
Abstract
Diagnostic medical sonography is viewed as a safe imaging modality. However, bioeffects research has yet to define the effects of exposure to sonography in humans. Therefore, sonographers must be aware of potential risks and practice ALARA (“as low as reasonably achievable”) routinely. This research explores sonographers’ ability to answer basic questions about the bioeffects of sonography, as well as their knowledge and use of the safety indices called the mechanical index (MI) and thermal index (TI). Members of the Society of Diagnostic Medical Sonographers, a southwestern sonographers’ society, and a sonography community on Facebook 2010 were surveyed. There is a low level of bioeffects knowledge and minimal safety practices among sonographers in this survey. No significant relationship was found between sonographer knowledge of the bioeffects of sonography, years in the profession, or whether the sonographers monitor the MI/TI.
Diagnostic medical sonography is a valuable imaging tool that provides real-time, dynamic information for an array of medical conditions. Because sonography does not expose patients to ionizing radiation, most medical professionals and the public consider it safe. Evidence has shown that under certain circumstances, adverse biologic effects can occur, but studies have failed to provide conclusive evidence that sonographic exposure causes damage to human tissue. The assumption that sonograms are safe to perform on humans is based not on safety data but predominantly on a lack of evidence of harm. Therefore, safety practices within the profession are based on the premise that biologic effects are possible but not likely to occur in humans and that the principle of “as low as reasonably achievable” or ALARA is adequate to protect humans from any potential harm. Applying the ALARA principle means that the operator should use only the lowest possible acoustic output power required to achieve the best possible diagnostic sonogram. ALARA requires that sonographers and other operators such as physicians, residents, and nurses bear the responsibility to minimize the risk of harm to the patients.
Regulatory History of Sonography
The Food and Drug Administration (FDA) is responsible for regulating medical devices within the United States. In 1976, the FDA placed the first acoustic output limits on sonographic equipment. 1 Limits were set for four categories of scanning: fetal (94 mW/cm2), cardiac (430 mW/cm2), peripheral vascular (720 mW/cm2), and ophthalmic (17 mW/cm2) imaging. 2 The maximum acoustic limits were based on the acoustic output levels of machines used prior to 1976 because it was felt that no adverse effects had been identified at those intensity levels. 1 However, pre-1976 limits were never tested specifically for safety.
The FDA explored tighter regulations on acoustic outputs in the early 1990s. Many organizations within the sonography community favored removal of the upper limits, allowing the operator to monitor the output levels and adjust the patient sonographic exposure according to ALARA. 2 It was believed that removal of upper limits would benefit the patient by offering improved imaging and diagnostic capabilities. However, some organizations believed the examination-specific upper limits were necessary to maintain patient safety. 2 The FDA removed application-specific acoustic output limits but retained a maximum overall output limit of 720 mW/cm2for general, cardiac, and obstetric imaging. 2 This change to the global acoustic output limit created the possibility for nearly an eightfold increase in acoustic output capabilities in the case of obstetric imaging. 3 The only exception to the overall maximum output of 720 mW/cm2 was with ophthalmic imaging, in which limits increased from 17 mW/cm2 to a maximum output of 50 mW/cm2,3.
The FDA approval of the increased acoustic output limits included additional stipulations. Manufacturers were required to incorporate a built-in notification system that alerted operators when acoustic energies reached levels capable of producing biologic effects. In addition, the American Institute of Ultrasound in Medicine (AIUM) was to provide education so that all operators have knowledge in how to interpret the notification system and how to adjust machine settings properly to accomplish the ALARA principle. These conditions were met with the incorporation of the Output Display Standard (ODS) on sonography machines, which serves as the warning system for the operator, and the publication of the educational brochure Medical Ultrasound Safety, produced by the AIUM, which provides basic bioeffect and safety information. 3
The ODS includes the mechanical index (MI) and thermal index (TI), and they are displayed on all machines manufactured after 1992. These indices are indicators for the risk of producing adverse effects in the body through cavitation and heating, respectively. Cavitation occurs in two forms: transient, or inertial, cavitation and non-inertial cavitation. Of the two, transient cavitation produces a greater risk for biologic damage and is the basis for the mechanical index.3–5 Transient cavitation is the expansion and rapid collapse of gas bubbles, which is capable of producing high temperatures, shock waves, and free radicals. 6 Thermal effects result from tissue absorption of sound, in which the acoustic energy is converted to heat. The rate of absorption is dependent on tissue type. Therefore, the thermal index is divided into three categories: TI for soft tissue (TIS), TI for bone (TIB), and TI for cranial bone (TIC). 3
For the mechanical and thermal indices, a value greater than 1.0 represents the potential to create biological effects. 3 The indices are not representative of an actual mechanical or thermal change but represent the potential for such to occur. Mechanical and thermal effects are dependent on factors such as acoustic output, scanning mode (B-mode, M-mode, Doppler, etc.), focal zone position, frame rate, and dwell time (or how long the sonographer maintains the transducer in a stationary position over the area of interest).3,4 These factors can vary throughout the procedure and are under the control of the sonographer. 4 Not all of these factors are considered in calculating the biologic indices yet play a large role in the actual production of thermal bioeffects. 7 Thus, the indices are only a prediction of what could occur rather than what actually occurs. Operator awareness of MI/TI alone is insufficient to monitor patient safety. Knowledge of the multiple factors that contribute to the creation of biologic effects and how to minimize them, including how to limit dwell time, proper equipment operation, and how to monitor the MI/TI, are essential to incorporating the ALARA principle into performing a sonogram.
The shift from FDA regulation of specific acoustic output limits to allowing the operator to self-regulate requires an understanding of sonographic bioeffect principles and the ability to interpret the ODS. This type of understanding is best appreciated through formal education in sonography. However, operators are not required to demonstrate competence in bioeffects or safety knowledge by any regulatory body through formal education, credentialing, or any other method of demonstrating competence. The obligation is voluntary, and currently, little is known about how much safety knowledge operators have about sonographic energy or how they practice ALARA when performing sonograms.
Biologic Effects Education
The Commission on Accreditation of Allied Health Education Programs requests accredited diagnostic medical sonography programs to provide their students with education on sonographic bioeffects, pertinent in vitro and in vivo studies, exposure indices, ALARA principles, and the generally accepted maximum safe exposure level. 8 For many sonographers, their formal education may be the only time they receive bioeffects education, unless continuing medical education in the area of bioeffects and safety is pursued by attending seminars, reading journal articles, or reading textbooks. In addition, sonographers who entered the profession prior to the development of formal educational programs may have received their biological effects knowledge in more self-directed ways such as reading journal articles and textbooks. Another common time to receive bioeffects education is with the purchase of a new sonography machine. The FDA has set forth specific guidelines to include educational material detailing ALARA practices with all newly manufactured machines. In addition to the AIUM publication Medical Ultrasound Safety, which is a general overview of bioeffects and safety content, manufacturers should provide information specific to the device being marketed.3,9 Sonographers have the choice of reading the information if they choose. The credentialing organizations do test for knowledge of bioeffects and safety as part of the credentialing examinations; however, there are no regulations requiring sonographers (except in select states) to obtain credentials and/or licensure to practice. Nor is there a requirement that sonographers continue to update their bioeffects and safety knowledge through continuing medical education.
Operator Knowledge of Sonographic Bioeffects
A few surveys have been conducted to assess how much the operators are informed about the current safety guidelines.10–12Maršál 10 distributed a questionnaire to 199 professionals who performed fetal sonograms across nine European countries. Most of the professionals who responded were physicians (145), followed by midwives (32) and sonographers (22). 10 Results showed that 69 respondents (35%) were able to define the abbreviation MI, and 64 (32%) respondents could define the abbreviation TI. However, when it came to identifying the distinctions between TIS, TIB, and TIC, 12 (6%) could provide a correct answer for TIS, 16 (8%) could describe TIB, and only 5 (3%) could adequately describe TIC. 10 When asked to provide definitions of MI and TI, 43 (22%) respondents could adequately describe TI, and 21 (11%) could describe MI. 10 Fifty-six respondents (28%) claimed to know where the ODS was located in the equipment, and only 43 (22%) could identify how to adjust the acoustic output power on the equipment. The respondents in this study demonstrated a poor ability to describe and locate the safety indices that are displayed in the ODS.
Sheiner et al. 11 distributed a questionnaire at an obstetrics and gynecology (OB/GYN) review course, a general sonography imaging review course, and two hospital OB/GYN grand rounds. The questionnaire assessed operator knowledge of bioeffects in obstetric scanning as well as opinions on routine sonograms in low-risk pregnancies. Of the 130 respondents, 82 (63%) were physicians, 41 (32%) were sonographers, and 7 (5%) were nurse practitioners. 11 Results showed that 42 (32%) respondents were familiar with the term TI, and 29 (22%) were familiar with MI. Twenty-seven respondents (20.8%) could locate the MI/TI display on their sonographic systems. 11 Only 22 (16.9%) respondents could adequately describe the relationship between temperature increases and the potential teratogenic effects on the first-trimester fetus. 11 When the researchers noted how physicians answered the survey compared with other nonphysician users, the researchers found no differences between the answers of physicians versus answers of the other nonphysician users. 11 The researchers did discover that a linear relationship existed between the knowledge of sonographic bioeffects and the belief that there should be a limit to the number of obstetric sonograms performed during a low-risk pregnancy. 11 The respondents in this study had poor knowledge of biologic effects and the safety indices, but this study also demonstrated that the respondents’ knowledge influenced their attitudes toward safety, with the higher levels of knowledge leading to more conservative attitudes toward safety.
Pisacaglia et al. 12 surveyed the Italian Society for Ultrasound in Medicine and Biology to assess member knowledge of sonographic safety. They collected demographic data as well as administered an 11-question multiple-choice quiz that assessed operator knowledge of bioeffects principles, the ODS, and current safety statements from the FDA, AIUM, and the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB). Of the 97 responses, 91 (93%) knew that tissue heating was associated with TI, 78 (80%) were aware that fetuses are at greater risk for biologic effects than adults, and 70 (72%) knew the acoustic output limits set by the FDA. Forty-seven participants (49%) could adequately describe the EFSUMB statement on safety, whereas 85 (88%) were familiar with the FDA limits on acoustic output. 12 The results indicated that the participants had a good understanding of general bioeffects terms and guidelines. Although this group did appear to have more knowledge than previous studies, the authors state that the respondents demonstrated an overall lack of knowledge and that improved operator education was essential. 12
The general lack of knowledge regarding safety parameters among the respondents to these surveys is discouraging given the role that sonographers and other operators have in the regulation of patient exposure to acoustic energy. Limitations to these studies include but are not limited to low statistical power; the fact that when questionnaires are mailed or e-mailed, there may be possible overestimations of knowledge because the respondents have opportunity to use reference material in answering the questions; lack of validation of the knowledge assessment tools; and lack of the ability to generalize the results to all operators or a subset, including sonographers, physicians, residents, and nurses.
Of the few research studies that have assessed the level of sonographic bioeffect knowledge in all operators, sonographers have made up approximately one-third of the respondents. There are currently no studies that assess bioeffects knowledge and safety practices in which respondents are only sonographers. The purpose of this research is to assess the level of sonographers’ knowledge of sonographic bioeffects, determine how often sonographers monitor the MI and TI during a sonogram, and determine if credentialing or longevity in the field leads to more knowledge and/or higher levels of safety monitoring (the MI/TI).
Materials and Methods
A three-part, institutional review board–approved, electronic survey (see appendix) was created using Survey Monkey. The survey link was posted for members of the Society of Diagnostic Medical Sonographers in the online discussion forums, e-mailed to members of a southwestern sonographers’ society, and posted to members of a sonography-based community on the social network Facebook 2010. The survey was available from February 22, 2010, to March 15, 2010. Participation in the survey was limited to individuals currently practicing in the field of sonography.
Section 1 of the survey collected demographic data, including years in the profession, credentials, and type of scans routinely performed. Section 2 evaluated the frequency of MI/TI monitoring during procedures and types of procedures in which MI/TI monitoring is performed. Section 3 consisted of seven multiple-choice questions that assessed sonographers’ knowledge of sonographic bioeffects and the MI/TI. These questions were similar to questions in the Sheiner et al. 11 and Piscaglia et al. 12 surveys. This section was scored to determine the relative knowledge level of participants regarding sonographic bioeffects principles. Each question in this section included the option “I don’t know” to avoid guessing. Answers to questions in section 3 were given a score of 0, 0.5, or 1. A score of zero was given for incorrect answers, and a score of 1 was given for correct answers. A score of 0.5 was given for partial answers to question 5, which asked at which stages of fetal development the fetus is most susceptible to biologic effects. The correct answer to this question was in the first and third trimesters.13–16 Therefore, any combination of answers, which included at least one of the two answers, was given a score of 0.5. If neither answer was selected, a score of zero was given. A score of 1 was given when the first and third trimesters were selected with no additional selections. Answers of “I don’t know” were considered incorrect in the calculation of the percentage. The maximum score possible for section 3 was 7. The correct responses were converted to a percentage. Participants were permitted to skip any question they did not wish to answer in accordance with the requirements set forth from the institutional review board.
Survey responses were analyzed using SAS 9.1 statistical software (SAS Institute, Cary, North Carolina). A nonparametric Kruskal-Wallis test was used to assess relationships between the total percentage correct on section 3 (using the previously discussed scoring method) and predictors that included credentialing status, years in the field, and the frequency of monitoring the MI/TI.
Separate Fisher exact tests were performed to determine, for each question in section 3, whether the probability of answering questions correctly (partially correct questions were regarded as incorrect) was associated with credentialing status and whether the respondent monitors the MI/TI. Separate logistic regression models were used to determine whether the probability of answering each question correctly was related to years in the field.
Results
A total of 212 responses were received at varying degrees of completion. All 212 respondents answered the question regarding credentialing, and 114 (53.8%) were RDMS, 65 (30.7%) were RDCS, 16 (7.5%) were RVT, 9 (4.2%) were not credentialed, 4 (1.9%) were credentialed with CCI, 2 (0.9%) were credentialed with the ARRT (U) designation, and 2 (0.9%) were ARRT (non-U) (Figure 1). Of the 191 respondents who chose to disclose the number of years in the profession, 51 (26.7%) have been in the field more than 20 years, 23 (12.0%) between 16 and 20 years, 36 (18.9%) between 11 and 15 years, 31 (16.2%) from 6 to 10 years, 38 (19.9%) from 2 to 5 years, and 12 (6.3%) from 0 to 1 year (Figure 2).
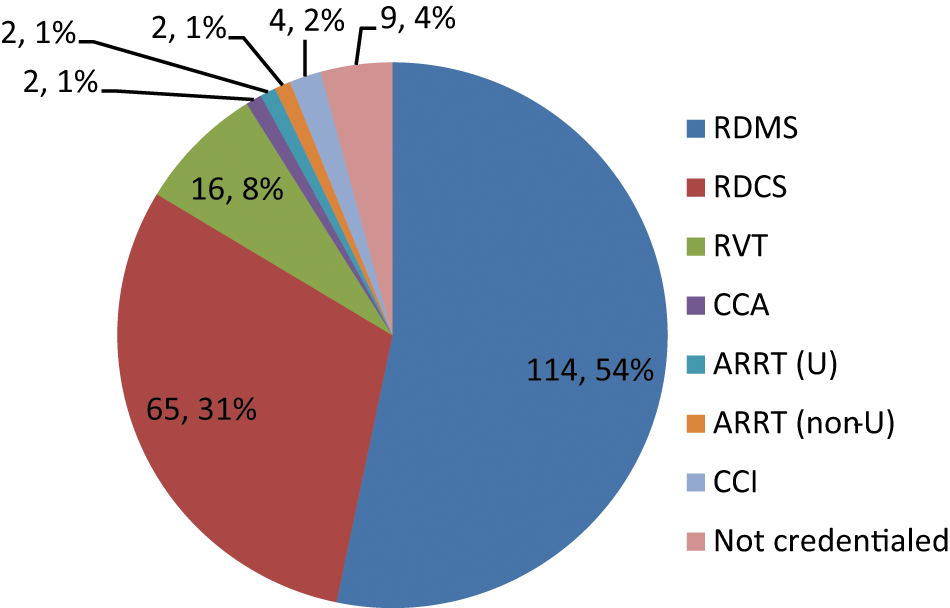
Demographic data: credentialing status.
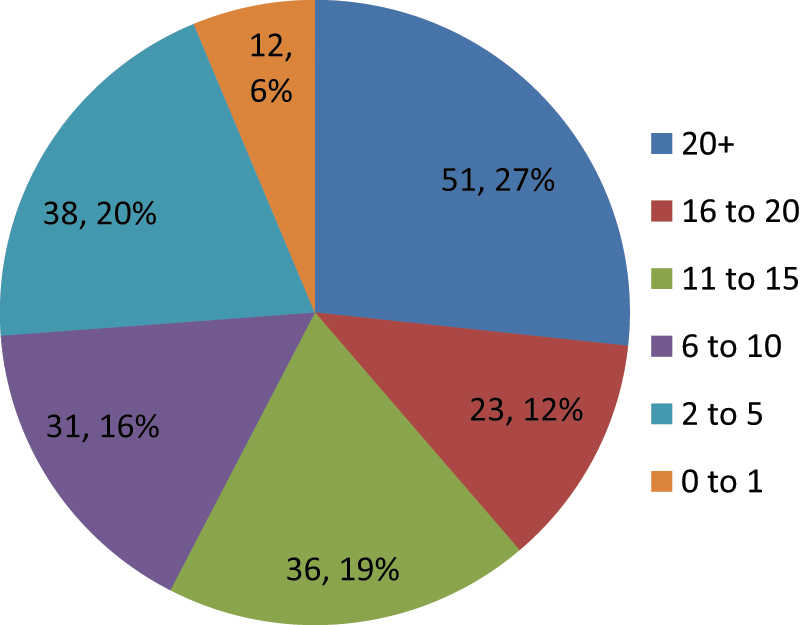
Demographic data: number of years in the profession.
When asked how often the sonographer monitors the MI/TI display during a procedure, of the 179 who chose to respond, 94 (53%) never monitor the MI/TI, 73 (40%) monitor one to two times per procedure, and 12 (7%) monitor MI/TI three to five times per procedure. There were no responses for monitoring six to eight or nine or more times per procedure (Figure 3).
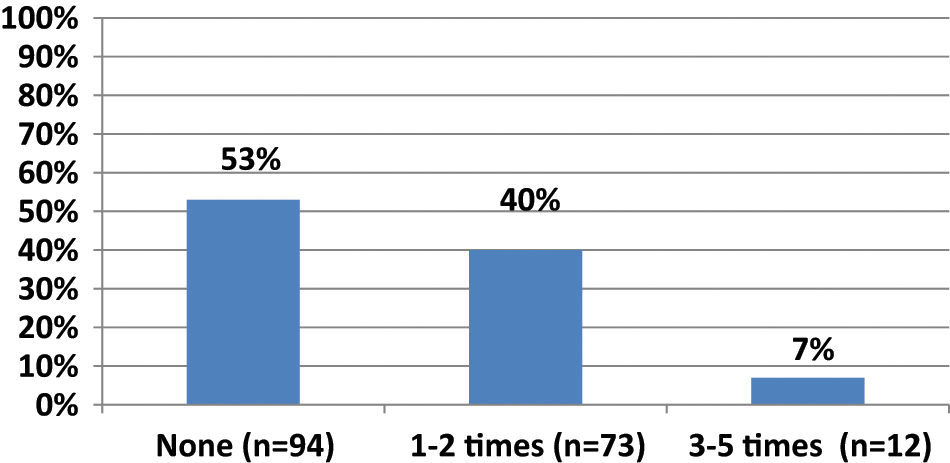
How often the respondents mechanical index (MI)/thermal index (TI) during each procedure.
In section 3, which assessed bioeffects knowledge, the highest percentage of correct answers was 78.6% and the lowest percentage was 0%. The mean percentage of questions answered correctly was 26.7%. When these questions were individually analyzed, 101 of 170 (59%) respondents knew that cavitation due to mechanical effects has been observed in mammals at pressure levels generated by diagnostic sonography equipment (question 3), and 25 of 164 respondents (15%) knew that mechanical effects did not increase temperature in the body (question 7). When asked about thermal indices (question 6), 59 of 163 respondents (36%) knew that a TI of 1 indicates a potential temperature increase of 1°C. Of the respondents who knew that the fetus is at a higher risk for bioeffects in the first trimester (129 of 167 responses or 77%), an additional 8 respondents (5%) could correctly answer that there is also an increased risk in the third trimester (question 5) (Figure 4).
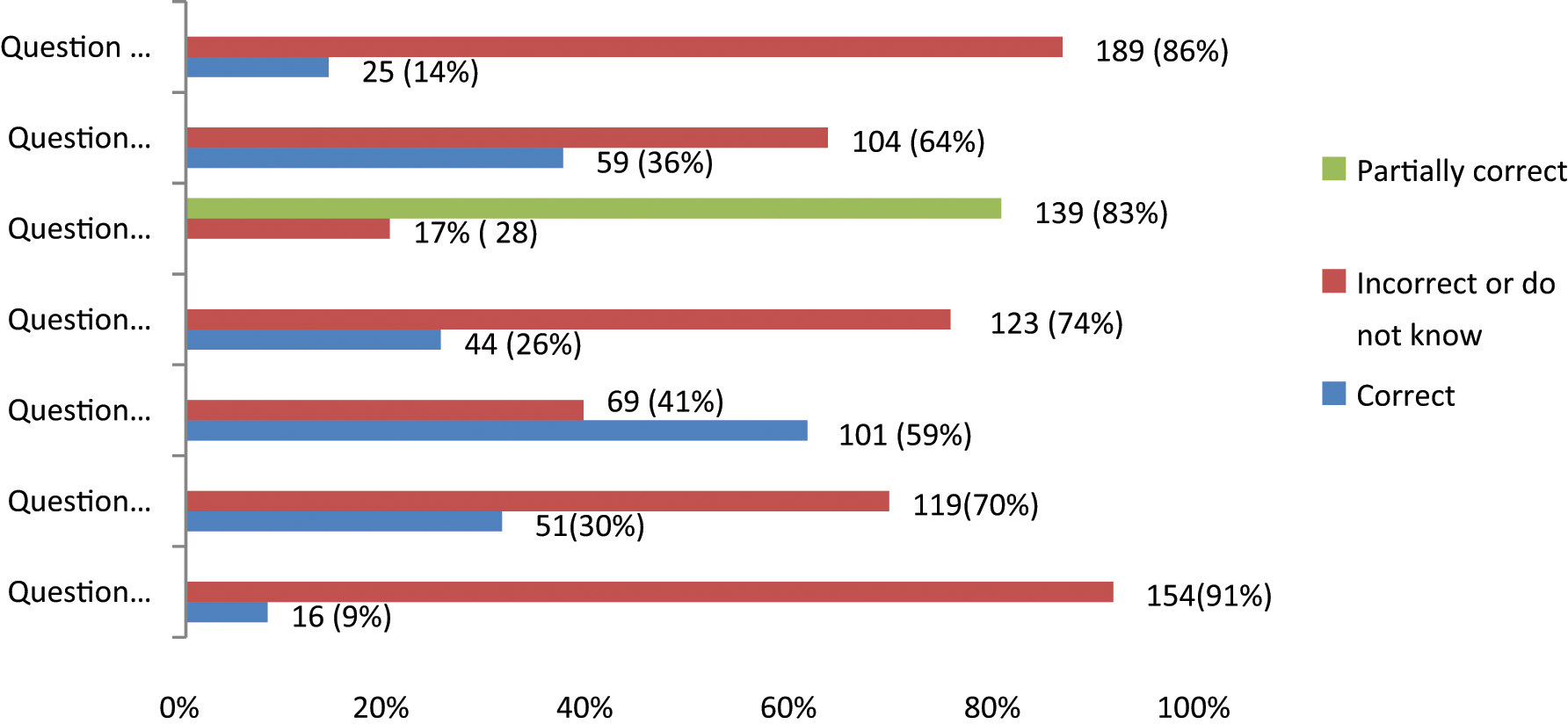
Individual question results for section 3 biologic effects knowledge.
The responses to section 3 were further analyzed to determine if the frequency of monitoring the MI/TI increased the probability of answering more questions correctly. For those who do not monitor, the mean percentage of questions answered correctly was 28%. For those who monitor one to two times per procedure, the mean percentage answered correctly was 35%, and for those who monitor three to five times per procedure, the mean percentage correct was 31%. Using a Kruskal-Wallis nonparametric test, the P value was .07, revealing that there was no statistical difference in the percentage of questions answered correctly by the frequency of monitoring (Figure 5). Because of the small size of those who monitor the MI/TI three to five times per procedure (n = 12), the data were combined to include only two categories: those who never monitor the MI/TI and those who do monitor the MI/TI. Those who reported monitoring the MI/TI either one to two times or three to five times per procedure were included in the “does monitor” category. The mean percentage of questions answered correctly was 35% for those who monitor the MI/TI and 28% for those who do not monitor the MI/TI. When the groups were divided this way, there was a statistical difference (P = .03) between those who monitor MI/TI and those who do not monitor MI/TI, with those that monitor the MI/TI answering more questions correctly (Figure 6).
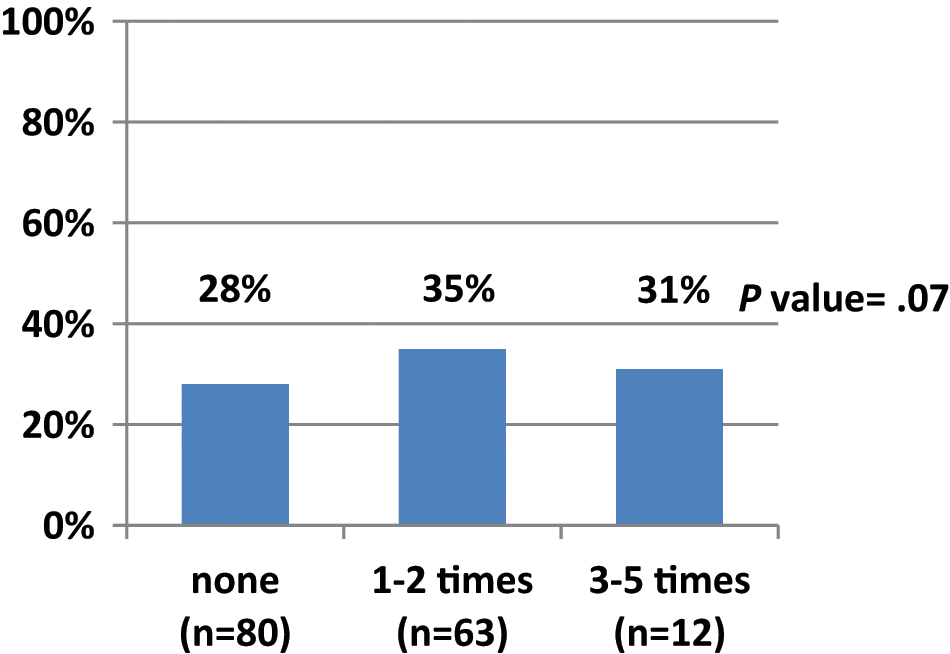
Percentage correct in section 3 by frequency of monitoring mechanical index (MI)/thermal index (TI) per procedure.
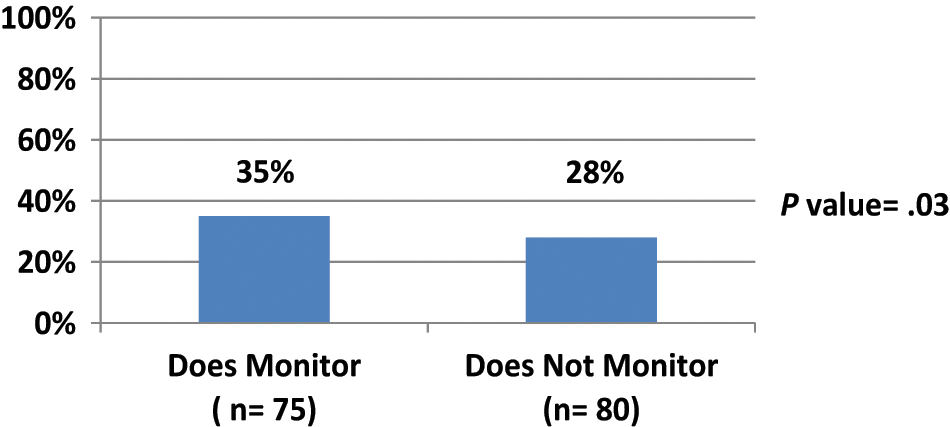
Percentage answered correct when monitoring was categorized as does or does not monitor.
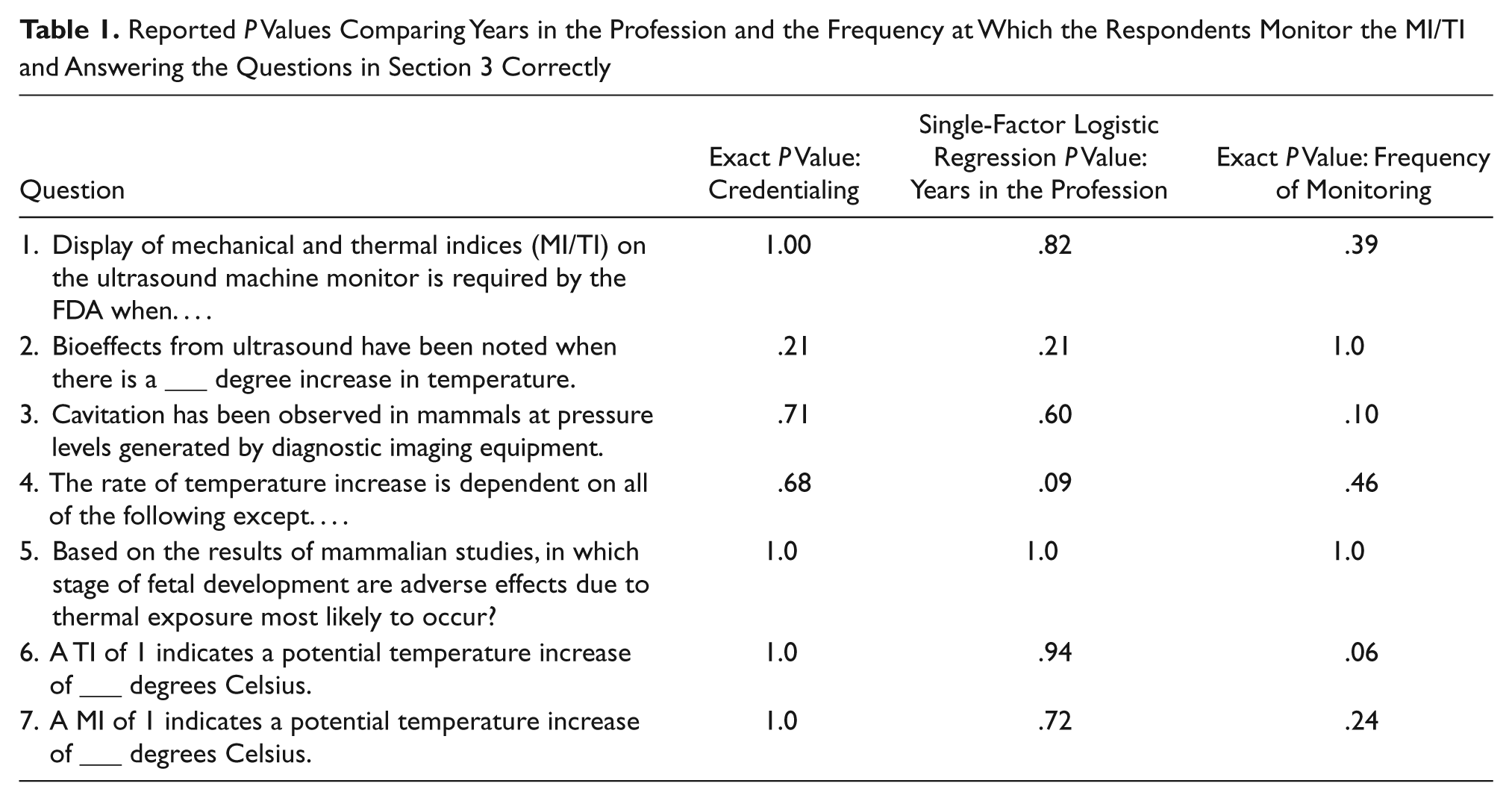
Years in the field were compared with the percentage of questions answered correctly in section 3 (see Table 1). The mean percentage of questions answered correctly was highest for the sonographers who were in the field two to five years who answered 34% of the questions correctly. The lowest mean percentage of questions answered correctly was the group of sonographers who were in the field 11 to 15 years, 28.7%. Using a Kruskal-Wallis test to compare all the categories of years in the field and the percentage of questions answered correctly, there was no significant difference (P = .92) between years in the field and probability of answering more questions correctly in section 3 (Figure 7).
Reported P Values Comparing Years in the Profession and the Frequency at Which the Respondents Monitor the MI/TI and Answering the Questions in Section 3 Correctly
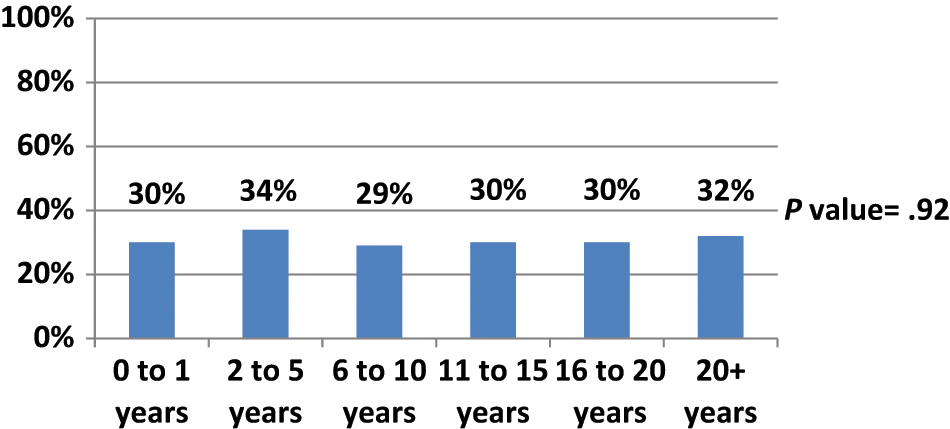
Percentage of questions answered correctly in section 3 by years in the profession.
Regarding credentialing status, because of the small number of responses for the ARRT(U) and CCI registrants, the categories were condensed into credentialed and noncredentialed. Any respondent who replied that he or she was registered with CCI, ARRT(U), RDMS, RDCS, or RVT was considered credentialed, and those responding noncredentialed or ARRT but not (U) were considered noncredentialed. One hundred eighty-one responses were categorized as credentialed, and 10 were categorized as noncredentialed. Using a nonparametric Wilcoxon test, the mean percentage of questions in section 3 that were answered correctly was 33% for the noncredentialed group and 31% for the credentialed group. The findings were insignificant (P = .83), and credentialing status did not appear to improve the probability of correctly answering a higher percentage of questions in section 3.
Each question in section 3 was analyzed individually and compared with years in the profession, credentialing status (credentialed or noncredentialed), and the frequency of monitoring (never monitors or does monitor). Fisher exact tests showed no significant relationships between the probability of answering any single question correctly in section 3 and credentialing status. When each question was compared with whether a sonographer monitors the MI/TI during a procedure, the only question that proved interesting was question 6: A TI of 1 indicates a potential temperature increase of __ degree Celsius? Of those who monitor TI, 45% responded correctly by answering 1°C versus the 28% of those responding correctly who do not monitor the TI. However, those differences also did not prove to be statistically significant (P = .06). Therefore, sonographers in this survey who are more attentive to the MI/TI are not able to answer more bioeffects questions correctly when compared with those who never monitor the MI/TI. When analyzed using single-factor logistic regression, years in the profession did not increase the probability of answering any question in section 3 correctly. Thus, a sonographer who is newly out of school/training does not appear to be able to answer more questions about bioeffects correctly when compared with veterans in the field and vice versa.
Discussion
Previous studies related to operator knowledge of sonographic bioeffects surveyed a broader participant group, including physicians, nurses, and nurse midwives who have professional responsibilities that are different from sonographers. Is it reasonable to expect sonographers to demonstrate more knowledge on the topic of sonographic bioeffects and safety as compared with other operators? This study focused on sonographers only and found that sonographers who answered this survey are lacking general knowledge of sonographic biologic effects principles based on a series of seven multiple-choice questions assessing biologic effects knowledge and assessed safety practices based on self-reported monitoring of the MI/TI. An overall high score of 78% and a mean score of 26% are noted.
The low level of knowledge and safety practices may demonstrate that sonographers responding to this survey do not think sonographic bioeffects are relevant enough to maintain a high level of knowledge or vigilant safety practices. There could be a presumption by these sonographers that the limits the manufacturers place on the systems do not allow for harmful exposure to the patient. During the debate when maximum acoustic energy limits were discussed by the FDA, then AIUM President John C. Hobbins, MD, suggested that an overall maximum limit may appear to protect a patient from exposure to inordinately high intensities of sonography. 2 Furthermore, this limit may suggest to an operator that any setting that is below the “upper limit” level is safe. 2 Additional research would need to be conducted to clarify this issue and learn why sonographers are lacking in their knowledge of sonographic bioeffects.
Of the respondents in this survey, 94 (53%) indicated that they never use the ODS to assess the MI/TI levels. This is troubling because the ODS is there to notify sonographers and other operators that the potential to produce bioeffects exists so that intensity levels and scan time can be adjusted appropriately. That sonographers in this study are not monitoring MI/TI appears to show insensitivity or lack of knowledge on the topic. Additional research is needed to further understand why sonographers do not monitor the MI/TI.
A limitation of this study was the method of distribution. Because the survey was sent electronically via e-mail, posted in discussion forums and in social media, there is no way to establish the exact number of people who received an invitation to the survey and therefore no way to calculate a return rate. Sonographers who opted to take this survey may not be representative of the entire profession, and therefore, the results are not generalizable to the whole profession. The survey had no time limit for completion once it was begun. Therefore, respondents may have looked up answers or collaborated with coworkers. If that were the case, the scores would be overestimated. Given that overall the percentage of questions answered correctly was low, it is doubtful that participants were collaborating or looking up answers.
An additional weakness of this study is the low numbers of noncredentialed sonographers, so the comparisons of knowledge and safety practices by credentialing status do not have enough power to detect any differences between the two groups if any differences do exist. Given the high numbers of credentialed sonographers in this survey and that the sonographic bioeffects knowledge and safety practices are low, increasing the number of noncredentialed sonographers in this survey is not likely to improve the level of knowledge or safety practices detected in this study. A final weakness is that the survey items were not pilot tested for errors prior to sending out to the community and that the questions in section 3 were not validated to ensure that they do measure true knowledge of bioeffects and safety monitoring. The responses in section 3 of this survey may not be indicative of true bioeffects knowledge. However, this study finds similarities with other surveys that share this drawback.11,17 When the answers are coupled with the low levels of self-reported MI/TI monitoring, the results appear to correlate unsurprisingly.
Sonographers’ education concerning sonographic bioeffects and safety is largely self-directed. Most physics textbooks contain chapters on bioeffects and safety, journal review articles adequately provide information, and seminars have been given for sonographers, but it is the responsibility of the sonographer to obtain the information and hold himself or herself accountable for the information. Additional research could be done to assess how many sonographers seek and/or attend continuing medical education in bioeffects and safety or how many choose to do self-directed readings from resources such as physics texts or the AIUM Medical Ultrasound Safety document. Further research could also assess sonographer knowledge of bioeffects and safety and compare it to how recently a sonographer attended a seminar on bioeffects and safety or participated in self-directed readings. In an editorial, Maršál 10 points out that many operators find the discussion of sonographic safety boring and/or difficult to understand. It could be helpful to know how many sonographers choose to attend continuing education activities related to sonographic bioeffects and safety.
Conclusion
Sonographers who answered this survey demonstrate limited knowledge of sonographic bioeffect principles and practice poor ALARA practices. These findings are similar to other surveys involving physicians and residents who provide sonograms to patients. It is difficult to theorize why sonographers put a low priority on these practices. It could be due to the lack of significant findings of bioeffects in humans, the low standards placed on bioeffects education, or the assumed inherent safety of current equipment. More education related to each of these areas could improve the safety practices of sonographers. The technologies used in sonography are continually changing. New operating modes and scanning techniques developed annually may increase the potential for bioeffects to occur. Because the intensities used in current sonography equipment have increased almost eightfold since the early 1990s, sonographers should do a self-assessment of sonographic bioeffects knowledge and safety practices and stay informed on the best ALARA practices for the optimal patient care and safety.
Footnotes
Appendix
Acknowledgements
The authors thank David M. Thompson, PhD, Department of Biostatistics and Epidemiology, The University of Oklahoma Health Sciences Center, for his support with the statistical analysis of data.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.