
Abstract
Objective:
The American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) is a reporting system for thyroid nodules detected with sonography and proposed by the ACR. The scoring of punctate echogenic foci (PEF) increases the TI-RADS score and leads to a biopsy of many thyroid nodules, otherwise found clinically. The aim of this study was to assess the risk of malignancy for mixed and solid nodules, with and without PEF, and cytologic correlation.
Materials and Methods:
Thyroid sonograms and ultrasound-guided thyroid biopsies were performed, at a University of Iowa Hospitals & Clinics for 105 patients, during July 2019 to June 2020. All these retrospective clinical studies were reviewed against the cytologic examinations.
Results:
Based on the 189 thyroid nodule biopsies reviewed, 82.5% were benign compared with 17.5% malignant lesions. A solid nodule composition was noted in 35.2%, and had a higher risk for malignancy, compared with 7.7% of the mixed nodules. There was a 33.3% incidence of malignancy for solid nodules with PEF, compared with 35.8% of lesions lacking PEF. For mixed nodules, 6.2% nodules demonstrated PEF and 7.7% of nodules, without PEF, were malignant.
Conclusion:
In this cohort, solid nodules had a higher risk of malignancy than mixed nodules. PEF did not increase the risk of malignancy in either solid or mixed thyroid nodules, in these patients. These findings would suggest that existing guidelines may overestimate the value of PEF in scoring, as well as determining which thyroid nodules require biopsy.
Keywords
Thyroid nodules (TNs) are commonly observed in clinical practice, with a prevalence of up to 68% within the US population. 1 Currently, this presents as a significant clinical challenge, for clinicians as they attempt to detect thyroid cancer, while not providing overtreatment, avoiding the biopsy of benign nodules, and selecting only clinically significant thyroid lesions, for biopsy. 2 The incidence of thyroid cancer is only about 10% for a small number of nodules, 3 therefore numerous published guidelines, which classify categories of risk, are based on sonographic features.
The American College of Radiology Thyroid Imaging Reporting and Data System (ACR TI-RADS) has been increasingly adopted, as a standardized approach for assessing the risk of TNs. The ACR TI-RADS was created specifically to calculate risk stratification of TNs, based on sonographic imaging features. The data system is to be used for the detection of those thyroid cancers that are biologically significant. The recommendation is that a fine-needle aspiration (FNA) biopsy and sonographic follow-up be done for those highly suspicious TNs, with a diameter of 10 mm or greater. 2 These recommendations have been tested and approved for routine clinical use and have supported several research studies. The TI-RADS scores are based on the number of combinations of suspicious sonographic features and help to determine the risk of malignancy.2,4,5
TNs are now classified and assigned to one of the five ACR TI-RADS risk factor levels for purpose of study and identification. These risk factor levels are as follows: benign (TR1), not suspicious (TR2), mildly suspicious (TR3), moderately suspicious (TR4), and highly suspicious (TR5). 6 The scoring system is based on the composition of the nodules, their size, echogenicity, shape, margin, and the absence or presence of echogenic foci. There are four types of echogenic foci, according to their characteristics: comet-tail artifacts (>1 mm), macro-calcification, rim calcification, and punctate echogenic foci (PEF). 6 PEF are foci with no posterior acoustic shadows, a lack of small comet-tail artifacts, and are less than 1 mm in diameter 6 (see examples in Figures 1 and 2). The presence of PEF is a strong criterion within this scoring system and can add 3 points for upgrading any mixed (1 point) or solid nodule (2 points) to at least a TR4 category. 6 This upgrade based on sonographic features can lead to a biopsy recommendation for any nodule >1.4 cm. 6 The main rationale for this approach is the concern that PEF may represent psammoma bodies that are well circumscribed, laminated, and calcified structures, within a papillary thyroid carcinoma. 7 The prevalence of malignancy for hypoechoic nodules, with PEF and without comet-tail artifact is 21.9%, compared with 27.6% with small comet-tail artifacts. 7 Among malignant lesions, 84.5% of TNs, with PEF, were papillary carcinomas. 7 In a cohort study by Malhi et al, 7 they described the risk of thyroid malignancy as much lower (5.7%–6.1%), based on partially cystic lesions with echogenic foci. They concluded that all categories of PEF except those with large comet-tail artifacts could be associated with a high risk for cancer. 7 A study by Muradali et al 8 evaluated the histopathology of PEF in ovaries and found that these foci were found in tiny cysts, with no evidence of calcifications. These tiny ovarian cysts were associated with specular reflection, off the cyst wall, rather than psammomatous calcification. 8
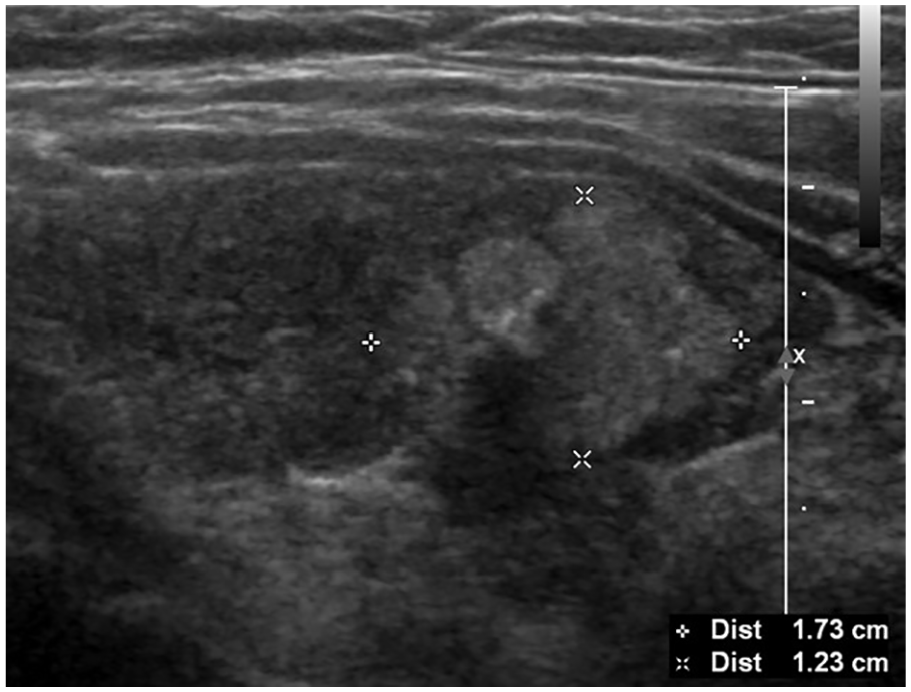
USG revealed 1.7 cm, solid, hyperechoic, thyroid nodule with punctate echogenic foci. The biopsy showed a benign thyroid nodule.
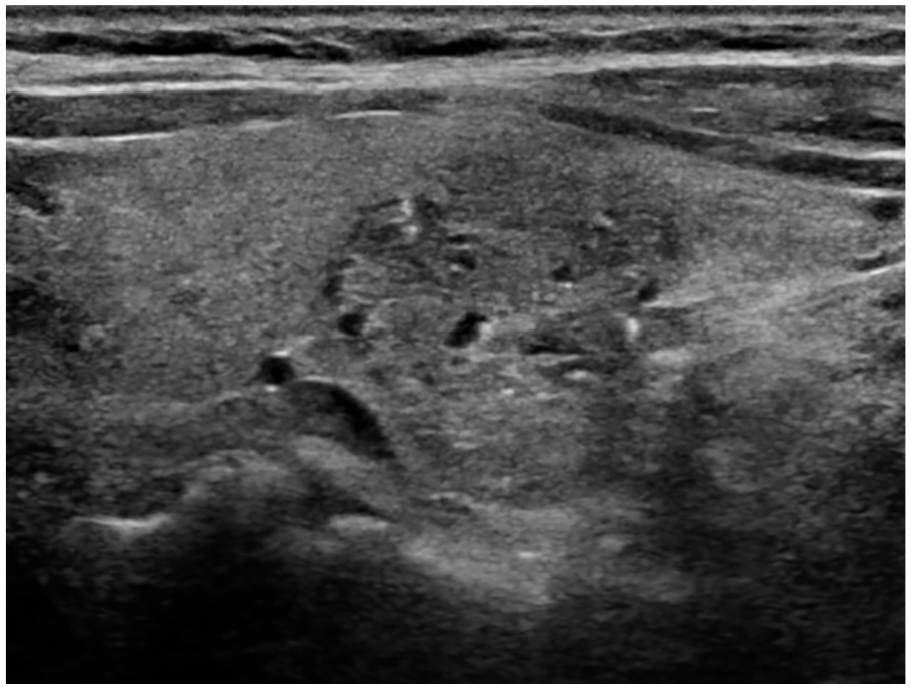
USG revealed 2.1 cm, mixed solid and cystic, hyperechoic, thyroid nodule with punctate echogenic foci. The biopsy showed a benign thyroid nodule.
A recent publication, using a multi-institutional database, found a low risk of malignancy in mixed nodules with PEF. 2 The authors suggested that decreasing the number of points assigned to PEF, in such nodules, could significantly decrease the number of unnecessary biopsies, for benign TNs. 2 The aim of the present study was to compare the prevalence of malignancy in mixed and in solid TNs, with and without PEF, compared with cytologic findings.
Materials and Methods
Thyroid sonograms and ultrasound-guided thyroid biopsies were performed, at a University of Iowa Hospital & Clinics for 105 patients, during July 2019 to June 2020. Thyroid imaging protocol and ultrasound-guided thyroid biopsy was completed using an Acuson Sequoia (Siemens Medical Solutions USA, Issaquah, WA) or an IU22 matrix (Philips Healthcare, Andover, MA) ultrasound equipment system. All the studies were read in a dedicated workstation using a Vue picture archiving and communication system (PACS; Carestream Health Inc, Rochester, NY). This study was staged in a single institution and required a retrospective review of 105 consecutive patients who underwent thyroid biopsy. The study was approved by the Institutional Review Board and written informed consent was waived.
Two radiologists with 18 and 17 years of experience interpreting thyroid sonograms, retrospectively, reviewed the lesion images for composition and presence of PEF, per ACR-TI-RADS guidelines. A consensus between the radiologists was needed for any discrepant interpretations. In cases where a consensus could not be achieved, a third radiologist with 15 years of experience interpreting thyroid sonography served as the tiebreaker. The radiologists were anonymized to the cytology results and any prior sonography interpretive reports. Only those nodules that were diagnosed as benign, malignant, or those that were resected, based on a definite cytologic diagnosis, were included in the study. All the nodules were classified for composition as follows: almost completely cystic, spongiform, mixed solid and cystic, and solid or almost completely solid (see examples in Figure 3). Nodules were also assessed for the presence of PEF, as indicated by the ACR TI-RADS guidelines. The prevalence of malignancy was evaluated for mixed and solid nodules, with and without PEF.
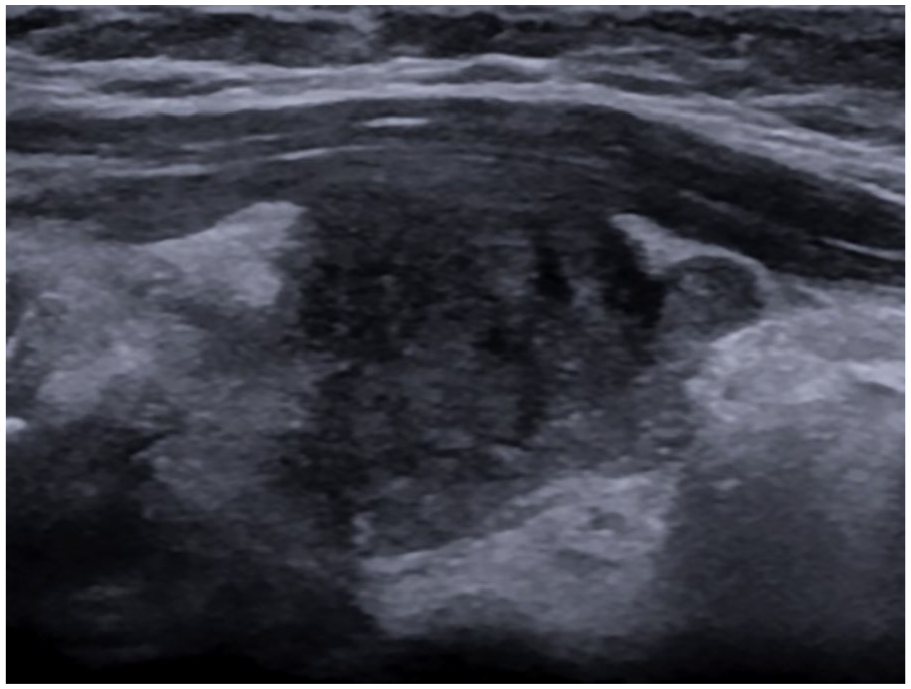
USG revealed 3.3 cm, solid, hypoechoic, thyroid nodule with punctate echogenic foci. The biopsy revealed papillary carcinoma.
Statistical Analysis
Descriptive statistics were gathered for the cohort and a Fisher exact test was used to compare the risk of malignancy between those four groups. Fisher’s exact test is a statistical significance test used in the analysis of contingency tables. The level of statistical significance was set at a P value <.05.
Results
This cohort study included a review of 105 patients’ records. The age distribution of this cohort was 15–94 years, with an average age of 46 years (±5 years). The cohort was composed of 68 females and 37 males. Of the total cohort, there were a total of 198 biopsied nodules of which, 189 had definite results and 9 were inconclusive. The inconclusive reporting resulted in those data being excluded from the study. Out of those, 189 definite reported nodules, 33 were malignant (17.5%) and 156 nodules were benign (82.5%) (see Table 1).
As Per American College of Radiology Thyroid Imaging Reporting and Data System Recommendations for Percentage of malignancy in Solid and Cystic Nodules Versus Solid Nodules With or Without Echogenic Foci.

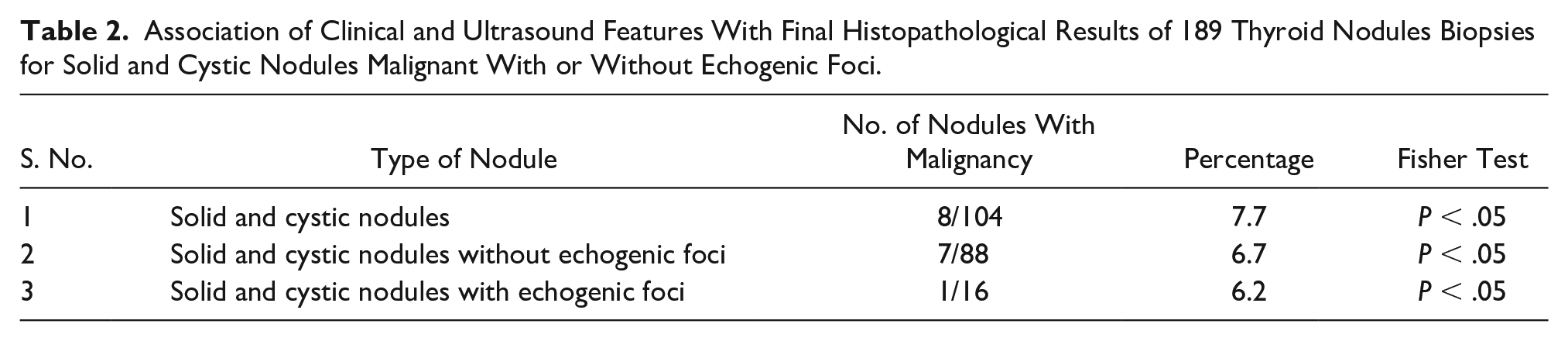
Based on the results of the 189 nodules, 104 nodules were characterized as mixed nodules. Out of those 104 mixed nodules, 8 nodules were malignant (7.7%). From the group of 104 mixed nodules, 88 nodules were without PEF and 7 nodules were malignant (7.9%). There was 1 out of 16 mixed nodules, with PEF, that was malignant (6.2%). Fisher’s exact test was not statistically significant P = 1 (see Table 2). In the cohort of 71 solid nodules, 25 were malignant (35.2%). From the group of 71 solid nodules, 53 nodules were without PEF. Of the solid nodules, without PEF, 19 out of 53 (35.8 %) were diagnosed as malignant. The solid nodules, with PEF, there were 6 out of 18 (33.3%) that were malignant. Again, Fisher’s exact test demonstrated no statistically significant differences between solid nodules with or without PEF (P = .60) (see Table 3). There were no malignancies found in the 14 nodules classified as almost completely cystic or spongiform nodules. The risk of malignancy was significantly higher for those 25 out of 71 solid nodules (35.2%). This was compared with 8 out of 104 (7.7%) mixed nodules (P < .00001). Mixed nodules versus solid nodules comparison are provided in Table 4.
Association of Clinical and Ultrasound Features With Final Histopathological Results of 189 Thyroid Nodules Biopsies for Solid and Cystic Nodules Malignant With or Without Echogenic Foci.
Association of Clinical and Ultrasound Features With Final Histopathological Results of 189 Thyroid Nodules Biopsies for Solid Nodules Malignant With or Without Echogenic Foci.

Association of Clinical and Ultrasound Features With Final Histopathological Results Mixed Nodules Versus Solid Nodules Malignant With or Without Echogenic Foci.

Discussion
Categorizing benign and malignant lesions based on undetermined cytology reports for TNs has been a significant challenge for clinicians. 2 With regard to thyroid lesions, a challenge exists for clinicians to appropriately balance the chance of causing harm, incurring significant investigatory costs, and to the risk of missing a malignancy, due to not conducting an ultrasound-guided biopsy.9,16 Those clinicians working in this discipline would welcome a modern diagnostic modality that improves the current uncertainty and ultimately saves the patient’s life. 10 The ACR TI-RADS has been proved to have several advantages over the other types of diagnostic guidelines. It is the standardized acquisition of sonographic features that mainly detects the suspicious malignancies attributed to PEF, compared with other nodule features. It also allows the risk stratification of suspicious TNs.12,13
The aim of this cohort study was to determine whether there was any statistically significant difference between mixed nodules, with or without PEF. Based on this cohort’s diagnostic data, the statistical values were not significant (P < .05). The solid nodules, in this cohort, had a significantly higher risk of malignancy compared with the mixed nodules. The present study results were comparable with those reported by Teefey et al. 2 It was indeed difficult to distinguish PEF from psammomatous calcifications, of the solid component, in tiny unresolved cyst, within mixed nodules. 3 This fact may have been one of the reasons that the present study results were not statistically significant. A sonographic pathologic study by Tahvildari et al 11 demonstrated that PEF could represent psammomatous, coarse, colloid, or dystrophic calcifications. None of these lesion features would be differentiated from each other with sonography, due to limited resolution afforded by current transducers. 14 Hoang et al 15 reported that only thyroid features with the substantial agreement were microcalcification and nodule size. 2 In a pathologic study of 360 thyroid carcinomas, Henrichsen et al 16 observed that 88.3% of carcinomas were solid and 9.2% of those were 6%–50% cystic; this is compared with their 2.5% which were more than 50% cystic. These results indicated that a very small percentage of thyroid cancers can be partially cystic. From all the predominant cystic carcinomas, Henrichsen et al 16 found that one or more suspicious features, such as solid components that consist of microcalcification, solid nodule dominancy, vascularity, and thick irregular wall, would permit an FNA. 16 Malhi et al 7 studied mixed nodules and they observed that the prevalence of thyroid cancer was minimal in mixed nodules. They studied 124 patients, and out of this cohort, lesions that were partially cystic were characterized as 50% cystic, others more than 50% solid, and the percentage of carcinomas was 6.1%, 5.7%, respectively. 7 They also supported that PEF in partially cystic nodules was a superior diagnostic sign for benign nodules. 8 Middleton et al 17 described that mixed nodules have an overall 4 % risk of malignancy (53/1331) compared with the solid nodules (200/1549), which had a risk of 12.9% malignancy. In addition to this, PEF increased the malignancy risk by35.3%, in solid nodules and an approximate risk of 10%, in mixed nodules. 17 Thus, this may seem to indicate that not only it is unusual for a thyroid carcinoma to have a partially cystic sonographic appearance, but the risk of malignancy, in partially cystic nodule, may be low. 17
The present study supports these findings that PEF did not boost the threat of malignancy in mixed nodules 8/104 (7.7%). Comparatively, the solid nodules significantly increased the risk (35.2%) of being thyroid cancer than mixed nodules (7.7%). The ACR TI-RADS were composed as a tool to assist a radiologist in classifying TNs. The scoring system uses simple points along with a risk stratification-based system. The present cohort study would seem to support recalibrating the TI-RADS scoring system with regard to PEF scoring points. Entertaining a recalibration of these points could assist in reducing thyroid biopsies and increase follow-up examinations, of benign nodules. It will eventually be supportive of detecting clinically important malignancy of TNs. However, as described in multiple studies, it can be difficult to determine the absence or presence of a few sonographic characteristics like PEF, which may increase unnecessary biopsies and the duration of follow-up examinations.
Limitations
This study has several limitations which are mainly due to the research designed used. In addition, the study was based on results from a single institution. Likewise, this study had a small sample size. As a retrospective study, it has an inherent weakness of technical limitations, given that only static sonograms and clips were used for the review.
Conclusion
In this cohort, solid nodules had a higher risk of malignancy than mixed nodules. PEF did not increase the risk of malignancy in either solid or mixed TNs, in these patients. These findings would suggest that existing guidelines may overestimate the value of PEF in scoring, as well as determining which TNs require biopsy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.