especially true in the realm of vascular anomalies, where the sonographer has the opportunity to assess blood flow in real time. The continued development and expansion of pelvic sonogram protocols will help to promote the reputation of sonography as a valid approach to investigate emergent pathologies. Such changes will result in better quality patient care while helping to reduce the cost to the health care system.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.