
Abstract
Iatrogenic endometrial arterial injury is a rare and life-threatening condition that can occur after dilation and curettage (D&C) procedures. A case is presented that describes the sonographic features of an iatrogenic endometrial arterial injury status post-D&C. The patient presented to the emergency department on several occasions for post-D&C complaints. The patient was imaged with transabdominal and transvaginal grayscale and Doppler (color and spectral) sonography on all visits. Other diagnostic testing, such as beta human chorionic gonadotropin (B-hCG) levels, also was performed. The report dictated by the radiologists considered multiple differential diagnoses, with the findings showed by sonography suggesting that the diagnosis was most consistent with an arteriovenous fistula. A follow-up sonogram at 3 months demonstrated resolution of this condition, which was present in the first 2 emergency department visits.
Keywords
Duplex sonography is an essential diagnostic tool in obstetrics and gynecology. Sonographic appearance of the endometrium following dilation and curettage (D&C) may indicate a variety of pathological conditions.1–4 However, with the use of duplex sonography, arterial injuries following this type of procedure can be identified with accuracy by a skilled sonographer. A case is presented of a 20-year-old female with a history of a recent D&C less than 1 month prior who presented to the emergency department (ED) with uterine cramping and a foul vaginal discharge. The uterus was evaluated using transabdominal and transvaginal sonography, the reading physicians’ impressions listed multiple differential diagnoses as discussed below, and the important role of sonography in reaching the proper conclusion is discussed.
Case Study
A 20-year-old female, gravida 1 para 1, presented to the ED with pelvic cramping, dysuria, and a foul vaginal discharge. The patient reported a history consistent with an incompetent cervix. Her recent history indicated she was status post–vaginal delivery of a 22-week twin gestation 22 days prior to this examination. The patient stated that the pregnancy began as triplets, but 1 fetus was lost early in the pregnancy. The pregnancy was otherwise uncomplicated until she had a painless cervical dilation. A cerclage was attempted, however, the patient experienced premature rupture of membranes (PROM) and subsequently delivered live born twins that then demised. The patient then underwent a D&C for retained products of conception (RPOC) 2 days later. Since then, the patient was seen in the ED for a urinary tract infection (UTI) and treated with Bactrim. The laboratory test results demonstrated a beta human chorionic gonadotropin (beta-hCG) of 15 without an increase in white blood cell (WBC) count.
The medical staff ordered transabdominal and transvaginal sonography to rule out RPOC. The examinations were done using a Siemens Sequoia 512 ultrasound machine (Siemens Healthcare, Malvern, PA) with a 4V1 Vector 4MHz transducer for the transabdominal portion and an EV-8C4 8MHz endocavitary transducer for transvaginal imaging.
In her first visit pertaining to this case, the sonographic findings demonstrated a heterogeneous, thickened endometrium measuring 1.6 cm with abnormal hypervascularity (Figure 1). The patient was discharged from the ED and returned 4 days later with persisting symptoms. Repeat transabdominal and transvaginal sonography was done, which again showed a heterogeneous, thickened endometrium with abnormal hypervascularity. In the second examination the endometrium measured up to 2.3 cm, with free fluid seen in the cul-de-sac (Figure 2). The thickened endometrium shown in Figure 2 is nonspecific and can represent several differential diagnoses including gestational trophoblastic disease (which was ruled out based on beta-hCG testing) and retained products of conception. Utilization of color and spectral Doppler testing showed focal areas of turbulent hypervascularity with spectral broadening, characteristic of an arteriovenous fistula (Figures 3 and 4). The patient returned to the ED 3 months later with a chief complaint of pelvic pain. On sonographic evaluation the uterus, endometrium, and adnexa were all within normal limits, without evidence of free fluid or hemodynamic abnormalities. The patient reported no change in medical history since the prior ED visit.
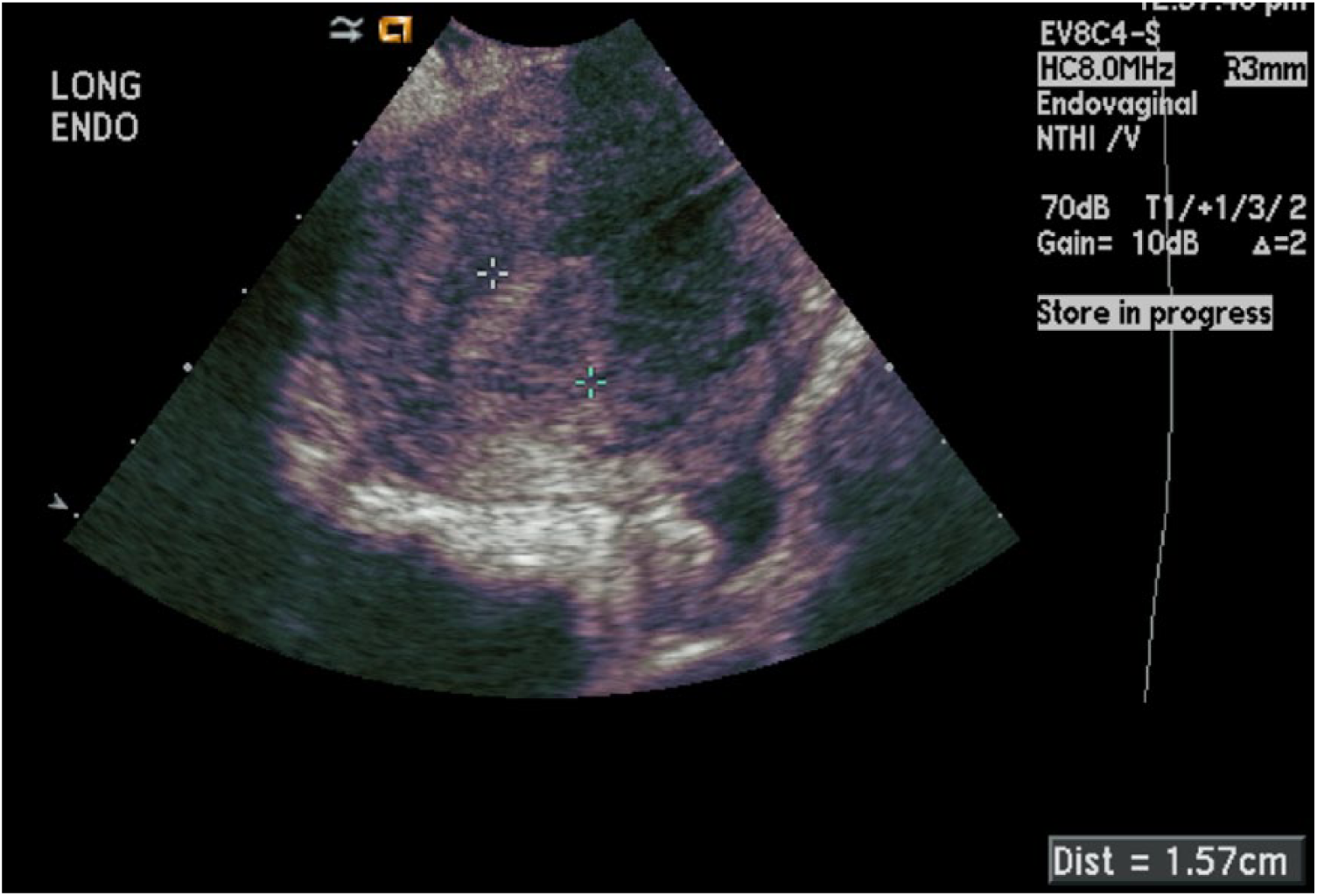
Longitudinal transvaginal grayscale image of the endometrium taken during the patient’s first visit to the emergency department approximately 3 weeks following dilation and curettage showing a heterogeneous, thickened endometrium measuring 1.6 cm.
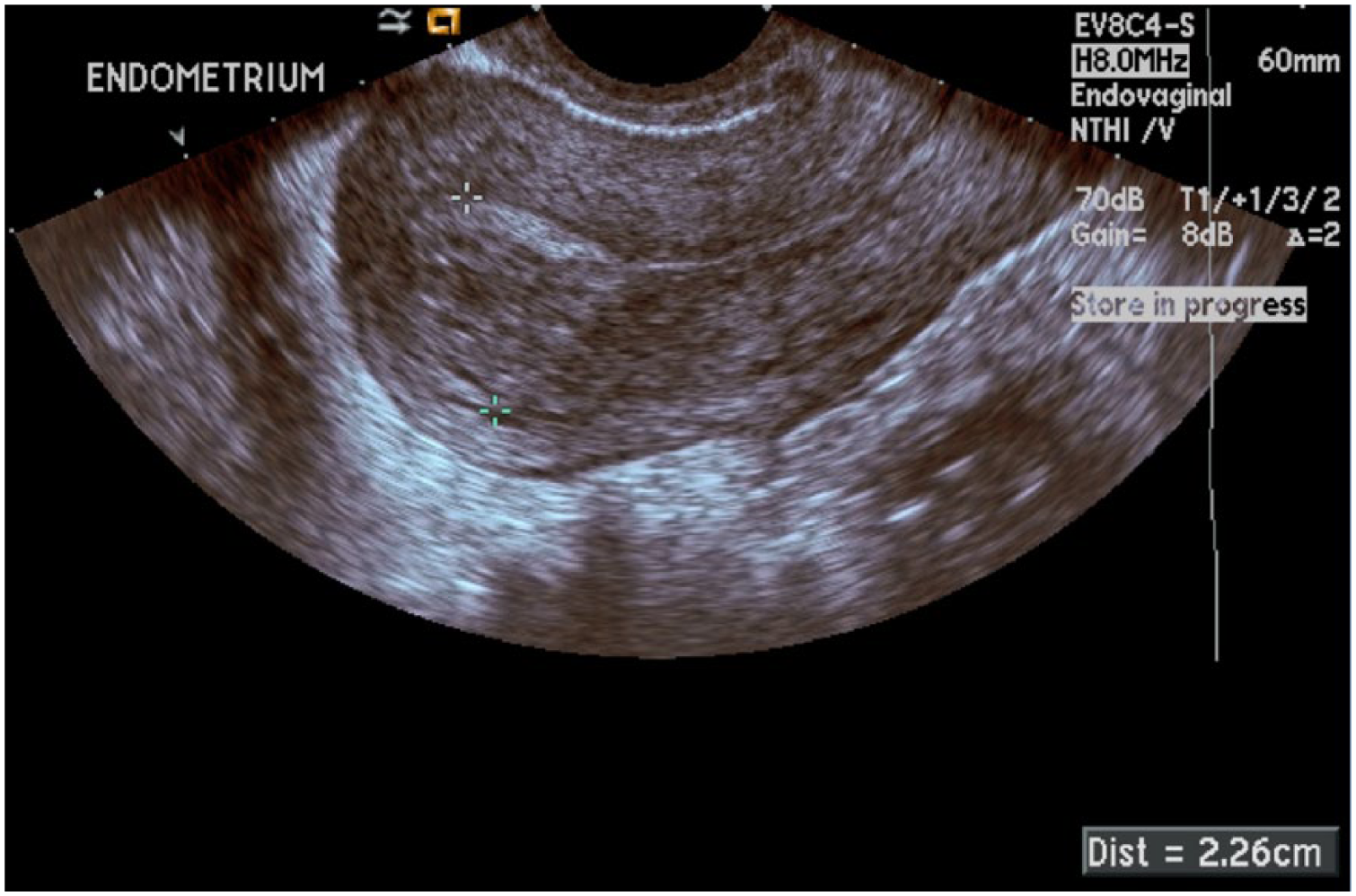
Sagittal transvaginal grayscale image of the endometrium taken during the patient’s second visit to the emergency department 4 days following the visit shown in Figure 1, again showing a heterogeneous, thickened endometrium now measuring 2.3 cm.
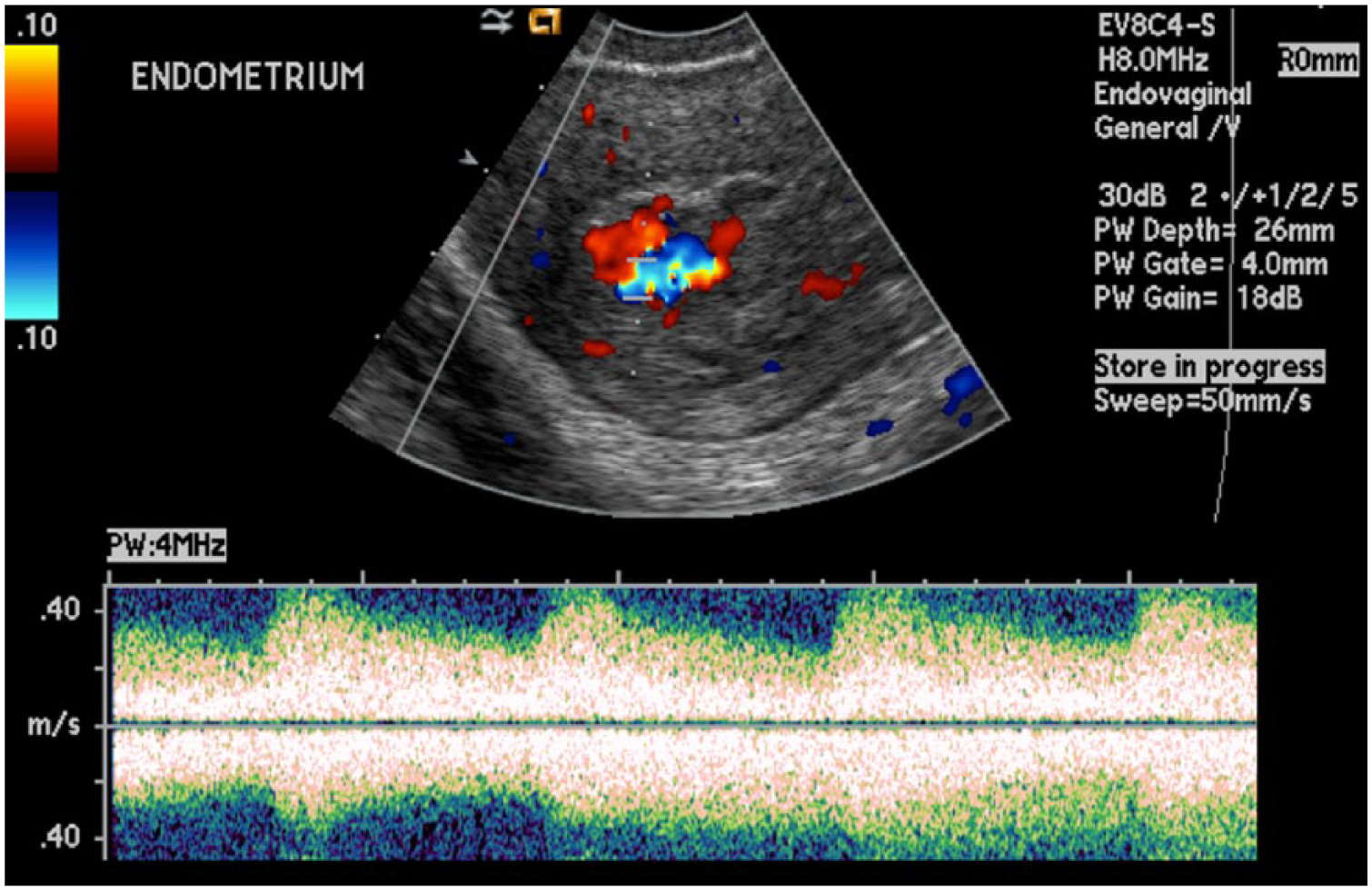
Color and spectral Doppler image of the endometrium taken during the patient’s second visit to the emergency department showing very hyperdynamic flows with very low vascular resistance, significant flow turbulence, and a broad spectral envelope indicating possible iatrogenic endometrial injury with an arteriovenous fistula.
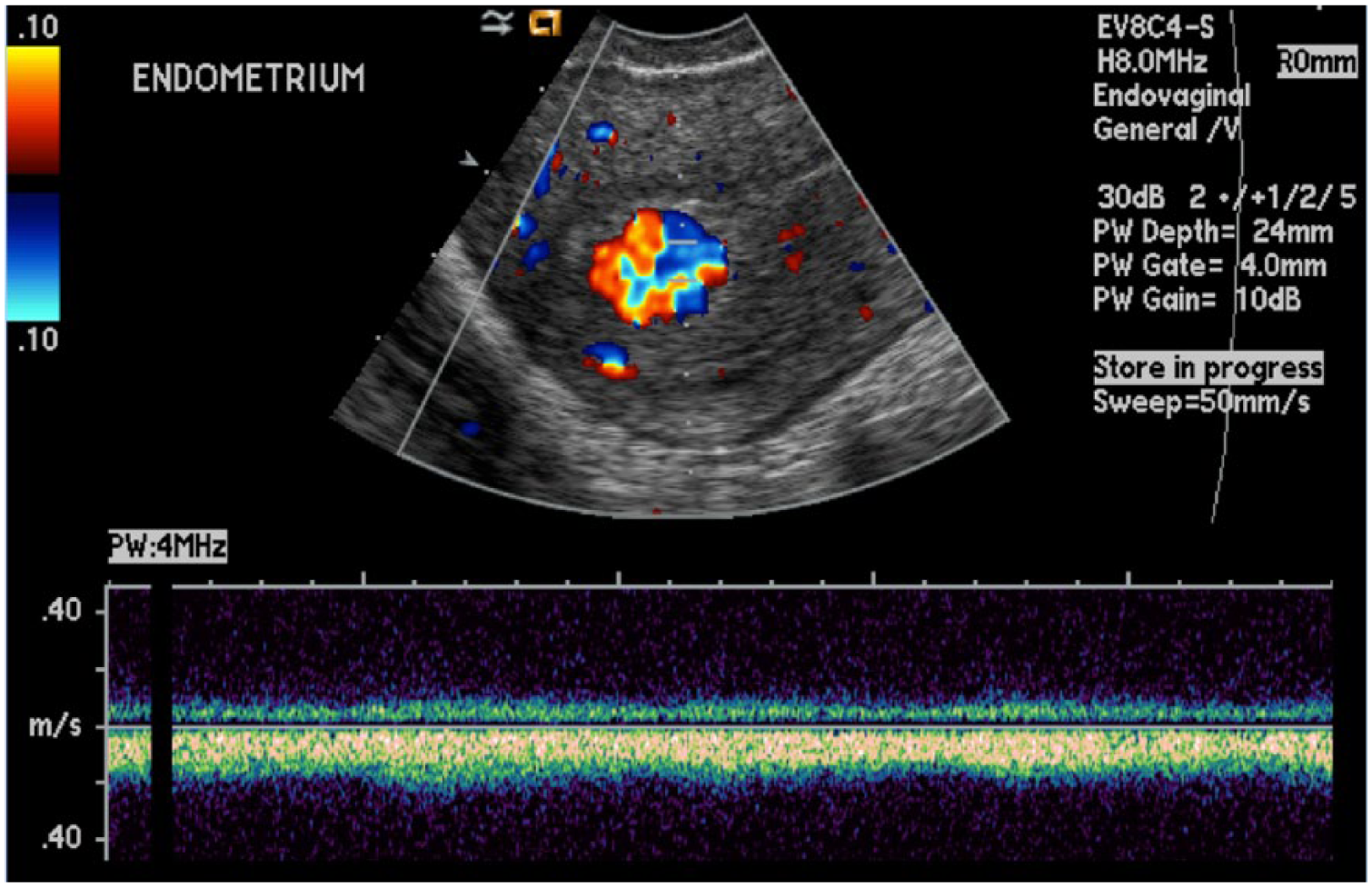
Color and spectral Doppler image of the endometrium taken during the patient’s second visit to the emergency department showing a strong hyperemic venous flow waveform in the same general area as the image shown in Figure 3.
Discussion
Iatrogenic vascular injury, often following D&C is a rare, but potentially life-threatening condition. Because of its symptoms and appearance on certain imaging modalities, it can easily be confused with other conditions. Grayscale sonography can detect the presence of multiple tubular or spongy hypoechoic areas within the endometrium. These can represent retained products of conception (RPOC), hemangioma, or gestational trophoblastic disease (GTD). 5 Therefore, using color and spectral Doppler evaluation is important for obtaining the most accurate information. A thick, hypervascular, heterogeneous appearing endometrium with measurements beyond normal limits (7–16 mm during the secretory phase) may lead to several differential diagnoses including infection, RPOC, pseudo-aneurysm, or a possible arteriovenous fistula created by the mechanisms of D&C.1–4
In the past, iatrogenic vascular injuries related to the endometrial canal following procedures such as D&C were sometimes overlooked. 1 With the use of duplex sonography, arterial injuries following this type of procedure can be identified with relative ease by a skilled sonographer, and can be treated by interventionists with transcatheter arterial embolization if necessary.1,3,6 It should be noted that arterial iatrogenic injuries such as an arteriovenous fistula are different from arteriovenous malformations (AVM).7,8 These AVMs result from an anomaly in the embryonic development, are relatively rare in occurrence, and are congenital rather than traumatic. 3 Since there can be similarities in the sonographic appearance of these 2 different conditions, it is important for sonographers, as well as health care practitioners, to acquire a detailed patient history prior to the sonographic examination.1,3,8
Pelvic pain, fever and vaginal bleeding post-D&C may also indicate RPOC. 4 The basis for a diagnosis of RPOC also relies on the components of the echogenic material found within the uterus on sonographic evaluation. Following this diagnosis, the treatment is often a follow-up with curettage to empty the contents of the endometrial cavity.
In the case presented above the beta-hCG levels were low, which would effectively rule out GTD. This patient had what appeared to be a thickened endometrium via grayscale sonography, which could have indicated RPOC. However, on utilization of color Doppler imaging, an abnormal hypervascularity was seen leading to the suspicion of iatrogenic arterial injury. Such a localized area of focal increased vascularity with very hyperdynamic flows within the endometrium typifies an iatrogenic arteriovenous fistula (AVF), a single communication between an artery and vein without the normal intervening capillary bed or vascular nidus. Spectral pulsed Doppler evaluation of the identified area in these cases will normally show a very low resistive index (RI) blood flow waveform with high peak velocities and evidence of flow turbulence. The waveform is usually broad with an irregular spectral envelope.9,10 The uterine artery typically is the primary vascular supply to the uterus with the venous channels following a similar course to the arteries. 1 Acquired uterine AVFs may occur after surgery, pregnancy, delivery, or trauma (including iatrogenic trauma). 7
The overall goal of treatment for an iatrogenic AVF is to eliminate the direct arteriovenous connection. The literature has shown significant advancements in the treatment of iatrogenic AVFs in recent years. AVF treatment of a single arteriovenous connection through transcutaneous techniques can be a straightforward procedure.7,10 Therapy can be achieved through coil embolization at the fistula site or by placement of a covered stent graft to eliminate the arterial to venous connection. For embolizaton, metallic coils are the preferred choice because of the risk of shunting of injected particulate embolic material into the systemic circulation via the high velocities in the fistula. Selective catheterization of the vessels close to the fistula and control of the flow must be accomplished,10,11 and the precise materials used will then depend on the size of the vessels, accessibility to the vessels and the amount of flow of the AVF. The advantages of ultrasound-guided transcutaneous embolization of uterine AVF versus such techniques as surgical intervention include superior success rates, lower complication rates and preservation of fertility. The complications are infrequent, but there is the risk of contamination/infection following ultrasound-guided transcutaneous embolization.1,12
While there have been several interventional advances in recent years, it is also possible for an ateriovenous fistula to resolve without any intervention. Itoh et al reported a case where a patient experienced such a resolution. 6 The 34-year-old patient reportedly had to have a Caesarean section after a placental abruption. This patient was later noted to have massive vaginal bleeding, and a mass was seen in the endometrium on magnetic resonance imaging (MRI). GTD was also ruled out in this patient because of low beta-hCG levels. Transvaginal Doppler sonography showed significant vascularity within this mass, and it was determined to be an AVF 28 days post–caesarean section. No intervention was done and the patient appeared to have complete resolution 10 days after the original detection of the fistula.
The patient presented in this report also appeared to have had a complete resolution of the AVF without surgical or percutaneous intervention. She returned to the ED 3 months after her second visit with a complaint of pelvic pain. There was no new medical history according to the patient. The sonographic findings were reported as normal. Her uterus was found to measure 6.3 cm, the endometrial canal measured 6 mm in thickness (compared to her visit 3 months prior where the endometrium measured 2.3 cm), and the ovaries appeared normal in size without evidence of free pelvic fluid. In addition, no adnexal masses were identified. While the patient reported no additional procedure, the uterus, ovaries, and endometrium now appeared normal on transabdominal and transvaginal sonography, with no residual evidence of the AVF.
Important central themes in this case study to the field of sonography include having a good understanding of clinical findings, which include symptomatology, correlation with laboratory findings, and appropriate patient care. Differential diagnoses in gynecological sonography may comprise a long list of possibilities. Use of good color and spectral Doppler techniques are essential in narrowing this list; without skilled use of color and spectral Doppler the thickened endometrium could be interpreted solely as infection and the diagnosis of AVF not considered. Furthermore, the sonographer must use adequate communication and patient care skills. In the case presented, the sonographer discussed a recent D&C with the patient, which presented as a caution to consider iatrogenic injury for the sonographer performing the study. This led to the decision to add color and spectral Doppler evaluation to the examination.
Conclusion
It is recommended that in cases of suspected iatraogenic endometrial injury that a transvaginal sonographic scan and color Doppler assessment be performed to exclude this rare but dangerous postprocedural abnormality. Correlation with clinical findings, which is always relevant to the diagnosis, can help clinicians identify the most likely pathology. Given this patient’s history of recent D&C procedures, transvaginal sonography was the diagnostic test of choice. Color and spectral Doppler evaluation are additional necessary tools to make the correct diagnosis in the case of endometrial arterial injury. The significance of this case is that it shows the importance of sonography in reaching a good outcome when there are multiple possible differential diagnoses. It is important to consider the relevant and most probable diagnosis with regard to sonographic appearance, medical/surgical history and clinical findings. It is crucial to the field that sonographers consider the important role that they play beyond the capacity to operate a machine and realize that they can greatly benefit from the skill of listening carefully to their patients’ medical histories and current symptoms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.