
Abstract
This research examines whether using a reference tool alters the monitoring of the mechanical index (MI) and thermal index (TI) during obstetric (OB) sonograms. A presurvey regarding users’ behavior patterns of monitoring MI/TI indices was emailed to sonographers who were registered in a clinical database affiliated with an accredited sonography program. The presurvey included a reference tool which respondents were asked to print and use when performing OB sonograms. A postsurvey was sent to the same respondents to determine if behavior patterns regarding MI/TI monitoring improved after using the reference tool. There were no significant changes in how often sonographers monitored MI/TI from the pre- to the postsurvey.
Keywords
During diagnostic medical sonography the interaction between the ultrasound pressure wave and the tissue being scanned can create biological effects, either in the form of heat absorption or mechanical effects such as cavitation and radiation forces. In mammals, heat has been shown to have deleterious effects, particularly on the developing fetus. 1 Temperature increases that exceed 4°C above core body temperature for longer than 5 minutes have created congenital anomalies in animal studies. 1 There are no documented ultrasound induced thermal biological effects for exposures that are under 2°C for 50 hours, nor are there documented bioeffects in the fetus when the thermal index value is less than 2.1-4
Temperature increases that could cause bioeffects to the fetus are theoretically possible in contemporary ultrasound systems and are related to examination time length, amount of bone that is present near sensitive tissues, output power/intensity, transducer frequency, focal length, absorption coefficient, beam cross-sectional area, scanning modes, frame rate, and dwell time.1,5,6 To reduce the risk of heat related biological effects, operators are encouraged to practice the principle of As Low As Reasonably Achievable (ALARA). While imaging, the operator can practice ALARA by reducing the dwell time, moving the transducer often, verifying the manufacturer default preset is appropriate for the procedure, using the freeze frame often, increasing the depth, adjusting the focal zones deeper than the area of interest, and staying educated on current bioeffects research.5-7
The potential bioeffects of ultrasound have prompted federal agencies to require intensity-output displays to be built into all ultrasound machines. The responsibility for monitoring energy levels falls to the operator of the ultrasound machine. The shift in FDA regulations requiring the operator performing the sonogram to monitor and adjust settings necessitates a comprehensive understanding of sonographic bioeffects and what ultrasound equipment settings affect it.
History of Acoustic Exposure Regulations
Prior to 1976, there were no acoustic exposure limits to diagnostic sonography equipment. 7 In 1976 the Food and Drug Administration (FDA) developed acoustic exposure limits that were specific to the type of sonographic procedure. The limits for examinations were set for fetal examinations at 94 mW/cm2, peripheral vascular at 720 mW/cm2, cardiac at 430 mW/cm2, and ophthalmic at 17 mW/cm2.5,7-9
In 1992 machine manufacturers and users requested a change to the 1976 limits to improve the diagnostic capabilities of ultrasound because it was believed that increasing the output power would have a medical benefit for patients.7,9 The FDA allowed the acoustic limits to increase to a maximum output of 720 mW/cm2 for all procedures except ophthalmic imaging, and the operator became responsible for monitoring the index levels for potential bioeffects during scanning and adjusting the equipment to decrease the index levels if needed. 6 The National Electrical Manufacturers Association (NEMA) developed the Standard for Real-Time Display of Thermal and Mechanical Acoustic Output Indices on Diagnostic Ultrasound Equipment, otherwise known as the output display standard (ODS).7,8 This standard incorporated the mechanical index (MI) to monitor for mechanical pressure effects of ultrasound on tissue, and the thermal index (TI) to monitor for the effects of heat on tissue. There were three classes of TI developed.5,8 Thermal index in soft tissue (TIS) is monitored during first trimester obstetric examinations because the ultrasound beam seldom interacts with bone. Bone increases the potential for heating in surrounding tissues due to increased attenuation rate and absorption, so thermal index in bone (TIB) is monitored after 10 weeks gestation as the fetal bone ossifies. Thermal index at cranial bone (TIC) assumes bone is superficial, and is monitored during cranial examinations. Both the MI and TI are displayed in increments of 0.2, and in general, when the indices exceed 1.0 during obstetric examinations, the operator is expected to follow the ALARA principle to minimize acoustic exposure.5,6,8
The American Institute of Ultrasound in Medicine (AIUM) created the necessary education for the operators with the booklet Medical Ultrasound Safety. 6 All machines manufactured after 1994 are packaged with the Medical Ultrasound Safety booklet for educating operators on the potential for bioeffects, the thoughtful use of performing sonographic examinations, and information on how to practice ALARA. 6 Although the booklet provides an overview of the biological effects of ultrasound and the rationale for implementing the MI/TI into the machine, it does not give detailed instructions on how MI/TI indices should be used while performing a sonogram. The AIUM frequently publishes statements regarding the most current knowledge of biological effects, and both the statement on heat and the statement on mammalian in-vivo biological effects inform operators that there are no known biological effects when the TI is kept below 2.0.1,2 However, the statements do little to provide guidance on how to use the TI in daily clinical practice.1,2
In 2009 the British Medical Ultrasound Society (BMUS) created guidelines for how to monitor the MI/TI during sonograms in a summarized and printable format. 10 For obstetric scanning, the BMUS recommends scanning below a TI of 0.7, and as the TI exceeds 0.7, they offer a suggested time limit for scanning at particular levels of TI. 10 It is unknown if sonographers have printed or used these guidelines while scanning. The AIUM, thus far, has not published similar guidelines concerning TI. Nelson et al suggest guidelines for obstetric sonograms using a TI of less than 0.5 if scanning for an extended length of time, a TI of up to 1.0 for less than 30 minutes, a scan time less than 60 seconds for TI greater than 2.5, and an MI less than 0.4 if gas bubbles are present or as low as possible in the absence of gas bubbles. 7
Lack of Operator Knowledge Regarding MI/TI Indices
Researchers have conducted studies on operator knowledge of bioeffects and have determined that most operators have a relatively low knowledge. In 2005, Maršál surveyed 199 physicians specializing in obstetrics and gynecology (OB/GYN), radiology, clinical physiology, or pediatric cardiology; sonographers; and midwives who routinely perform OB sonograms in Europe. 11 This survey assessed the knowledge of operators in regard to safety and bioeffects during OB sonograms. Only about a third of those surveyed were able to define what MI and TI meant. 11 In all, 22% stated they knew how to adjust acoustic output power and 28% stated they knew the location of the ODS on their equipment. 11 These results confirmed that many operators who are responsible for monitoring MI/TI lack basic knowledge about the indices or how to adjust the equipment to alter the index level.
In 2007, Sheiner et al surveyed 130 users prior to their attending a review course and two hospital grand rounds. 12 While 63% of participants were physicians, with the remaining being sonographers and midwives, there was not a difference in responses between the physician versus nonphysician groups. The survey assessed the operators’ knowledge of bioeffects in OB scanning and their attitudes toward the use of sonography in low-risk pregnancies. 12 Of the respondents, 22% were familiar with the term MI and 32% with TI; 12 20% could locate the ODS on their equipment. 12 The study concluded that operators have a low knowledge level of ultrasound bioeffects but those with a higher level of bioeffects knowledge believed that the number of sonograms performed during pregnancy should be limited.
In 2011, Houston et al surveyed 165 maternal-fetal medicine (MFM) fellows and postgraduate OB/GYN residents in regard to the safety of OB sonography and monitoring of the ODS. 13 They found knowledge was different between residents and fellows based on program, formal sonography training, and year of schooling among fellows. 13 In all, 37% of residents and 46% of fellows did not believe there were any limitations to ultrasound usage during OB sonograms, and 22% of fellows and 39% of residents did not believe there was a limit to Doppler usage during OB sonograms. 13 A total of 73% knew thermal mechanisms could be harmful to the fetus and 35% knew mechanical mechanisms could be harmful to the fetus, but only 13% reported that they could find or use the MI/TI. 13 This study provides evidence that ultrasound bioeffects may not be given as much emphasis in educational programs as they should.
In 2011, Bagley et al surveyed 212 sonographers to assess their knowledge of MI/TI and whether credentialing or length of experience influenced monitoring habits. 14 A characteristic of this study was that it was distributed to sonographers only, while other studies included various operators with only a small number of sonographers. Of respondents, 53% stated they never monitor MI/TI on the output display. 14 The survey determined that the relationship between sonographers’ knowledge of bioeffects, years of experience and whether the sonographer monitored MI/TI was not significant. 14 The high number of sonographers that never monitor MI/TI displays may signify that sonographers do not think ultrasound bioeffects are relevant enough to warrant monitoring.
These studies show poor operator knowledge of MI/TI, but evidence is limited on ways to improve the monitoring patterns of MI/TI. It is unknown if operators using a tool similar to the BMUS reference tool would increase MI/TI monitoring or bioeffect knowledge. The purpose of this study was to determine the monitoring behavior of sonographers and whether a printed reference tool would improve the behavior of monitoring index levels. A secondary question of whether users’ overall knowledge of bioeffects could be improved by using a reference tool was also assessed.
Methods
Two surveys (Appendices A and B), created electronically with a Qualtrics® Research Suite (Qualtrics, LLC, Provo, UT) and approved by the Institutional Review Board, were distributed to 103 sonographers registered in the Trajecsys Reporting System© (Trajecsys Corporation, Alexander, AR) affiliated with an accredited sonography program. The surveys were distributed via email to sonographers registered as performing OB sonograms routinely. Participation was optional and the sonographers did not receive an incentive for completing the surveys. Each survey was available to be completed for approximately 2 weeks.
The presurvey consisted of 13 questions regarding MI/TI. Seven of the survey questions pertained to sonographers’ monitoring habits of MI/TI during OB sonograms. Six of the survey questions pertained to sonographer’s knowledge of MI/TI during OB sonograms. The sonographers were asked to print the reference tool and to post it near the ultrasound machine for reference while performing OB sonograms (Appendix A). The reference tool was based the BMUS guidelines for monitoring the MI/TI during OB sonograms, and a reference to the guidelines was printed on the tool. 10
The postsurvey was emailed approximately 4 weeks after the presurvey, and consisted of 15 questions regarding MI/TI. Questions 1 through 12 of the postsurvey were the same as questions 2 through 13 of the presurvey. Two questions in the postsurvey were related to printing and use of the reference tool. The last question in the postsurvey asked for an explanation of why the respondents thought monitoring the MI/TI is important or unimportant during OB sonograms. Duplicating the questions on the postsurvey provided a comparison of the individual’s MI/TI monitoring habits and MI/TI knowledge level after using the reference tool.
Each pre- and postsurvey response was linked by email and Internet Protocol (IP) address when available or by unique IP address alone when an email match was not available. The data were deidentified prior to statistical analysis. Survey responses were analyzed using descriptive statistics computed for demographic and survey item responses before and after making the sonography tool available. McNemar’s test was used to analyze changes in categorical survey responses from the pre- to postsurvey. The rate with which respondents monitored MI/TI was assessed for normality and a change in rate of monitoring was compared using a paired t test or the signed rank test, as appropriate. The responses were analyzed using SAS® 9.2 statistical software (SAS Institute, Cary NC). A sample of 22 survey respondents was needed to detect a change in TI knowledge for sonograms done in the first trimester with 80% power and 5% type I error.
Results
A total 14 respondents completed the presurvey and 9 respondents completed the postsurvey. Seven out of 9 postsurvey responses were linked to the same respondents from the presurvey, allowing observation in the change of behavior or knowledge for 7 of the 14 original respondents. Due to low postsurvey responses, incomplete surveys were included if the pre- and postsurvey responses could be linked.
Of the nine respondents that completed the postsurvey, six respondents (67%) stated they printed the reference tool. Of the six respondents that printed the reference tool, three respondents (50%) stated they used it. One respondent that printed the tool stated he forgot to use it, and another stated he scans quickly during obstetric exams to reduce exposure time on any certain part of the fetus at any given time.
Operators were asked if they monitor MI/TI during OB sonograms, and 79% (n = 11) of presurvey respondents and 78% (n = 7) of postsurvey respondents stated they do not monitor MI/TI. Of the seven responses to this question that were linked in the pre- and postsurvey, one respondent who answered yes to monitoring in the presurvey also answered yes in the postsurvey. One respondent answered no to monitoring in the presurvey and answered yes to monitoring in the postsurvey. The remaining five responded no monitoring in both pre- and postsurvey. The change in reported behavior to this question from the pre- to the postsurvey was not statistically significant (P = .31).
The survey asked the respondent to type in a numerical value as to how often each monitored MI/TI during OB sonograms. Four respondents gave short answers instead of a number value. If the short answer indicated “no monitoring,” the value was counted as “zero.” When asked how often operators monitor MI/TI during OB sonograms, 9 of the 12 presurvey respondents (75%) stated they never monitor, and two (16.6%) stated they monitor at least five times per examination. Six of the eight postsurvey respondents (75%) stated they do not monitor, and one (12.5%) respondent stated he monitors five times per exam. There were six linked responses for this question, and the median (IQR) number of times monitoring during an examination in the presurvey was 0.0 times per exam. The median (IQR) number of times monitoring was 0 (0,1) per examination in the postsurvey; the change was not statistically significant (P = 1.0).
Respondents were given three options when asked what the recommended safe TI value was during OB sonograms. The options were derived from the BMUS printable reference tool recommendations, with 0.7 and below being the recommended TI. Of the seven linked responses for this question, five respondents (83.33%) answered correctly on both surveys (Figure 1). Respondents were also asked what TI should be displayed during first trimester and second trimester sonograms, TIS and TIB being the appropriate responses, respectively. Of the linked responses, two respondents (40%) correctly identified TIS as the appropriate display during first trimester sonograms. Two respondents (40%) did not know the correct TI for a first trimester sonogram on the presurvey, but correctly answered on the postsurvey. These differences were not statistically significant (P = .39). None of the respondents answered correctly in regard to the TI displayed during second trimester sonograms.
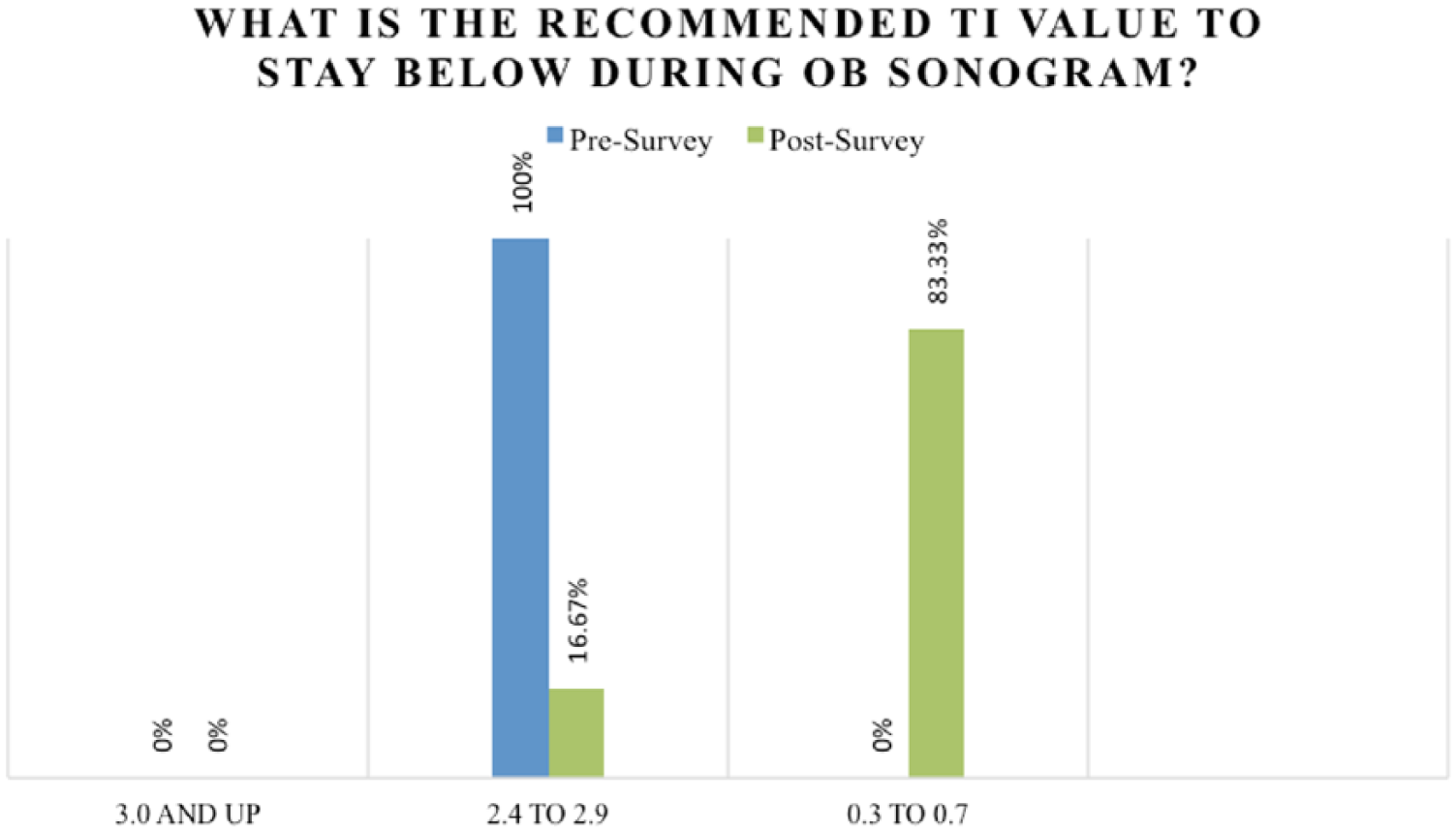
A comparison of pre- and postsurvey responses regarding the recommended limit for the thermal index (TI) during an obstetric sonogram.
All pre- and postsurvey respondents (100%) indicated they knew where the MI/TI (ODS) display was on their machines, but none limited scan time based on the displayed MI/TI. Four respondents (80%) stated they do not adjust settings based on the TI in both the pre- and postsurvey. One respondent in both the pre- and postsurvey stated he makes adjustments to settings based on TI. One respondent, who did not alter settings prior to taking the postsurvey, began altering settings according to postsurvey comments; the change was not statistically significant (P = 1.0).
When asked which index monitors for potential cavitation and for heating, four respondents (80%) correctly answered MI and TI, respectively, on both surveys. Respondents were given a variety of choices of settings and asked to choose all that can affect MI or TI (Figure 2). Thirteen respondents answered this question on the presurvey and nine answered on the postsurvey. Of the postsurvey responses, the greatest response increase was for the number of focal zones. This choice went up 35% with 8 of the 9 postsurvey respondents (89%) choosing it as affecting the MI/TI, while only 7 of the 13 presurvey respondents (54%) originally chose this as affecting MI/TI. Another large increase was frequency. Nine of the nine postsurvey and nine of the 13 presurvey respondents indicated that frequency affected MI/TI. It is difficult to say if the same nine were the respondents of the pre- and postsurvey but the results were not statistically significant.
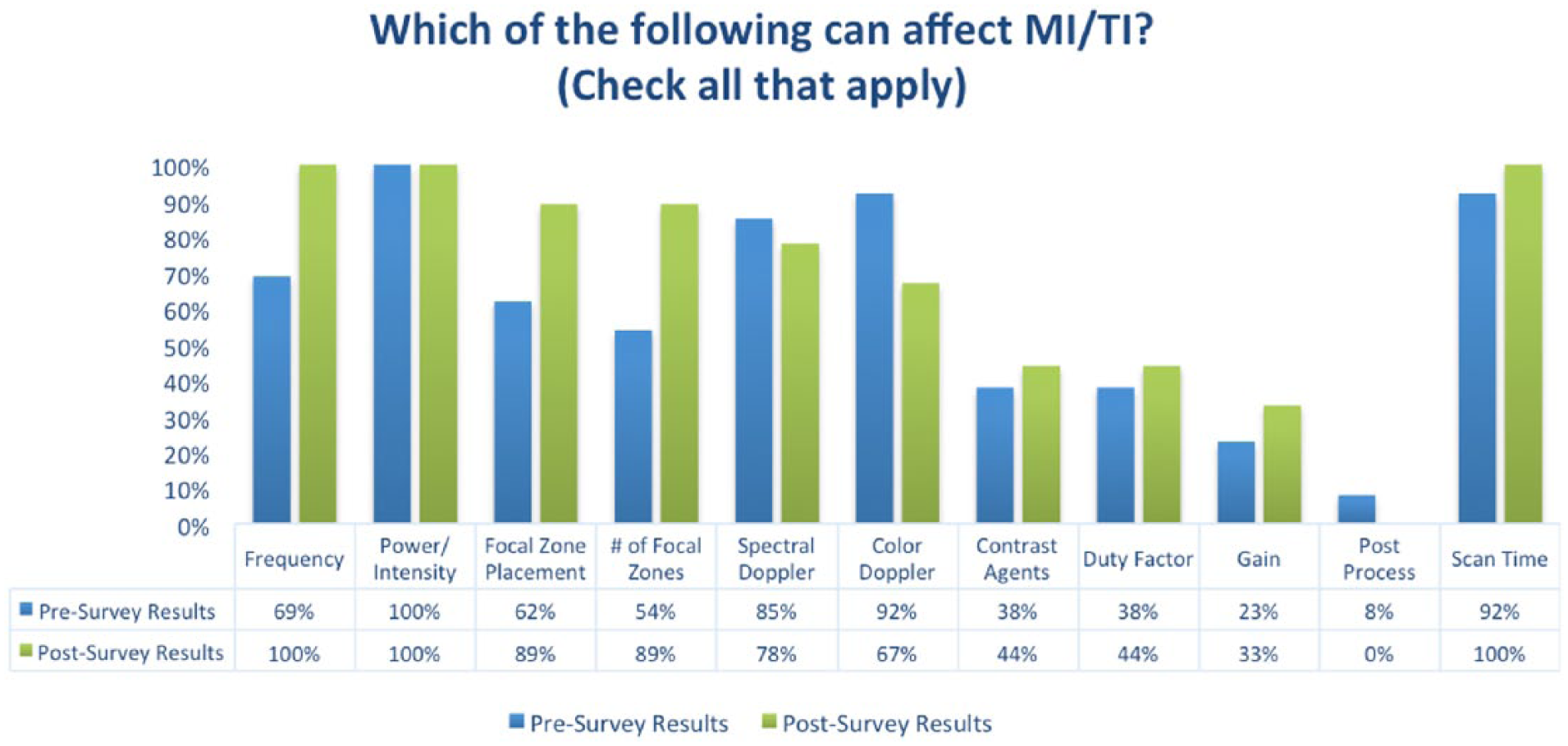
Comparison of pre- and postsurvey results regarding the instrument settings and scanning parameters that can affect the mechanical and thermal indices. MI, mechanical index; TI, thermal index.
Discussion
Because of the low overall response rate and minimal differences from pre to post responses, changes in operator tendency to monitor for bioeffects and alterations to knowledge level could not be detected. This study affirms the findings of other studies that operators have a lack of knowledge of the potential for bioeffects. Offering operators a reference tool to assist in monitoring for bioeffects did not prove to be beneficial.
Three of the nine (33%) postsurvey respondents did not print the tool. Of the six who printed the tool, only three respondents (50%) used it. Operators heavily relied on their equipment default settings to monitor MI/TI, stating for example “the machine is set not to exceed the limits.” Another respondent stated that “Quality Assurance monitored the MI/TI once a year,” another indication that operators do not understand the purpose of the MI/TI display or how to use it to implement ALARA. These comments further suggest that operators are currently not routinely implementing the ALARA principle into their scanning protocols.
Limitations to this study were the small sample size, the low response rate, and that the survey was distributed to sonographers affiliated with a single sonography program in one state, so generalizability is questioned. A larger sample size would be needed to note a true change in user behavior. After analyzing the data and taking the distribution of responses into consideration, it was concluded that this study would need 64 respondents to detect the observed change in TI knowledge for sonograms given in the first trimester with 80% power and 5% type I error.
The email address field was not required, therefore not all respondents entered email addresses, and not all data could be linked via email address. Several different IP addresses were used; therefore not all data could be linked via IP address. This finding could be due to sonographers having used several devices to complete the survey. The survey had no time limit once begun, allowing operators time to research answers to survey questions. In addition, there was a two-week gap between pre- and postsurveys, allowing operators time to research questions separate from the reference tool. It is possible that the small knowledge increase reflected in the pre- and postsurvey responses to the question pertaining to what can affect the MI/TI could be attributed to looking up the answers rather than using the printed reference tool (Figure 2).
There was a trend that monitoring MI/TI did slightly increase in the postsurvey. Of postsurvey respondents, 50% (n = 1) began adjusting settings based on the TI display, but it is unknown if the reference tool is solely responsible for this change in behavior. Furthermore, between the pre- to the postsurvey, there was a small, albeit insignificant, improvement in the answers concerning what system parameters affect MI/TI (Figure 2). Both trends suggest that respondents may have either used the tool or looked up information between the surveys, and these findings suggest that replication of the study on a larger scale may be worthwhile. Future researchers wishing to replicate this study may consider a different way to distribute a reference tool because delivering it to an email inbox does not appear to be a suitable way to motivate the intended audience to print and use it. If sonographers will not print a tool that is directly emailed to them, it seems unlikely they will purposely go to a society website and voluntarily print a tool such as the one available on the BMUS website. Handing out preprinted reference tools at conferences or via journal inserts may be a more suitable way to distribute a tool. Offering continuing education credits or a monetary incentive to respondents may boost participation.
Conclusion
It is the operator’s responsibility to monitor for potential bioeffects. The ODS is the mechanism by which operators monitor the MI and the TI to implement the principle of ALARA into scanning protocols. Operators in this research study exhibited little knowledge about the ODS, and these findings are similar to previous studies on the topic. Sonographic societies have attempted to educate operators with little success. This research provided a printable reference tool and invited respondents to print and use the tool while performing OB sonograms. There is no statistically significant evidence that using the reference tool changed behavior, although the sample size was small. There were some trends that may indicate the reference tool could be useful in helping to inform operators how to use the ODS when performing sonograms. This research study could be replicated with a larger sample size to determine if the use of a reference tool might prompt sonographers to monitor the ODS and in turn adjust equipment settings when indicated during OB sonograms.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.