
Abstract
Introduction:
Indonesia reduced the prevalence of stunting from 37.6% in 2013 to 21.6% in 2022; however, it remains above the 2024 target of 14%. In Central Java, the prevalence is 20.7%, underscoring the need for targeted interventions. This study examined the determinants of stunting in children in Central Java.
Methods:
A matched case-control study was conducted in June-July 2024 across selected districts. A total of 138 children aged 6 to 59 months were included in the study. Data were collected using structured questionnaires and medical records. Chi-square test and logistic regression were used for bivariate and multivariate analyses.
Results:
Stunted children more often had pulmonary infections (87.5%), low birth weight (84.6%), and a history of hospitalization (53.5%). Maternal postpartum depression (82.4%) and low education levels were also significant. Hospitalization (OR 5.985, P < .01) and postpartum depression (OR 5.155, P < .05) remained key predictors.
Conclusion:
Integrated strategies addressing healthcare, maternal mental health, and nutrition are essential for reducing stunting.
Background
Sustainable development goal point 2.2 aims to end all forms of malnutrition, related to stunting and wasting in children under 5 years of age, and fulfill the nutritional needs of adolescent girls, pregnant and lactating women, and the elderly. 1 Stunting in children under 5 years of age is a nutritional problem of global concern, which describes a chronic condition due to malnutrition early in the growth period and affects the physical and cognitive development of children as they grow into adulthood.
The global prevalence of stunting in 2022 is 22.3% or 148.1 million stunted toddlers in the world, and more than half of the stunted toddlers come from Asia (76.6 million). 2 The prevalence of stunting in Indonesia has successfully decreased from 37.6% in 2013 to 21.6% in 2022. However, the prevalence of stunting decreased by only 0.1% according to the 2023 Indonesian Health Survey (IHS), which was 21.5%. This achievement has met the RPJMN 2020-2024 target, where the stunting prevalence target is 14% in 2024. 3
The HIS 2023 results found that 1 in 5 children under the age of 0 to 59 months in Indonesia are stunted. Data by province show a large gap between regions, with the lowest prevalence of stunting at 7.2% and the highest at 37.9%. Central Java Province has a stunting prevalence of 20.7%. 4 This is a 0.1% decrease from the SSGI 2022 (Indonesian Nutrition Status Survey) result of 20.8%. However, of the 35 districts/cities in Central Java Province, only Demak District has a stunting prevalence of less than 14%, which is 9.5% compared to other districts/cities that are still above 14%. 4 Health determinants are factors that have a significant effect, either positive or negative, on health. There are many dimensions that can be used to describe determinants, such as a person’s characteristics and behavior, the physical environment, and the socioeconomic environment. 6
The determinants of stunting include maternal and child health factors and household and environmental conditions. Maternal health during pregnancy, place of delivery, breastfeeding practices, infectious diseases, and child feeding patterns have all been shown to play important roles.5 -7 However, these determinants do not operate independently. In low- and middle-income settings, inadequate access to health services, limited household income, and cultural feeding practices often exacerbate these risks. For example, mothers with limited education or those experiencing postpartum depression may face difficulties in providing responsive care and adequate nutrition to their infants. Similarly, children with repeated infections or hospitalizations are more vulnerable when living in households with poor sanitation, food insecurity, or limited social support.8 -10 These challenges demonstrate how biological risks are amplified by socioeconomic and cultural contexts, making stunting a complex problem that requires multisectoral solutions.
Therefore, this study aimed to determine the determinants of stunting from maternal, infant, behavioral, and sociocultural factors and environmental factors, referring to hospital-based data on cases of stunted toddlers, to provide recommendations for future stunting prevention in Central Java Province.
Methods
Study Design and Settings
A matched case-control study was conducted in the Central Java province from June to July 2024. This province encompasses 3 distinct terrains: coastal regions, plateaus, and lowland areas. Three districts were selected to represent the 3 areas based on an increase in cases of over 5%, according to the 2023 SSGI survey data (Figure 1).
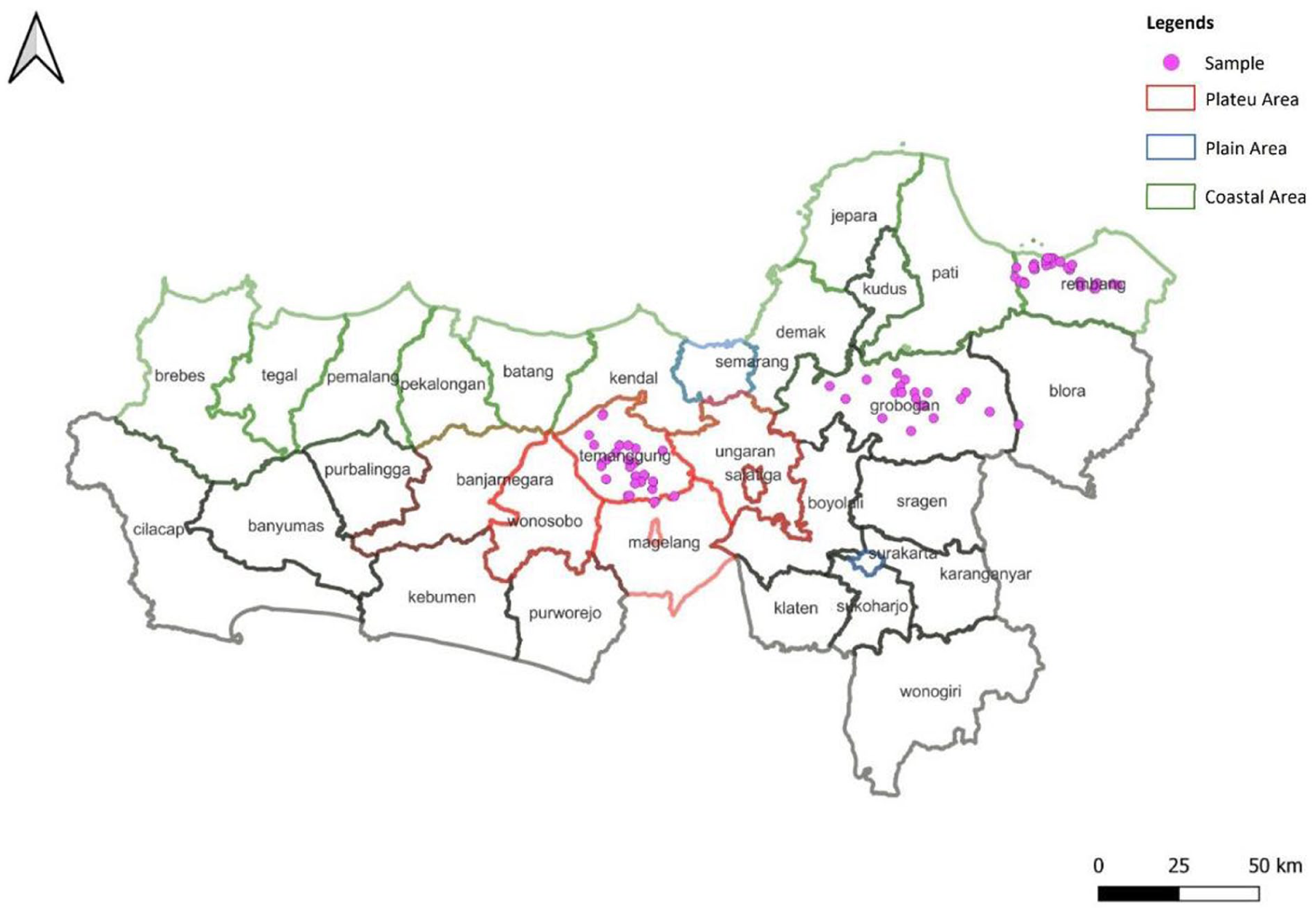
Map of Central Java Province showing districts chosen for the study.
Study Participants
Stunting was defined according to the World Health Organization (WHO) Child Growth Standards as a height-for-age Z-score (HAZ) of less than −2 standard deviations (SD) below the median of the reference population. Children with HAZ ≥ –2 SD were classified as non-stunted. For this study, cases were children aged 6 to 59 months identified in hospital records as stunted, while controls were age-matched children without a history of stunting or nutritional problems. In the hospital setting, stunting was diagnosed by pediatricians using the WHO Child Growth Standards.
Sample Size Calculation
The necessary sample size was determined using the EpiR sample size calculator for matched case-control studies (available at https://shiny.vet.unimelb.edu.au/epi/sample.size.mccs/) with a 95% confidence interval, an effect size of 6, a risk factor exposure rate of 3.3% in the control group, and a power of 80%. 11 A total of 69 cases and 69 controls were collected, with 23 cases and 23 controls from each district. The risk of stunting was assessed based on the child’s and mother’s factors.
Data Collection Tools
The questionnaire was developed by adapting the questionnaire of the “Survei Kesehatan Indonesia” from the Ministry of Health of Indonesia and the Edinburgh Postnatal Depression Scale. 12 No clinical data were collected during the study. A structured questionnaire was employed to gather information from the mothers of the selected children regarding child factors (gender, infectious disease history, family history of TB, mother’s gestational age at birth, birth weight, birth length, and hospitalization history) and mother’s factors (occupation, education, average income, health insurance ownership, early breastfeeding initiation, and postpartum depression). Gender was categorized as male (coded as 1) or female (coded as 2). The history of infectious diseases and family history of TB were assessed through recall questions, with responses categorized as yes (coded as 1) or no (coded as 2). Mother’s gestational age at birth was categorized as 37 weeks or less (coded as 1) and more than 37 weeks (coded as 2); birth weight was categorized as low birth weight (coded as 1) if the weight was less than 2500 g, and normal (coded as 2) if the weight was equal to or more than 2500 g. Birth length was categorized as less than 48 cm (coded as 1) or ≥48 cm (coded as 2). Hospitalization history was coded as 1 (yes) and 2 (no). Maternal occupation was categorized as employed (coded as 1) if the mother worked outside the home and housewife (coded as 2) if she had no other employment. Maternal education was classified as low (coded as 1) if the mother did not finish high school and higher (coded as 2) if she completed university. Average household income was categorized based on information from previous studies. 13 Postpartum depression was categorized as not good (coded 1) if the score was 13 or more, and good if the score was below 13.
Data Collection
This study focused on children aged 6 to 59 months, with cases defined as stunted children identified through medical records at district hospitals. Four trained enumerators collected data by visiting households and interviewing mothers using questionnaires. To ensure accurate information regarding the children’s birth history, including birth length and weight, the enumerators referred to the children’s health records known as “Kartu Menuju Sehat” (KMS). A matched case-control design was applied, with each case paired to a control based on age and residential area to control for differences in growth potential related to the developmental stage and local environment. Additional matching was ensured by selecting controls from nearby households, thereby increasing comparability in terms of socioeconomic and cultural contexts. This design was intended to reduce confounding and strengthen internal validity while maintaining feasibility in a field setting.
Data Analysis
The analysis was conducted at 2 levels: initially, a bivariate analysis was performed to identify variations based on explanatory variables. A chi-square test was used to assess the presence of significant relationships between stunting and specific risk factors. Subsequently, the variables identified in the bivariate analysis with P < .25 were incorporated into a multivariate analysis. A logistic regression model was employed to explore the independent relationships between the explanatory variables and the binary outcome (stunting). This approach was chosen to allow the inclusion of all relevant covariates in the multivariate model, following the analytic strategy applied in comparable epidemiological studies. 14 Statistical analysis was performed using IBM SPSS 26, and the goodness of fit for the logistic regression model was evaluated using the Hosmer and Lemeshow chi-square test. Nagelkerke’s R2 coefficient of determination was used to evaluate the predictive ability of the model.
Ethical Approval and Informed Consent
This study was conducted in accordance with the guidelines of the Declaration of Helsinki, and all procedures involving human patients were approved by the Ethics Committee of Universitas Dian Nuswantoro (No.001482/UNIVERSITAS DIAN NUSWANTORO/2024). Written informed consent was obtained from all the participants.
Results
Child and Mother Characteristic
The study included a sample of 138 mothers with children aged 6 to 59 months, comprising 69 children with stunting and 69 without stunting. As shown in Table 1, a higher proportion of males (55.1%) was noted in the stunted group than in the non-stunted group (31%). The prevalence of infectious diseases in the stunted group was significant, with pulmonary infections occurring in 87.5% of the cases. Additionally, over half of these children (71.4%) had a family member with a history of tuberculosis. Notably, most stunted children were classified as having low birth weight (84.6%) and had a record of hospitalization (53.5%). Most mothers of stunted children were housewives (50.9%), had low education (50.4%), and low income (55.4%). More than half of the mothers of the stunted children had health insurance (58.1%) and reported poor mental health during the postpartum period (82.4%).
Socio-Demographic and Economic Characteristic of Study Population and Factors Associated With Stunting: Bivariate.

P < .05. **P < .01.
The Correlation Between Child’s Factors, Mother’s Factors and Stunting
Based on child factors, children with a history of pulmonary infections were significantly associated with higher odds of being stunted compared to their non-stunted peers (P = .031, 95% CI: 0.918-64.177; OR: 7.677). Additionally, stunting was more frequently observed among children born with low birth weights than among those with normal birth weights (P = .020, 95% CI: 1.352-29.847, OR: 1.930). Children who had been hospitalized were more likely to be stunted, with odds 7.7 times greater than those without a history of hospitalization (P < .001, 95% CI: 2.757-21.726, OR: 7.740). Furthermore, regarding maternal factors, mothers who experienced postpartum depression were significantly more likely to have stunted children (P = .010, 95% CI: 1.530-20.492, OR: 5.6).
Table 2 shows the outcomes of the multivariate model analysis with adjusted odds ratios (OR) and 95% confidence intervals (CI). Notably, a history of hospitalization was strongly associated with stunting, with OR of 5.985 (95% CI: 2.046-17.509) and 5.113 (95% CI: 1.710-15.292) in Models 1 and 3, respectively, indicating higher odds of stunting among children with prior hospitalization. Although the relatively small sample size and wide confidence intervals suggest caution in interpretation, these findings offer important indications and highlight areas that require further investigation in larger studies. In contrast, health insurance ownership was associated with lower odds of stunting, particularly in Model 2 (OR 0.443, 95% CI: 0.214-0.916). This association persisted in Model 3 (OR 0.626, 95% CI: 0.288-1.360), although it was not statistically significant.
Result of Multivariate Model Analysis.

Model 1 was adjusted for child’s factors.
Model 2 was adjusted for mother’s factors.
Model 3 was adjusted for child’s factors and mother’s factors.
P < .05. **P < .01.
Additionally, postpartum depression was a significant correlate, with Model 2 showing an OR of 5.155 (95% CI: 1.387-19.165), suggesting an association with a higher odds of stunting. Other variables, such as pulmonary infection history, birth weight, and birth length, also showed associations, but their wide confidence intervals and non-significant p-values indicate uncertainty about the strength of these associations.
The overall model fit statistics, including chi-square values and Hosmer–Lemeshow test p-values, suggest that while these models provide insight into the factors associated with stunting, they explain only a modest proportion of the variance, as reflected by the Nagelkerke R² values (0.126-0.258).
Discussion
Stunting in early childhood is a critical public health issue, reflecting nutritional deficiencies and health challenges that have long-term effects on physical and cognitive development. 15 This study highlights the high prevalence of stunting among children aged 6 to 59 months and identifies several important factors contributing to it. We observed that stunted growth was more common among male children, although the difference was not statistically significant. Biological differences in growth patterns and immune responses may make boys more vulnerable to undernutrition and infection. However, these biological predispositions are further shaped by household dynamics, social norms, and caregiving practices, reinforcing inequalities in child health and well-being.16,17
We also observed a strong association between stunting, pulmonary infections, and low birth weight, underscoring the complex relationship between infection and growth. Respiratory infections increase metabolic demands and reduce nutrient availability, thereby worsening nutritional status.18,19 Low birth weight compounds this risk by impairing immune development and restricting growth trajectories.20,21 Together, these conditions create a cycle of recurrent infections and chronic undernutrition, ultimately increasing the likelihood of stunted growth and adverse health outcomes in children.
Importantly, this study provides new insight into the strong association between hospitalization history and stunted children. Frequent hospitalizations often reflect recurring health problems, such as infections or malnutrition, which can disrupt growth and recovery. Hospitalization may also interrupt consistent nutritional intake and expose children to stressors that hinder their optimal development.22,23 This association underscores the need for health policymakers to focus not only on treating acute health issues but also on implementing preventive measures that address the underlying causes of recurrent hospitalization. Improving access to primary healthcare services and enhancing nutritional support may reduce the prevalence of stunting among children with a history of hospitalization. This finding highlights the importance of a holistic approach to child health, emphasizing the interconnectedness of hospital care, nutrition, and long-term developmental outcomes of children.
Additionally, Maternal factors, particularly postpartum depression, played a significant role and were strongly associated with stunting. Poor maternal mental health can negatively affect feeding practices and caregiving, especially during the critical first 1000 days of life. 24 Children of mothers experiencing postpartum depression may not receive adequate nutrition or responsive care, thereby increasing their risk of growth faltering. This finding is also supported by a study in Ethiopia 25 and a multi-country study that assessed psychological risk factors related to women and child stunting across 137 low and middle-income countries, 26 which similarly reported links between maternal depression and child undernutrition. A study in West Java, Indonesia, reported that maternal well-being was linked to stunting prevention behavior among mothers. 8 Comparisons with higher-income countries reveal different dynamics, while maternal depression was also associated with child growth delays. 27 These findings suggest that both maternal well-being and child morbidity play crucial roles in shaping stunting outcomes, underscoring the need for integrated approaches that address maternal health, childcare practices, and infection prevention to reduce the prevalence of stunting.
Despite these contributions, this study has several limitations. First, recall bias may have affected mothers’ reports of postpartum depression, particularly when recalling events months or years after delivery. Second, some participants were unable to provide complete child health records, which limited data validation. Third, the matched case-control design used a hospital-based sample from purposively selected districts, which restricted generalizability to broader populations. Finally, the relatively small sample size may have reduced the statistical power and contributed to the wide confidence intervals in some analyses.
Overall, these findings underscore the multifactorial nature of stunting, which is shaped by child health, maternal mental well-being, and healthcare access. Preventive strategies should integrate maternal support, infection control, and nutrition programs to break the cycle of undernutrition and poor health outcomes in children.
Conclusion
This matched case-control study identified the key determinants of stunting among children aged 6 to 59 months in Central Java, Indonesia. Stunting is strongly associated with a history of pulmonary infections, low birth weight, and prior hospitalizations, underscoring the interlinked pathways of infection, growth, and nutritional vulnerability. Maternal postpartum depression also emerged as a significant factor, highlighting the importance of maternal mental health in shaping feeding practices and childcare during the critical first 1000 days of life.
These findings emphasize that stunting is not solely a nutritional problem but a multifactorial condition shaped by children’s health status, maternal well-being, and access to healthcare. Therefore, efforts to reduce stunting must adopt an integrated approach that combines improved infection prevention, maternal mental health support, and strengthened nutrition programs. Preventive, community-based strategies that reduce hospitalization and enhance early life care are especially important for breaking the cycle of undernutrition and recurrent illness.
Footnotes
Author Contributions
YDP: Conceptualization; Methodology; Writing – Original Draft; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. TY: Supervision; Writing – Review & Editing; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. ER: Data Curation; Investigation; Validation; Writing – Original Draft; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SH: Formal Analysis; Visualization; Writing – Review & Editing; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SW: Funding Acquisition; Resources; Supervision; Writing – Original Draft; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. DCK: Literature Review; Project Administration; Writing – Review & Editing; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Provincial Health Office of Central Java. The funding body had no role in the design of the study, data collection, analysis, or interpretation, nor in writing the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.