
Abstract
The use of sonography has transformed prenatal screening, as it is predominantly noninvasive and considered safe. The most anticipated bioeffects of ultrasound include nonthermal effects such as cavitation and heat. Nonthermal or cavitational bioeffects are not likely in obstetric sonography because fetal bowel and lungs do not contain naturally occurring gas bodies required for cavitation to occur. The potential for bioeffects from ultrasound exposure is documented in in vitro and animal studies, and therefore, biological effects must be considered a possibility when tissues are exposed to high levels of ultrasound over an extended time.1–8
Hyperthermia, a known teratogen or an agent that causes embryonic malformation, may potentially occur when acoustic energy is absorbed by the fetus. 2 Some animal studies suggest that bioeffects may occur under certain circumstances related to elevated heat while other animal studies have demonstrated potentially nonthermally induced behavioral, learning, and social aberrations with both two-dimensional sonography and pulsed-wave Doppler exposure.3,4,6–8 Human studies do not demonstrate a correlation between ultrasound-induced temperature rise and fetal bioeffects, and a comprehensive review of the currently available literature does not demonstrate any correlations between adverse outcomes from in utero ultrasound exposure.1,6,9 Although animal studies are not directly applicable to humans, they suggest that future research is warranted.
In 1992, the Food and Drug Administration (FDA) allowed the increase in acoustic output capabilities for all examination types to a limit of 720 mW/cm2. This increase raised the potential allowed intensity in obstetric sonographic examinations almost eightfold; however, it does not mean that the system automatically operates at the raised intensity level.10,11 To monitor for biological effects, the Output Display Standard (ODS) was incorporated into ultrasound systems so the operator could observe the mechanical index (MI) and thermal index (TI).
The thermal index predicts heat production and is the most important index to observe during an obstetric sonogram.5,12 An increase in the TI should prompt the practitioners to consider the risks versus benefits at scanning at an elevated TI and attempt to alter the functions that can reduce it. Evaluating TI and taking action to reduce examination time and TI are required to implement the as low as reasonably achievable (ALARA) principle. Temperature rise is contingent on acoustic output, transducer, tissue types, beam dimensions, focal zone placement, scan mode, and dwell time.10,11 These parameters vary throughout the examination and from patient to patient. Currently, there is not a way to calculate actual in situ exposure of temperature rise in a human fetus, and TI is not directly associated with temperature increase. In addition, the developing embryo does not have the ability to dissipate heat via perfusion the way a postnatal subject would, and the location of the fetus within the uterus is a limiting factor to calculate an accurate TI. 13 The actual range of temperature increase that the fetus could experience is between 0.5°C and 2°C; therefore, the TI is the most accurate approximation of potential risk for a thermally induced ultrasound bioeffect.11,13,14 The goal of the ODS is to allow the operators to obtain diagnostic quality images while implementing the ALARA principle in scanning.
The TI has three categories: TIs for soft tissue, TIb for bone at focus, and TIc for transcranial bone at focus. 11 In first-trimester sonography, for a fetus under 10 weeks gestational age, the machine should be set to display TIs on the monitor (Figure 1), and for a fetus 10 weeks gestational age or greater, the TIb should be displayed because bone ossification has begun by this time (Figures 2 and 3). 11 The American Institute of Ultrasound in Medicine (AIUM) has recommended TIb value limits to be less than or equal to 0.7 for extended obstetric examinationss. 12 High acoustic energy levels are not always needed to obtain diagnostic quality images, and practitioners are obligated to observe and respond to the ODS throughout sonograms. When practitioners see an increase in the TI during an obstetric sonogram, they should adjust their scanning techniques so that risk to the patient is minimized. To guide operators and to educate practitioners on how to implement ALARA and observe the ODS, the AIUM published the book Medical Ultrasound Safety. 11 In addition, the AIUM publishes statements on the safety of the use of ultrasound in pregnancy and offers guidelines on the TI levels and associated time limits for scanning during pregnancy.12,15
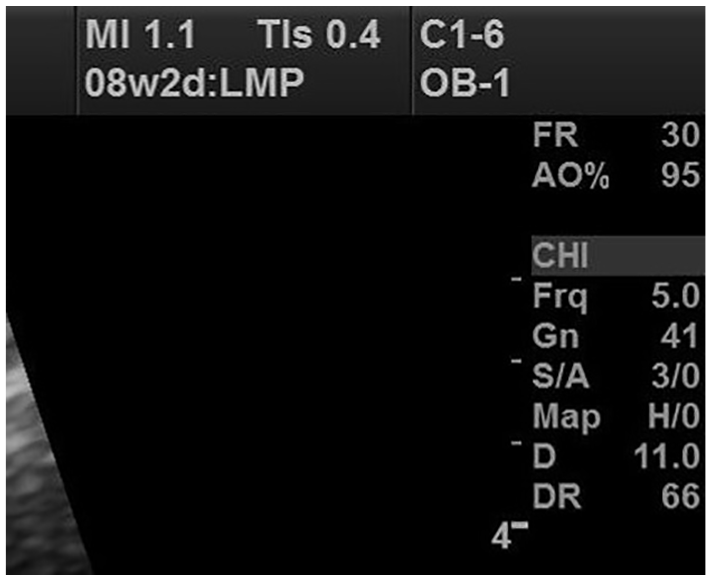
Proper use of TIs in the first trimester when the fetus is under 10 weeks.
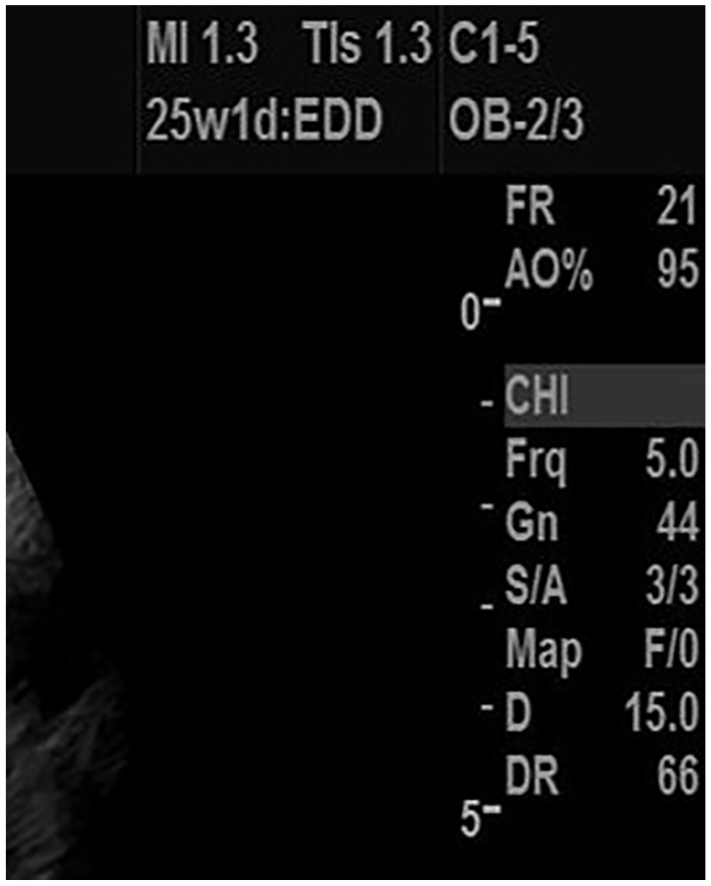
Improper use of TIs in the second trimester when the fetus is greater than 10 weeks.

A sonogram demonstrating the proper technique for measuring the nuchal translucency and includes the proper use of TIb for this gestational age.
Quality imaging, while maintaining low levels of TI in obstetric sonography, during the first-trimester nuchal translucency examination is achievable. 16 Practitioners appear not to follow through with ensuring that the appropriate TI is demonstrated on the images during the credentialing process. 17 The education and information on how to implement ALARA and monitor the MI and TI during sonography are available; however, the research indicates that most practitioners have low knowledge about potential bioeffects from acoustic output settings. It would appear that sonographers do not know how to adjust the equipment to keep the TI low during obstetric sonography.17–23
Because practitioner knowledge and compliance are low, the question then becomes, how can practitioners be informed of how to interpret the ODS and incorporate ALARA into their practices? A small study that included intensive bioeffect education through lectures, demonstrations, and email reminders over the course of six months demonstrated improvement in compliance with the TI 24 ; however, providing a pocket reference guide to operators did not show an improvement in their monitoring of the TI during obstetric sonography. 25 There are currently no large-scale interventional studies that include improving ALARA compliance in obstetric sonography as a study aim.
The Nuchal Translucency Credential
The nuchal translucency examination is a first-trimester screening sonogram that helps to identify the fetus’ risk for aneuploidy. To perform the examination, precise measurements of the nuchal translucency (Figure 3) must be taken between 11 weeks and 13 weeks 6 days’ gestation, and the results are correlated with specific laboratory blood tests. A credential is required in order for the individual performing the examination to prove that he or she has the skill and knowledge to measure the nuchal translucency correctly, as mismeasurement can alter the calculated risk for trisomies. 26
The Perinatal Quality Foundation (PQF) maintains a nuchal translucency quality review (NTQR) program that reviews images and awards an NT credential for providers who pass an image review. 26 Credentialing by the NTQR includes a mandatory submission of five images demonstrating the NT measurement from five different fetuses. 26 These images are scored relative to the nine mandatory criteria, and seven out of nine, or 80% or higher, is required to pass. 26 Practitioners who fail the first round of submissions will receive feedback on the criteria missed, and they are permitted to resubmit images. Individuals whose images meet the passing criteria will earn the NT credential.
When ALARA is not followed, through the incorrect TI displayed, no TI displayed, or the image displaying a level that is greater than or equal to 0.70, the image reviewer gives written feedback as to noncompliance with ALARA. This TI threshold was increased to the current less than or equal to 0.7 from TI less than or equal to 0.5 in 2017 to be consistent with the current AIUM guidelines. 12 Compliance with ALARA at the time of this study was not one of the pass-or-fail variables in the NTQR credentialing submission process.
The ALARA guidelines are not enforced by a credentialing body, and feedback given serves as recommendations of best practice. Passive attempts at education have failed at prompting the practitioners to implement ALARA during obstetric ultrasound examinations, but direct feedback on ALARA as a mechanism to prompt TI awareness or adherence to ALARA monitoring has yet to be studied in depth. This current study assessed if the written notification about ALARA improved the use of the correct TIb, as well as the level for practitioners who failed the first image submissions to NTQR and who also submitted images for a second attempt at earning the NT credential. The null hypothesis of this study was that there would be no change in ALARA behavior based on feedback about ALARA from comments on the NTQR image submissions.
Method
Researchers at a southwestern health sciences university conducted a retrospective, cross-sectional review of the Perinatal Quality Foundation Nuchal Translucency Quality Review Database with expedited institutional review board approval. The database was accessed and searched for images from practitioners who were identified as having failed their initial NT image submission between 2014 and 2017 and who received ALARA comments on their initial feedback from image reviewers. These comments were issued for each image in which ALARA was not followed. The feedback given that identified the images as not compliant with ALARA included the following comments: ODS was not demonstrated, a thermal index for BONE (TIb) should be used at this gestational age with an optimal ratio of <0.5, TIB should not exceed 0.7, TIs was used, or TIb was too high. For each batch submission from a practitioner, the highest value of TIb or TIs (if it was the only index displayed) on any of the five submitted images for each subject was recorded. A mean TIb for all practitioners was calculated for those who submitted images with a TIb recorded.
The resubmissions of the same practitioners were evaluated to document if changes to ALARA were made in the second submission. On the second submissions for each practitioner, if the TIb was displayed, the highest TIb value on any image was recorded. A mean TIb was calculated for the second submissions. In this study, second-round TIb values less than 0.7 were considered in compliance, but the NTQR recommendations at the time were for the TIb to be less than 0.5. Registry status by the American Registry of Diagnostic Medical Sonographers (RDMS) was assessed; however, specialty credentials in obstetrics/gynecology or practitioner type (sonographer/physician) could not be determined in the review.
Descriptive statistics and proportions among each categorical variable were calculated along with 95% confidence intervals (CIs). Chi-square tests determined whether the proportion of submissions that addressed ALARA differed among submissions that passed second submission and those that did not pass. In addition, a chi-square test was used to determine whether the proportion of submission addressing ALARA concerns differed among those with RDMS certification or not. A paired t test determined if TIb values were different between first and second submissions. In addition, independent Student t tests determined differences in TIb among those submissions addressing ALARA or not, as well as individuals with or without RDMS certification. Assuming that 35% of the ALARA recommendations would be addressed upon resubmission, a sample size of 85 submissions was required to detect a difference from 50%. A sample size of 85 was adequate to achieve 80% power assuming a 5% chance of a type I error. All statistical tests were computed using SAS 9.4 (SAS Institute, Cary, North Carolina) and assumed a 5% chance of a type I error.
Results
There were 295 first-round submissions with ALARA comments, and 206 of these practitioners submitted a second time, resulting in a final sample size of 206 practitioners with two submissions for the NT credential. Seventeen percent (n = 35; 95% CI, 11.8–22.2) of all resubmissions addressed ALARA concerns, while 83% (n = 171; 95% CI, 77.83–88.12) did not (Table 1). Of all second submissions, 60.7% (n = 125; 95% CI, 54.0–67.4) passed; however, only 18.4% (n = 23; 95% CI, 11.6–25.2) of those who passed the second submission addressed ALARA. The proportion who addressed ALARA was not different among those who passed the second submission compared to those who did not pass the second submission (P = .50; Table 1).
Frequency and Percent of Those Who Addressed ALARA Among Practitioners Who Passed or Failed the Second Image Submission (P = .50).
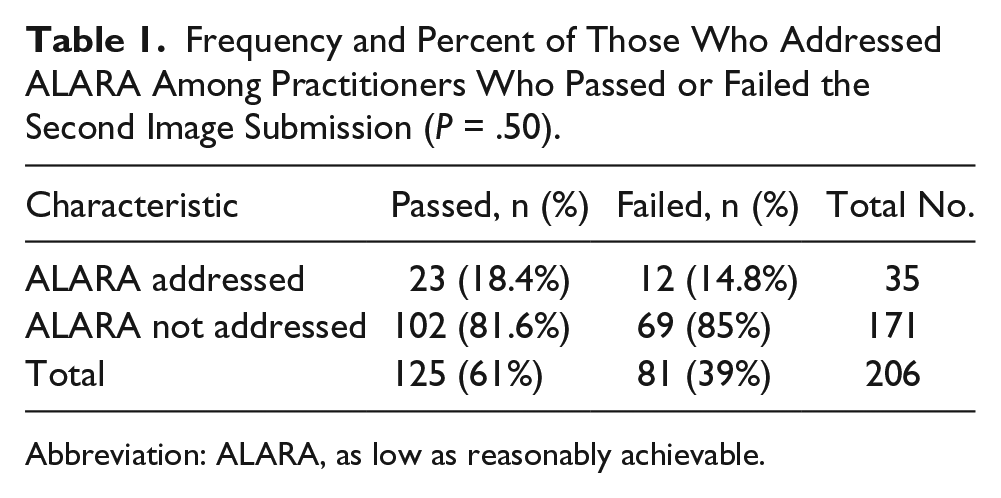
Abbreviation: ALARA, as low as reasonably achievable.
In the first submissions, 20.4% (n = 42; 95% CI, 14.8–25.9) reported TIb values, and in the second submission, 29.1% (n = 60; 95% CI, 22.9–35.4) reported TIb values (Table 2). Fifty-two percent (n = 106; 95% CI, 44.54–58.33) of operators used TIs instead of TIb in the first submission images. In the second submission, 38.8% (n = 80; 95% CI, 32.12–45.54) used TIs incorrectly a second time (Table 2). Of the operators who did not display an ODS on the images, 28.2% (n = 58; 95% CI, 21.06–34.34) reported no ODS in the first submission and 32.0% (n = 66; 95% CI, 25.61–38.46) in the second submission (Table 2).
Output Display Standard Reporting on First and Second Image Submissions.
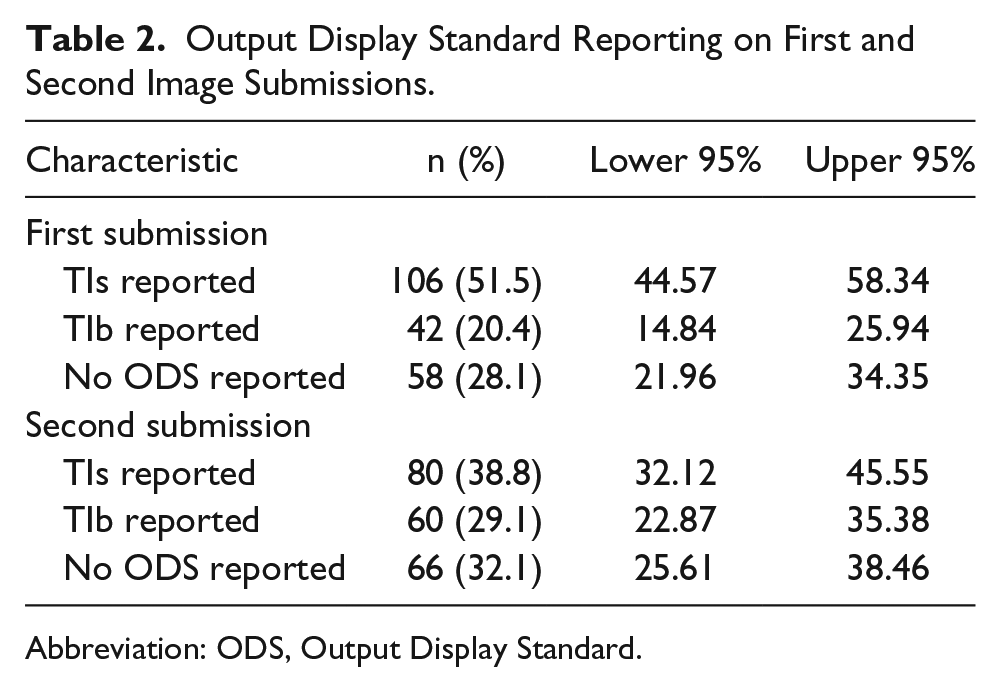
Abbreviation: ODS, Output Display Standard.
The proportion who addressed ALARA was not different among those who did and did not have the RDMS credential (P = .09; Table 3). For operators with the RDMS credential, only 19.9% (n = 29) addressed ALARA and 80% (n = 117) did not address ALARA following comments after first submission. In those without the RDMS credential, only 10% (n = 6) addressed ALARA and 90% (n = 54) did not address ALARA (Table 3).
Numbers of RDMS Certified Compared to Non-RDMS Certified Practitioners Who Addressed ALARA or Not on the Second Submission (P = .09).
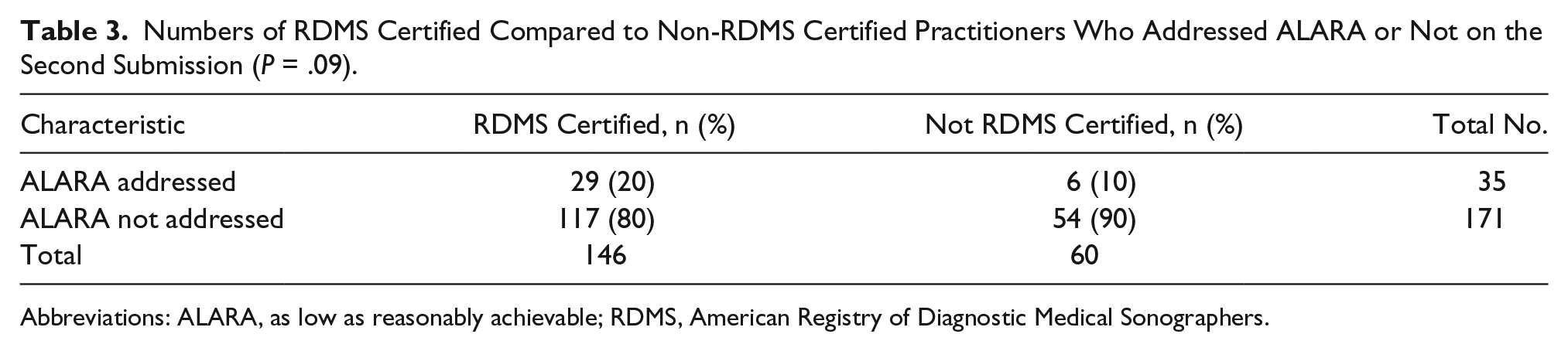
Abbreviations: ALARA, as low as reasonably achievable; RDMS, American Registry of Diagnostic Medical Sonographers.
Among those who submitted TIb values on both first and second submissions (n = 27), the mean TIb values on the second submission were 0.20 (95% CI, 0.02–0.37) lower compared to the first submission (P = .03; Table 4). Second submission mean TIb values were 0.68 (95% CI, 0.51–0.85) lower among those submissions with ALARA concerns addressed compared to those not addressing ALARA concerns (Table 5; P < .001). There was no difference in second submission mean TIb values among the proportion that passed the second submission and the proportion that did not (P = .2). There was no difference in mean TIb values among those with and without the RDMS credential (P = .8).
TIb Values on First and Second Submissions Among Practitioners Who Addressed ALARA (P = .02).

Abbreviation: TIb, thermal index for BONE.
Second Submission TIb Values With ALARA Addressed or Not Addressed (P < .001).

Abbreviations: ALARA, as low as reasonably achievable; CI, confidence interval, TIb, thermal index for BONE.
Discussion
The results of this research study were consistent with the null hypothesis of this study that practitioners will not adhere to the ALARA principle when given specific feedback. The majority of practitioners in this study did not adhere to ALARA but were able to earn the NT credential. The reasons why they did not adhere to ALARA are unknown, but it could be because ALARA is not among the nine required criteria for passing the image review. These findings contribute further to the body of research regarding noncompliance with ALARA and further support the concept that interventions to prompt practitioners to adhere to ALARA voluntarily are not effective.
Most practitioners did not use the correct TI in both the first and second submissions, nor did they consistently include the ODS on their images. These findings raise concern that practitioners may not know which TI is appropriate for this gestational age, may not know the difference or significance of using and displaying the correct TI, or may not consider it important to display the TI. In addition, they may not know how to adjust their machines in ways that will lower the TI. Some images had no ODS displayed at all. It is unknown if the machine did not have an ODS or if it was removed by the practitioner before the image was submitted to the NTQR for review; therefore, it is unknown whether these operators were monitoring the ODS. Practitioners may not understand how to implement the TI and choose not to display it on the images they submit for NT credentialing. This finding demonstrates that there is a lack of knowledge about the ODS or that practitioners do not consider it important. The finding is consistent with previous research.15–19
Practitioners who used TIb in the first submissions were more likely to use TIb again in their second submissions. Furthermore, the practitioners who used TIb in both first and second submissions were also more likely to lower their TIb values in their second submission based on first-submission ALARA comments. Practitioners who use the correct TIb setting may have a baseline level of awareness of the ODS, and for those individuals, feedback on ALARA may be effective. Further research is needed to determine if certain practitioners are more amenable to education and feedback.
There was variability in the reviewer comments. Some reviewers used stronger language that implied that ALARA was important to earn the credential, while others may have used language that the practitioners may have considered the comment as only a suggestion. It is possible that practitioners who received more in-depth or detailed comments from NTQR reviewers were more likely to adjust acoustic output levels upon resubmission. This study did not attempt to classify the types of comments received and did not account for reviewer’s depth or level of explanation in the ALARA comments, which is a weakness of this study.
This study did not compare if those who failed the first image submission were more likely to have ALARA comments, as everyone in this study had failed the first submission and had ALARA comments. In addition, this study did not look at the number of criteria that failed for each image and compare to images with ALARA comments to determine if receiving ALARA comments was correlated to receiving more failed criteria. Future studies could evaluate if any specific criteria for failure correlate to receiving ALARA comments.
This study looked at only one organization that provides a nuchal translucency credential. The PQF organization was selected based on its ALARA recommendations, for its written mentoring for including the TIb on nuchal translucency images, and because this organization previously chose to examine the issue of ALARA compliance among its practitioners. The NTQR database contains a representative sample of practitioners in the United States. This study did not query the databases of other NT credentialing organizations, and it cannot make claims about whether their clients follow any ALARA recommendations they might have. More important, the purpose of this study is not to imply that organizations that provide an NT credential should have ALARA standards but rather to illustrate that if organizations (of any kind) want their practitioners to follow ALARA, there should be mandatory credentialing or accreditation criteria. Otherwise, based on this research and previous research, it appears unlikely that practitioners will voluntarily follow ALARA.
A survey to the practitioners that asks them why they did not adjust the indices, did not display the ODS, or used the incorrect TI setting could be insightful. It is possible that the participants did not pay attention or feel compelled to adjust ALARA since it is not required of them to pass for NT certification. Information learned from these types of studies could be useful in guiding the NTQR in the next steps of deciding if ALARA should become a pass/fail variable for earning the NT credential.
Conclusion
Practitioners who use ultrasound equipment are responsible for monitoring the ODS and adjusting the imaging controls to keep the TIb below 0.7 during routine obstetric sonography. This information is given to providers in the Medical Ultrasound Safety Book that is included with all new ultrasound systems and is available for purchase. The AIUM publishes guidelines for how to observe the TI during obstetric sonograms. In addition, many organizations that serve the sonography profession provide educational activities about ALARA for their members. Thus, there is opportunity for practitioners to gain instruction on how to implement ALARA and observe the TI. The practitioners in this study had inconsistent use of correct TI throughout NT examination image submissions. A written comment upon first submission feedback was not enough to prompt change in ALARA monitoring upon resubmission for NTQR credentialing. Those seeking an NT credential who do not follow ALARA are not likely to follow it even after receiving a comment about incorrect use. Thus, ALARA may need to be included in the pass-fail criteria for receiving a NT credential. Further research is needed on why practitioners do not pay attention to ALARA and to determine what educational interventions will improve practitioner compliance with ALARA.
Footnotes
Acknowledgements
The authors extend special appreciation to the Perinatal Quality Foundation for access to its data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.