
Abstract
Acute otitis media (AOM) is one of the most common infectious diseases in pediatric clinical facilities and has a significant impact on health care. It is a polymicrobial disease and is usually preceded by a viral upper respiratory tract infection. Data on the spectrum of viruses that cause AOM in Indonesia are still limited. This study analyzed nasopharynx (NP) samples collected from 119 school children with AOM in Banyumas Regency, Central Java, Indonesia. Viral RNA was extracted for cDNA synthesis, followed by PCR and sequencing tools for detection of a panel of respiratory viruses using family-level primers for Coronaviridae, Enterovirus, Bocavirus, and Pneumovirinae for bocavirus. In total, 37 out of 119 NP samples (31.1%) tested positive for viruses. Human rhinovirus B was the predominant virus identified (32.4%) followed by rhinovirus C (29.7%), human rhinovirus A (27%), and human bocavirus (5.4%). Rhinovirus are predominant viral pathogens within school children with AOM in Central Java, Indonesia.
Introduction
Acute Otitis Media (AOM) is one of the most common diseases in young children and is the second most common reason for an family planning visit.1,2 Almost all children under the age of 3 have experienced at least 1 episode of otitis media with effusion. 2 In Taiwan, 12.5% of children had developed otitis media in the first 3 year of their life. 3 Daycare attendance, poor maternal mental health, harsh parental discipline correlated with parent-reported occurrence of otitis media. 3 Wijayanti et al 4 reported that household firewood use, poor nutritional status and family history of ear infection are factors associated with the occurrence of AOM among school children in Central Java, Indonesia. Regardless of the mode of treatment used, the quality of life of the children with recurrent acute otitis media did not reach the same level as healthy children. 5
AOM is predominantly a bacterial infection, especially Streptococcus pneumoniae followed by Haemophilus influenzae and Moraxella catarrhalis, meanwhile, viruses cause one-third of cases. 1 The viruses most commonly associated with AOM symptoms were respiratory syncytial virus, rhinovirus, adenovirus, coronavirus, bocavirus, influenza virus, parainfluenza virus, enterovirus, and human metapneumovirus. 2 It was recently reported that non-typeable Haemophilus influenzae and rhinovirus were common bacterial and virus pathogens within the upper respiratory tract of peri-urban/urban South-East Queensland Australian children with and without otitis media. 6 Previously, we have reported that 73% and 69.7% of S. pneumoniae and H. influenzae were identified among school children with AOM in Banyumas Regency, Central Java, Indonesia respectively.7,8 Data on the spectrum of viruses that cause AOM in Indonesia are still limited. This study we continue to analyze nasopharynx (NP) samples collected from 119 school children with AOM in Banyumas Regency, Central Java, Indonesia. The results will provide insight into the epidemiology of respiratory viruses in school children with AOM in Central Java, Indonesia.
Materials and Methods
Specimen Collection
Specimen from the NP was collected from school children (<12 years of age) with a diagnosis of acute otitis media (AOM) attending primary schools in the Banyumas Regency, Southwest of Central Java Province, Indonesia, between 2018 and 2019 as previously reported. 4 NP swab specimens were collected using flocked nylon swabs (Cat. No. 503CS01) and placed into 2 ml of viral transport medium (VTM) prepared in-house, containing bovine brain heart infusion and antibiotics. Then, the specimens were transported to the laboratory, vortexed, and stored at −80°C within 4 hours after collection. 7
Total RNA Extraction and Viral Detection
Viral nucleic acid was extracted using QIAamp Viral RNA Minikit (Qiagen, Hilden, Germany) according to the manufacturer`s instructions. Viral specific targets were identified by using reverse transcription–PCR (RT-PCR). In summary, 60 µl of viral DNA-RNA was obtained and 4 µl used as a template for complementary DNA (cDNA) synthesis using GoScript Reverse Transcription System (Promega, Madison, USA) and random hexamers.9,10
Singleplex PCR assays were used for detection of a panel of respiratory viruses using family-level primers for Coronaviridae, Enterovirus, Bocavirus, and Pneumovirinae. All of the primers and positive controls that were used in the amplification reaction were based on previous reports.9,10 Singleplex PCR reaction was performed in thermal cycler ProFlexTM PCR System with appropriate run controls. A recombinant plasmid representing sequence fragments of all family viruses was constructed and used as the positive control. For amplification, 2 µl of cDNA template was added to 23 µl of Promega Go Taq Green Polymerase Master Mix (Promega, Madison, USA). All PCR products were analyzed using electrophoresis in 1.5% agarose gel. Visualization of positive band was performed using Gel Imaging BioRad Gel Doc XR System and Quantity 1 1-D Analysis Software (Bio-Rad, California, USA).9,10
All samples with a positive band were followed up for further characterization by fragment sequencing based on Sanger method using BigDye® Terminator v3.1 and Applied Biosystem (ABI) sequencing machine. Sequencing results were analyzed using Geneious Software R8 version 8.1 (BiAOMtters Ltd, Auckland, New Zealand) and compared with GenBank database by BLAST for sequence homology.
Results
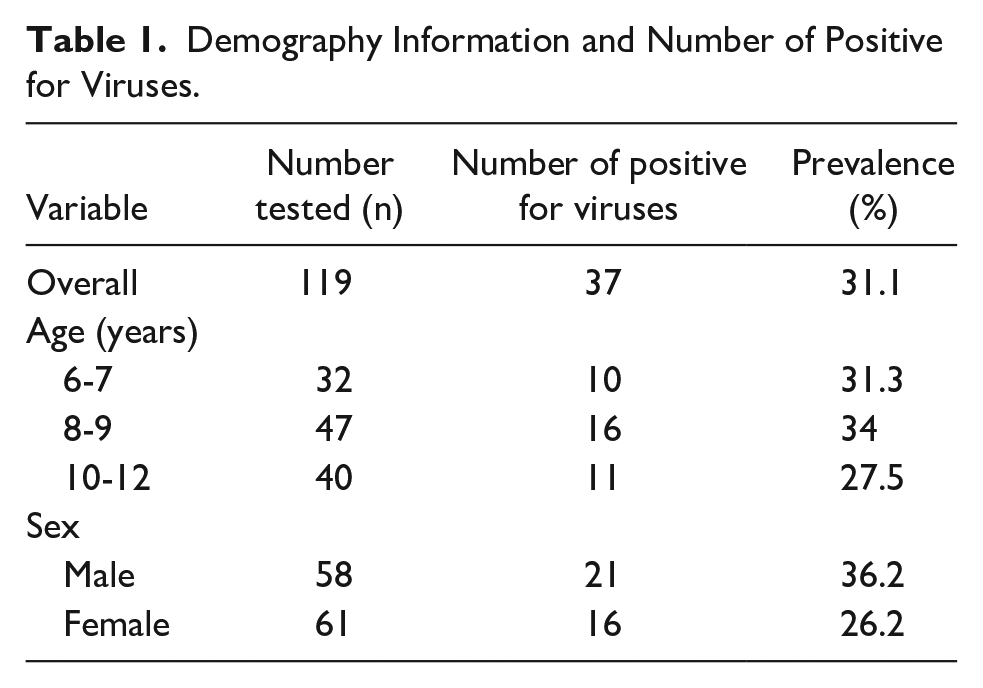
Viral infections were detected in 37 (31.1%) of 119 children between ages of 6 and 12 with higher prevalence in male (36.2%) than female (26.2%; Table 1). We also observed that children aged 8 to 9 (34%) had the highest number of AOM cases than those aged of 6 to 7 (31.3%) and older than 8 years old (27.5%). Most of these cases were single infection and predominantly caused by Enterovirus in 33 (89.2%) samples, followed by Bocavirus in 2 (5.4%) samples. Dual infection was observed in 2 (5.4%) samples as a result of Coronavirus and Enterovirus co-infection. However, no pneumovirinae was found in this study.
Demography Information and Number of Positive for Viruses.
Genetic characterization by sequencing was able to identify 6 virus species as described in Table 2. Thirty-five out of 37 AOM cases were caused by single viral infection with Human Rhinovirus B (HRV-B) as the leading cause and responsible for 12 (32.4%) cases, followed by Rhinovirus C in 11 (29.7%) cases. In addition, 10 (27%) cases of AOM were due to Human Rhinovirus A (HRV-A) infection, while only 2 (5.4%) cases were attributable to Bocavirus PgBoV-2 infection. Moreover, dual viral infection was also discovered in 2 (5.4%) cases, each caused by an OC43-Rhinovirus and a HKU1- HRV-B co-infection.
Viral Detection From 119 School Children With AOM in Central Jawa, Indonesia.

Further analysis of the sequencing results revealed 5 different serotypes of HRV-A and 1 serotype of HRV-B. Among 12 of HRV-B infections, 6 AOM cases were caused by HRV-B52 while the other 6 cases were untypeable HRV-B. On the contrary, more diverse serotypes were observed in HRV-A infections. Although, there was only a single case of infection for each serotype. The HRV-A serotypes were consisted of HRV-A38, HRV-A49, HRV-A60, HRV-A68, and HRV-A81, whereas the rest of HRV-A infections were untypeable.
Previously, we have reported that 73% and 69.7% of S. pneumoniae and H. influenzae were identified from the same set of nasopharyngeal specimens respectively.7,8 We analysis further regarding the co-infection of viruses and bacteria of S. pneumoniae and H. influenzae. We found that 62.2% (23/37) of nasopharyngeal swab samples that detected positive for viruses were also detected positive for both S. pneumoniae and H. influenzae bacteria. Meanwhile, nasopharyngeal swab samples were positive for viruses and only positive for S. pneumoniae as many as 24.3% (9/37) and only 8.1% (3/37) of the samples positive for viruses only positive for H. influenzae. In addition, 5.4% (2/37) only positive for viruses remained negative for S. pneumoniae and H. influenzae (Table 3).
Viruses and Bacterial Identified in the Nasopharynx School Children With AOM in Central Jawa, Indonesia.

Discussion
Common respiratory viruses including HRV, HCV, and HBV were detected in 31.1% of NP swabs of school children with AOM in Banyumas Regency, Central Java, Indonesia. Human Rhinovirus (59.4%) has the highest prevalence in this study. In addition, Rhinovirus was also responsible for 29.7% of AOM cases. This result consistent with previous studies that reported Human Rhinovirus and Rhinovirus among the more common virus group found in children nasopharynx and middle ear fluid (MEF) and have been strongly associated with AOM.11-13
Furthermore, we were able to detect Human Bocavirus from 2 samples (5.4%) in this study. This virus has been detected in children with respiratory tract infections.14,15 The presence of this virus alone or in combination with other viruses may worsen the clinical symptoms of AOM. 15 Although several studies have also detected Human Bocavirus in respiratory tract of children without respiratory symptoms.16-18
In 2 cases, dual viral infections both involving Coronavirus and Enterovirus were observed. The presence of more than 1 viral agent might aggravate the symptoms and prolong the clinical outcomes of AOM. A study by Chonmaitree, et al, 19 revealed that higher number of viral load in Upper respiratory infection (URI) patients resulted in higher degree of inflammation which increased the disease severity and the risk of AOM complication. Therefore, the quantification of the viral load would give us a better understanding of the important role of specific viruses in the disease pathogenesis.
AOM itself has been known to be a polymicrobial disease that induced by either bacteria or viruses infection alone or a complication of both. The presence of viruses in upper respiratory tract increases the risk of AOM by facilitating the bacteria invasion from nasopharynx to middle ear canal. URI can occur before or concurrently with AOM. The viral infection leads to inflammation in nasopharynx and eustachian tube and alter the bacteria adherence and colonization ability. Both interact with each other in the disease pathogenesis and is suggested to worsen the clinical symptoms of AOM. 13 In
Conclusion
Rhinovirus are predominant viral pathogens within school children with AOM in Central Java, Indonesia.
Footnotes
Acknowledgements
We are grateful to the children and parents for participating in the study, and all teachers and staffs at primary schools in Banyumas Regency, Central Java, Indonesia. We also thank Wisnu Tafroji, Miranti Oviani, Shafa Rana Nusaibah, Wisiva Tofriska, Yayah Winarti, Heri Priyanto, and Hanifah Fajri Maharani Putri for technical assistance and discussion.
Author’s Note
Anton Budhi Darmawan is also affiliated to Department of Otorhinolaryngology, Head and Neck Surgery, Jenderal Soedirman University, Purwokerto, Indonesia.
Author Contributions
Conceptualization: ABD, DJW, and DS; methodology: AKD, HFMP, and AW; validation: AKD, HFMP, and AW; analysis: AKD, HFMP, AW, and DS; investigation: ABD, DJW, and DS; resources: ABD and DJW; data curation: ABD, DJW, AKD, HFMP, and AW; writing—original draft preparation: ABD, DS, and HFMP; Writing review and editing: DS and HFMP; funding acquisition: DJW. All authors read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Ministry of Research and Technology, Indonesia No 176/SP2H/AMD/LT/DPRM/2020.
Data Availability
The data presented in this study are available on request from the corresponding authors.
Institutional Review Board Statement
This study was approved by the Ethical Committee of Faculty of Medicine, University of Jenderal Soedirman, Purwokerto, ethical number: 4015/KEPK/FK/2018.
Informed Consent Statement
The children’s parents signed informed consent forms prior to data and specimen collection.