
Abstract
Intrahepatic cholangiocarcinoma (Klatskin tumor) is a rare fatal disease that originates from biliary epithelium. This tumor may arise anywhere within the biliary tree, intrahepatic bile ducts, or common bile ducts, and it accounts for approximately 2% of all reported cancers. A case is reported of an elderly male patient presenting with chronic occlusion of the right portal vein and diagnosed with intrahepatic cholangiocarcinoma. This report details the initial sonographic findings, the correlating follow-up imaging studies that were done, and patient management.
Cholangiocarcinoma (bile duct cancer) is an uncommon malignancy arising from the epithelial cells of the biliary tract. These tumors may arise anywhere along the intrahepatic or extrahepatic biliary tree. Patients with cholangiocarcinoma typically present at advanced stages; therefore, cure rates are low, even with aggressive therapy. The reported incidence of cholangiocarcinoma is 1 to 2 cases per 100,000 patients in the United States, with the majority of patients >65 years of age. 1 Cholangiocarcinomas become symptomatic when the tumor obstructs the biliary system, causing fatigue, nausea, abdominal pain, fever, weight loss, jaundice, clay-colored stools, and/or dark urine. Sonography is one of the first imaging modalities ordered by physicians to obtain images of the liver, bile ducts, and gallbladder. Sonography has been found to be 98.78% sensitive and 83.33% specific in cholangiocarcinoma. 2 Sonography can provide essential information in diagnosis with size, echogenicity, shape, boundary, and ductal dilatation in regard to the tumor.
Case Report
An elderly male patient was referred for liver sonography evaluation due to increased fatigue, nausea, and an elevated alkaline phosphatase of 329 U/L (normal, 24-110 U/L). The sonogram of the liver was done with a Philips iU22 sonography system (Philips Ultrasound, Bothell, Washington) using a C5-2 curved array transducer. Sonographic imaging showed a heterogeneous mass (10.3 × 10.3 × 13.7 cm) located within the posterior right hepatic lobe (Figures 1 and 2), with a peripheral ring of hypoechogenicity. The remainder of the liver was normal in appearance with no evidence of ductal dilatation. The liver mass showed vascularity around the periphery and appeared to be solitary (Figure 3), with no evidence of cirrhosis documented. Additional blood tests were requested, which showed an elevated alpha-fetoprotein of 30.2 ng/mL (in adults, normal values <10 ng/mL).

Longitudinal gray-scale image of the liver shows a mass measuring 10.3 × 10.3 cm (arrows). The mass was noted to be in the posterior right hepatic lobe, with heterogeneous echogenicity and a peripheral ring of hypoechogenicity.

Transverse gray-scale image of the liver illustrates this mass with a measurement of 13.7 cm in this dimension (arrows).
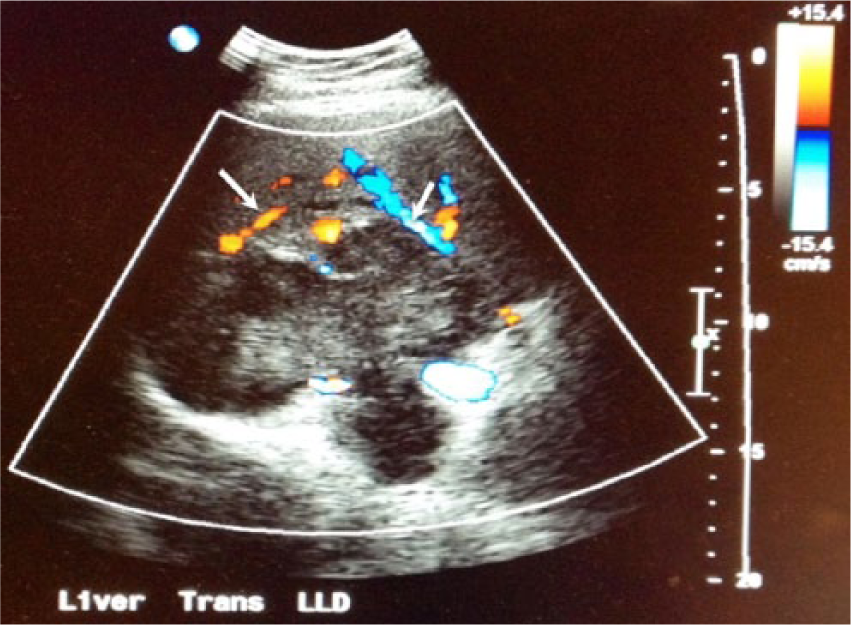
Transverse color Doppler image of the liver mass indicates vascularity around the periphery (arrows) with no significant intravascular component.
Based on the sonography findings, a history of cancer, and an elevated alpha-fetoprotein, a computed tomography (CT) examination of the chest, abdominal, and pelvis was performed. The CT scan identified a large right medial hepatic lobe mass (11 × 10.8 × 9.4 cm; Figure 4) involving the anterior and posterior segments as well as the caudate lobe, with tumor extension from the hepatic dome to the inferior margin. The proximal right portal vein was noted to be occluded. The distal right hepatic vein was not visualized. There was no evidence of ductal dilatation. In addition, there were multiple enlarged lymph nodes. Differential diagnoses that were reported included primary liver tumor versus metastatic lesion. The rest of the CT examination was normal. This tumor was inconclusive with imaging alone, and further assessment was completed by a CT-guided liver biopsy (Figure 5). Three core biopsy specimens of the lesion were obtained with an 18-gauge biopsy needle. A single-core biopsy specimen of normal left-lobe liver tissue was obtained with a 14-gauge biopsy needle. The biopsy specimens showed a bland fibrohistiocytic proliferation with associated lymphoplasmacytic infiltrate. There was question in regard to immunoglobulin G4–related sclerosis diseases versus an inflammatory myofibroblastic tumor, such as cholangiocarcinoma.

Cross-sectional computed tomography image of the liver shows a large right medial hepatic lobe mass (arrows) involving the anterior and posterior segments as well as the caudate lobe, with the tumor extending from the hepatic dome to the inferior margin. The mass measured 11 × 10.8 × 9.4 cm, with a proximal right portal vein occlusion. The distal right hepatic vein was not visualized.

Cross-sectional computed tomography image taken during a guided-liver lesion biopsy illustrates the needle track for the biopsy (arrows).
The patient was admitted to the hospital for a planned right hepatectomy with caudate lobe resection. Exploratory laparotomy with lysis of adhesions was first done, and on visualization of the left lobe of the liver, there was noted to be a 12-mm hard nodule concerning for metastatic disease. The surgeon chose not to proceed because of frozen section histopathology consistent with carcinoma. Pathology from the left-lobe liver nodule showed patchy cytokeratin 19 staining, focally positive for cancer antigen 19-9, suggestive of moderate to poorly differentiated cholangiocarcinoma.
One week later, the patient was started on chemotherapy, receiving gemcitabine injections (1000 mg/m2) on days 1 and 8 and cisplatin injections (25 mg/m2) on a 21-day cycle. After the cycle was completed, a magnetic resonance imaging (MRI) study was done, which showed that the main mass in the liver was significantly smaller (Figure 6). It had decreased from 10.9 × 8.3 cm to 8.1 × 5.3 cm. The peripheral left-sided cholangiocarcinoma was also noted on MRI of the abdomen, with no significant change. There were some scattered portal hepatic and retroperitoneal lymph nodes that appeared to be less prominent than those of prior studies. Considering these results, the gemcitabine and cisplatin doses were reduced and continued at 750 mg/m2 and 20 mg/m2, respectively.
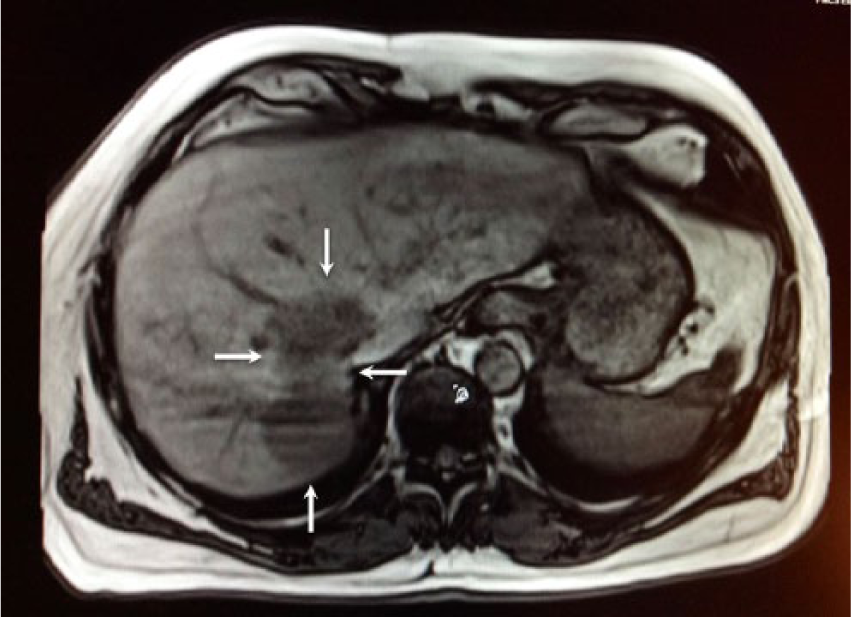
Cross-sectional magnetic resonance image of the abdomen, taken 11 months after the patient initiated chemotherapy with gemcitabine and cisplatin cycles, indicates that the mass in the liver had decreased from 10.9 × 8.3 cm to 8.1 × 5.3 cm (arrows).
Four months later, the patient had successful coil embolization of the gastroduodenal and right gastric arteries in preparation for microsphere embolization (TheraSphere; Theragenics, Buford, Georgia). The embolization procedure consisted of direct catheter-based left hepatic arterial injection of millions of small glass microspheres (20-30 µm in diameter) containing radioactive yttrium 90, allowing the treatment to be delivered directly to the tumor via blood flow. 3 The microspheres embolize, lodging themselves in the capillaries of the tumor. One month later, microsphere embolization was done via the right and medial hepatic arteries. Five months after the embolization, a CT scan was repeated (Figure 7), revealing the right posterior hepatic mass of known cholangiocarcinoma had slightly decreased in size, with new tumor invasion of the right portal vein, right hepatic vein, and inferior vena cava. After discussion with the patient of all the new findings and treatments completed, a right hepatic resection was recommended.
Corresponding cross-sectional computed tomography image illustrates the right posterior hepatic mass of known cholangiocarcinoma with slight interval decrease in size and with new tumor invasion of the right portal vein, right hepatic vein, and inferior vena cava (arrows).
The patient had an extended right hepatectomy. A sonography-guided nontargeted biopsy (Figure 8) of the left hepatic lobe parenchyma was done to evaluate for any further liver disease. Two core biopsies were reviewed, and histopathology showed normal liver parenchyma. Resection of the total right lobe of the liver and left-lobe nodule was successful, with the intraoperative course complicated by loss of blood pressure. A postoperative CT scan of the chest (Figure 9) showed a subsegmental pulmonary embolism. The patient was immediately placed on enoxaparin sodium (Lovenox) at 1 mg/kg.

Transverse gray-scale sonographic image of the liver, taken during guided nontargeted biopsy (Figure 6) of the left hepatic lobe parenchyma to evaluate for any further liver disease, shows the needle during the biopsy (arrow).
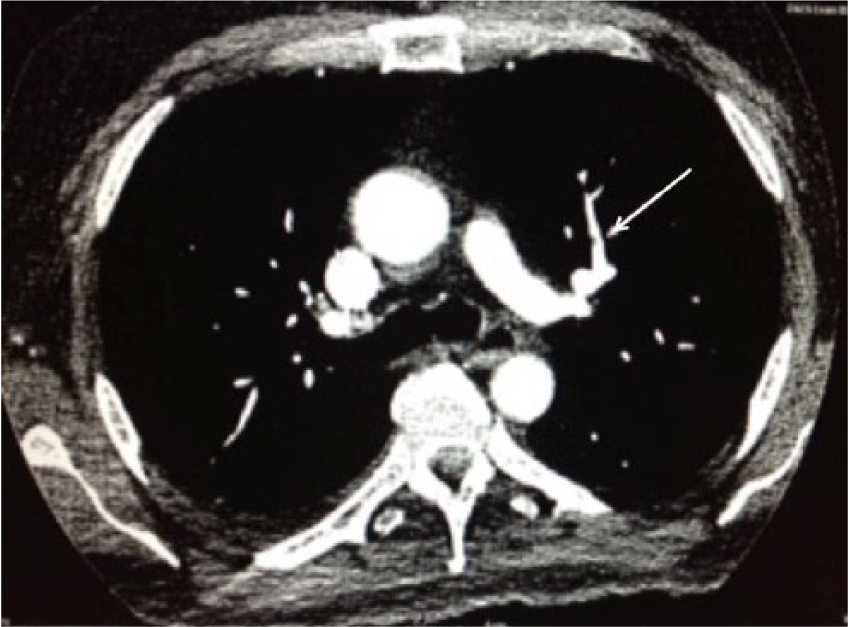
Postoperative computed tomography image of the chest indicates a subsegmental pulmonary embolism (arrow), which had caused a loss of blood pressure.
Intraoperative histopathology of the right lobe resection showed no evidence of malignancy identified within the left lobe of the liver following biopsy. However, there was visualization of carcinoma of the intrahepatic bile duct (cholangiocarcinoma) in the biopsy of segments 4 to 8. At the caval-margin excision, necrotic tumor was present at the suture line, and the surrounding liver parenchyma was involved with moderately differentiated cholangiocarcinoma. A second caval-margin excision line was created, and again moderately differentiated cholangiocarcinoma was visualized at the suture. A final revised caval-margin excision was negative for tumor. Postoperatively, a liver Doppler sonogram identified the left portal vein and left hepatic vein to be patent (Figure 10), with flow moving in the hepatopetal direction. The hepatic artery was not well visualized secondary to obstructing dressings around the liver.
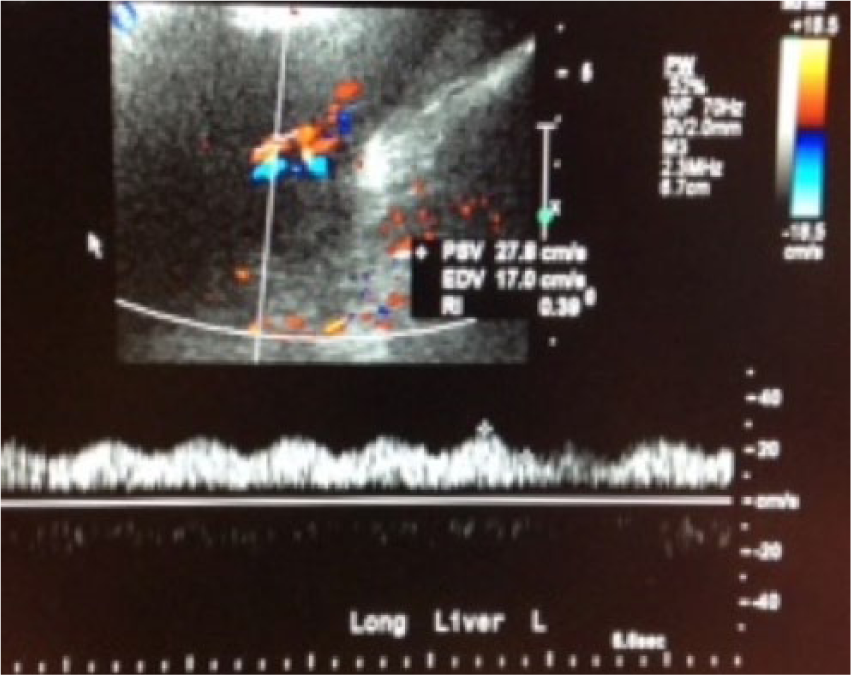
Color Doppler image shows patency of the left portal vein (with corresponding spectral Doppler trace) and the left hepatic vein, with flow moving in the appropriate directions.
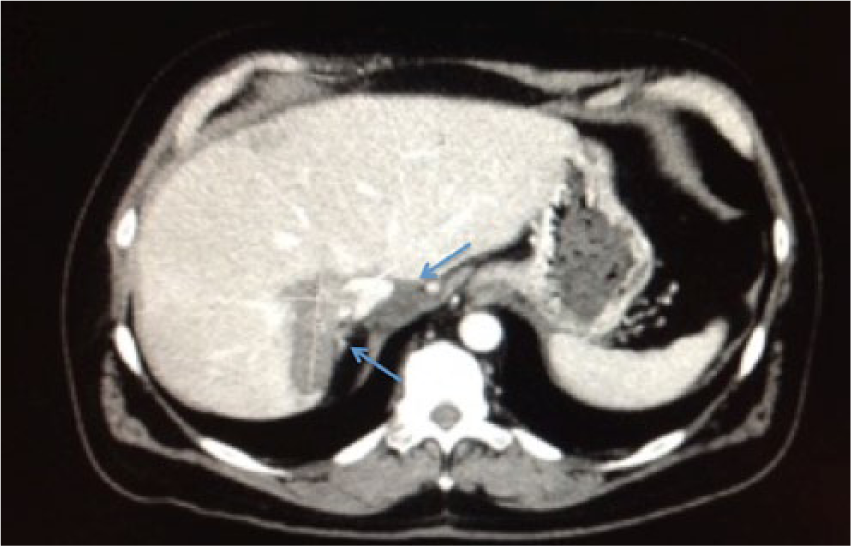
Two months after the resection, MRI showed the right hepatectomy with no evidence of recurrent or metastatic cholangiocarcinoma in the left lobe of the liver. A small wedge-shaped defect along the anterior portion of the left liver was seen, correlating with the prior resection of a nodule (Figure 11). Bile ducts were normal in caliber, and the pancreas, spleen, adrenal glands, and kidneys were within normal limits. Serum blood testing showed that alkaline phosphatase decreased from 329 to 78 U/L (normal, 24-110 U/L). The patient went on to an uneventful recovery and was able to return to work after approximately 1 year of treatment and surgery.

Cross-sectional computed tomography image of the abdomen, taken 2 months after the resection of the right lobe of the liver, illustrates the site of the right hepatectomy (blue arrows). The left lobe of the liver showed no evidence of recurrent or metastatic cholangiocarcinoma, with a small wedge-shaped defect along the anterior portion of the left liver secondary to a prior resection of a nodule (white arrow).
Discussion
Cholangiocarcinoma is a malignant tumor arising from the epithelium of the bile ducts. Most of these tumors are adenocarcinomas. Intrahepatic cholangiocarcinoma accounts for 10% of all cholangiocarcinomas, hilar cholangiocarcinoma for 25%, and extrahepatic cholangiocarcinoma for 65%. 1 Intrahepatic cholangiocarcinoma typically presents as a large mass because the tumor does not cause clinical symptoms in its early stages, whereas extrahepatic cholangiocarcinoma is usually small at the time of presentation. 3 Most patients are ≥65 years old by the time of diagnose. Patients present with general symptoms, such as abdominal pain, jaundice, dark urine with pale stools, chills, fever, weight loss, fatigue, and loss of appetite.
Cholangiocarcinoma is diagnosed through a combination of blood tests, imaging, and biopsies. Cholangiocarcinoma is difficult to diagnose definitively with only blood test tumor markers such as cancer antigen 19-9 and alpha-fetoprotein, as these tests are often suggestive but not diagnostic. Imaging, including sonography, CT, and MRI, are used to coordinate for tumor location, bile duct visualization, and blood flow to determine whether the tumor is resectable. The anatomic location of cholangiocarcinomas can make resection difficult; therefore, preoperative assessment typically requires several modalities to be certain that the patient qualifies for tumor resection. Sonography is usually the first imaging modality recommended for patients who arrive with nausea, vomiting, pain, or jaundice. The sonographic appearance of cholangiocarcinomas may vary. Tumors are usually homogeneous in appearance, with a peripheral hypoechoic area and perilesion vascularity but no significant intralesion blood flow. In CT and MRI scans, intrahepatic cholangiocarcinoma usually appears as a homogeneous low-attenuation mass with irregular peripheral enhancement, and it can be accompanied by capsular retraction, satellite nodules, and peripheral intrahepatic duct dilatation. 4
Radical surgical resection remains the only treatment with a potential cure for patients with cholangiocarcinoma. However, only 10% of cholangiocarcinomas are surgically resectable. 5 Tumor resection after hepatic infusion chemotherapy and embolization is feasible and has become an option to cure selective patients with cholangiocarcinoma. Unresectable cholangiocarcinoma may be treated with chemotherapy and radiation. Chemotherapy drugs that have been used for cholangiocarcinoma include fluorouracil, cisplatin, doxorubicin, and gemcitabine. 6 In addition to chemotherapy, microsphere embolization can be done.
Patients with cholangiocarcinoma have higher risk factors of recurrence; therefore, aggressive surveillance of this tumor is recommended by physicians. In patients undergoing aggressive surgery, 5-year survival rates range from 10% to 40% for cholangiocarcinoma. 7 Prognosis is greater for those with extrahepatic tumors who are suitable for early surgical intervention. Intrahepatic lesions carry the worst prognosis.
CT is presently the standard imaging technique in most institutions for monitoring cancers of the abdomen and pelvis. It is used routinely for detecting local recurrences or liver metastases.7,8 However, sonography can play an important role as a rapid, accurate modality for imaging the liver, and sonographic examinations are often ordered as part of the screening process for liver mass and for correlation with CT.
Conclusion
This case reports the findings of an intrahepatic cholangiocarcinoma. The initial sonogram revealed the liver lesion with characteristic features. Additional imaging modalities were necessary to completely assess the size and location of the mass. Sonography-guided biopsy was performed to evaluate the liver parenchyma prior to liver resection. Since cholangiocarcinomas have a high risk of recurrence, sonography can also be helpful as a follow-up screening tool for any liver mass.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.