
Abstract
Background:
BCG vaccination is the primary defense against severe childhood tuberculosis, yet data on its uptake in Somalia are limited.
Methods:
Data from the Somalia Demographic and Health Survey were analyzed, including 2025 children aged 0 to 59 months with vaccination cards. Descriptive statistics estimated national and regional BCG coverage, and 2-level logistic regression assessed individual and community-level determinants.
Results:
National BCG coverage was 57.3%, ranging from 31% in Nugal to 78% in Mudug. Children with higher birth orders were less likely to be vaccinated. Older children had higher vaccination odds, and maternal tetanus toxoid receipt was positively associated with BCG uptake. Middle-income children were more likely to be vaccinated. Children from rural and urban areas had lower odds than nomadic children. Community-level factors explained 10.9% of the variance.
Conclusion:
BCG coverage in Somalia is below the WHO’s 90% target. Addressing inequities in birth order, maternal health, wealth, and geography is essential.
Introduction
Immunization is a cornerstone of public health, globally recognized for its critical role in reducing child morbidity and mortality from vaccine-preventable diseases (VPDS).1,2 As 1 of the most cost-effective health interventions, immunization prevents millions of deaths annually and contributes significantly to global health targets, including those outlined in the Immunization Agenda 2030.3,4 Among childhood vaccines, Bacille Calmette-Guérin (BCG) plays a vital role in combating tuberculosis (TB), especially in protecting young children against its severe forms, such as meningitis and miliary TB.5-7 The World Health Organization (WHO) recommends administering a single dose of BCG at birth or as soon as possible in high TB-burden settings. 7 As a result, BCG vaccination is routinely included in the Expanded Programme on Immunization (EPI) across many countries, particularly in Sub-Saharan Africa. 8
Despite its benefits, ensuring high BCG coverage remains a persistent challenge, especially in fragile and resource-limited settings.9,10 Globally, millions of children, particularly those in underserved or remote communities, miss timely BCG vaccination, which increases the risk of TB infection. 11 Somalia, which faces prolonged conflict, political instability, and humanitarian crises, exemplifies such a setting. These challenges have severely impacted the health system and compromised the delivery of routine immunization services. 12 Consequently, Somalia has historically recorded the lowest BCG coverage rates worldwide. 13
Understanding the factors influencing BCG immunization coverage is essential for developing strategies to improve vaccine uptake. Previous studies from low- and middle-income countries (LMICS), especially those with fragile health systems, have identified various determinants. These include maternal education, household wealth, urban versus rural residence, access to health facilities, antenatal care attendance, and parental knowledge and attitudes toward vaccination.14-18 A study conducted in northern Somalia found that factors such as healthcare infrastructure, maternal literacy, and regional health budgets have been shown to affect immunization rates. 17
Other international studies have similarly emphasized the role of health system access and caregiver attitudes.19,20 Although the general determinants of childhood immunization are well documented, there remains a gap in recent nationally representative evidence from Somalia. The 2020 Somalia Demographic and Health Survey (SDHS) presents a valuable opportunity to explore BCG coverage and its associated factors in this context. Understanding these factors is essential for designing targeted interventions that can strengthen the immunization program, improve BCG uptake, and ultimately reduce the burden of childhood TB in Somalia. Therefore, this study aimed to identify the factors influencing BCG immunization coverage among children aged 6 to 59 months in Somalia using data from the 2020 SDHS. These findings provide evidence-based insights to inform policies and interventions that promote equitable and timely BCG vaccination.
Materials and Methods
Study Design and Objective
This cross-sectional analytical study investigated individual- and community-level determinants of Bacillus Calmette-Guérin (BCG) vaccination among children aged 0 to 59 months in Somalia. The primary objective was to identify the sociodemographic, maternal, and contextual factors associated with the likelihood of receiving BCG vaccination in this population.
Data Source
Data were drawn from the 2020 Nationwide Survey Data, a nationally representative household survey that used a multistage stratified cluster sampling approach to capture urban, rural, and nomadic populations in all regions of Somalia. Enumeration areas were selected with probability proportional to size, and within each selected cluster, households were sampled systematically to yield a dataset weighted to reflect the national distribution of children aged under 6 years.
Sample Size and Sampling Procedure
The analytical sample comprised children aged 0 to 59 months with complete information on BCG vaccination status and key explanatory variables. After excluding records with missing data, the final weighted sample included 2025 children. From the initial dataset of 3547 children aged 0 to 59 months, a total of 1466 were excluded due to missing information on 1 or more of the key variables, resulting in the final analytical sample of 2081 (unweighted). The sampling weights provided by the survey were applied throughout to account for the complex design and to ensure the generalizability of the findings.
Measurement of Variables
The binary outcome variable for BCG vaccination status was derived from the DHS variable H2 (“Received BCG”). A child was coded as “Vaccinated” if the source of information was “Vaccination date on card,” “Reported by mother,” or “Vaccination marked on card.” Conversely, a child was coded as “Not Vaccinated” if the response was “No.” The explanatory variables included maternal characteristics (education level, age group, media exposure, number of antenatal care visits, and tetanus toxoid vaccination status), child characteristics (sex, age category, birth order, place of delivery, and birth size), household wealth index, place of residence, and administrative region.
Statistical Analysis
All analyses were conducted using Stata 16, incorporating sampling weights, clustering, and stratification to reflect the survey’s design. Descriptive statistics were used to summarize the sample characteristics and BCG coverage. Bivariate associations between each explanatory variable and vaccination status were assessed using survey-adjusted chi-square tests, with a significance threshold of P < .05. All key individual- and community-level variables identified from the literature were included in the final multivariable model to control for potential confounding effects, regardless of their significance in the bivariate analysis. Four sequential models were fitted: a null model (Model 0) to quantify the baseline community-level variance; Model I, including only individual-level factors; Model II, including only community-level factors; and Model III, which combined both sets of predictors. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were used to measure associations. Random effect parameters, including the intraclass correlation coefficient, median odds ratio, and proportional change in variance, were calculated to assess the between-cluster heterogeneity. Model fit was evaluated using the log-likelihood, Akaike Information Criterion, and Bayesian Information Criterion, and variance inflation factors confirmed the absence of multicollinearity.
Results
Sociodemographic Characteristics and BCG Vaccination Prevalence
This study utilized data from 2025 weighted children aged 0 to 59 months included in the descriptive analysis from the 2020 Nationwide Survey Data (Table 1). Regarding maternal characteristics, most mothers had no formal education (71.3%). A notable proportion of mothers were aged 20 to 24 years (26.4%) and 25 to 29 years (26.7%). Most mothers (77.7%) reported no exposure to the media (TV or radio). Antenatal care (ANC) coverage varied: 45.4% of mothers had zero ANC visits, 38.8% had 1 to 2 visits, and 15.8% had 3 to 4 visits. Regarding tetanus toxoid (TT) vaccination before birth, 50.7% of mothers received no doses, 17.6% received 1 dose, and 31.7% received 2 or more doses. Regarding child characteristics, there was a near-even split by sex (53.7% male, 46.3% female). The largest proportion of children was in the 48 to 59 months age group (36.8%), followed by 36 to 47 months (25.0%). Most children were of birth order 2 to 3 (64.6%). Most children were born at home (60.5%), and most were of average size at birth (62.1%). Household wealth was categorized into 3 groups, with the largest proportion falling into the middle wealth quintile (49.8%), followed by the poor (25.3%) and the rich (24.9%). In terms of residence, 58.4% lived in urban areas, 26.5% in rural areas, and 15.1% were nomads. The sample was distributed across all regions, with Banadir having the largest proportion (22.1%). Figure 1 presents the overall prevalence of BCG vaccination; 57.3% of the children had received the BCG vaccination, while 42.7% had not.
Bivariate Analysis of Sociodemographic Characteristics and BCG Vaccination Status.
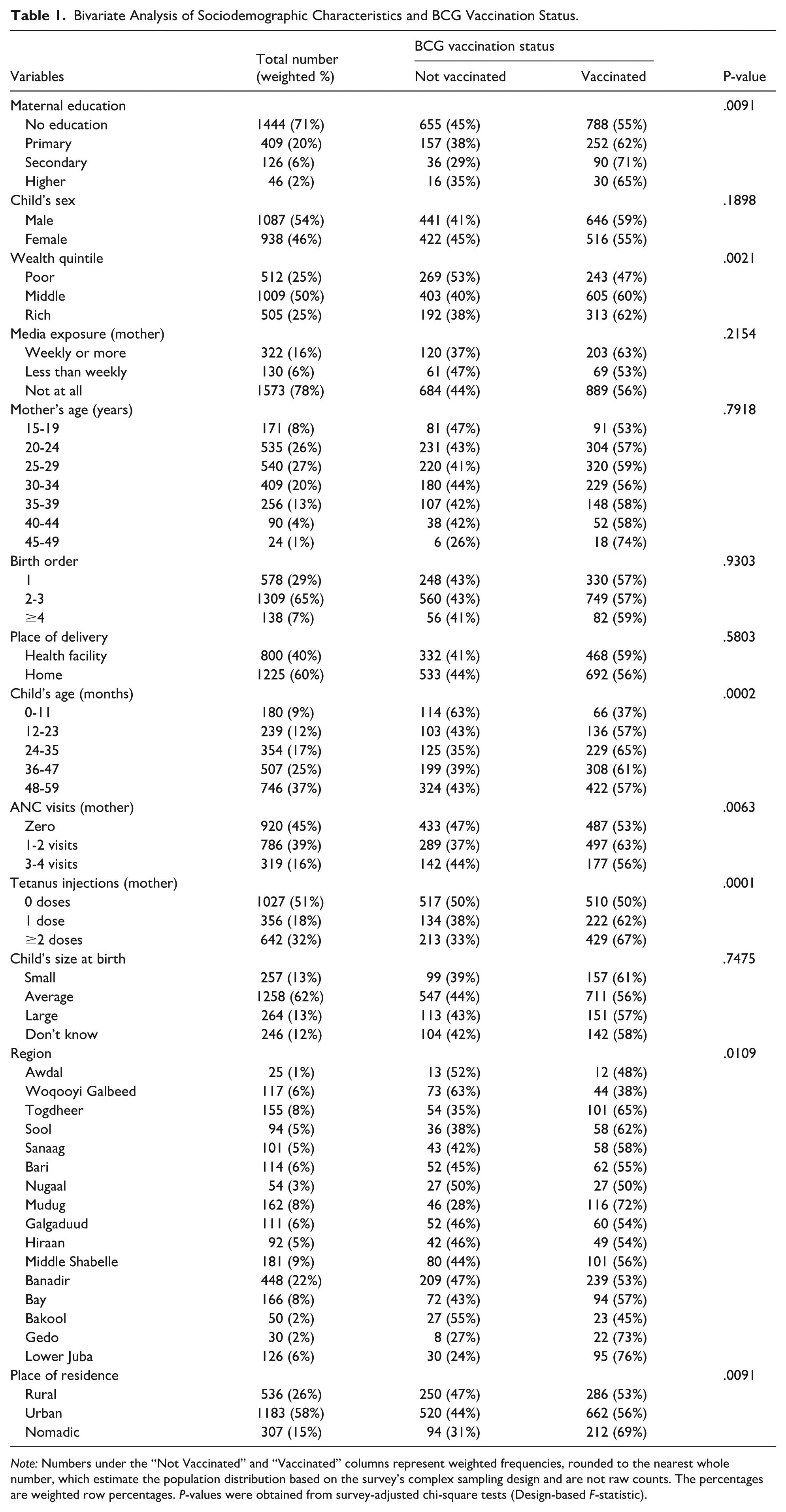
Note: Numbers under the “Not Vaccinated” and “Vaccinated” columns represent weighted frequencies, rounded to the nearest whole number, which estimate the population distribution based on the survey’s complex sampling design and are not raw counts. The percentages are weighted row percentages. P-values were obtained from survey-adjusted chi-square tests (Design-based F-statistic).

Prevalence of BCG vaccination among children aged 0 to 59 months in Somalia (2020 Nationwide Survey Data).
Table 1 also details the prevalence of BCG vaccination across different sociodemographic characteristics of the participants. Bivariate analyses (survey-adjusted chi-square tests) indicated significant associations (P < .05) between BCG vaccination status and several factors. Higher vaccination prevalence was observed among children whose mothers had secondary education (71.3%) compared those with no education (54.6%) (P = .0091). BCG coverage was higher among children from rich households (62.0%) than among those from poor households (47.4%) (P = .0021). Child age was significantly associated with BCG vaccination, with the lowest coverage among infants 0 to 11 months (36.8%) and highest among those 24 to 35 months (64.6%) (P = .0002). The number of ANC visits was linked to BCG vaccination status, with children of mothers attending 1 to 2 visits having higher coverage (63.2%) than those with zero visits (52.9%) (P = .0063). Maternal tetanus vaccination status was also significant, with higher BCG coverage among children whose mothers received 1 dose (62.3%) or 2 or more doses (66.8%) of TT compared with no doses (49.7%) (P < .0001). Place of residence showed significant differences, with nomadic children having the highest BCG coverage (69.2%) compared to rural (53.4%) and urban (56.0%) children (P = .0091). Significant regional variations in BCG vaccination prevalence were also observed (P = .0109). Child sex (P = .1898), media exposure of the mother (P = .2154), mother’s age (P = .7918), birth order (P = .9303), place of delivery (P = .5803), and child size at birth (P = .7475) were not significantly associated with BCG vaccination status in the initial bivariate analyses.
Individual- and Community-Level Factors Associated With BCG Vaccination
Random Effects
Table 2 details the random effects (community-level variation) and the model comparison metrics. The null model (Model 0), without predictors, confirmed significant between-community variation in BCG vaccination (Cluster Variance = 0.555). The Intra-Cluster Correlation Coefficient (ICC) was 14.4%, indicating that approximately 14.4% of the total variance in BCG vaccination status stemmed from differences between communities. The Median Odds Ratio (MOR) of 1.99 suggested a notable contextual influence, implying that a child’s odds of receiving BCG vaccination could change by a median factor of 1.99 if moving from a low-coverage to a high-coverage community. Adding individual-level factors (Model I) reduced the cluster variance to 0.477 (ICC = 12.7%; MOR = 1.90). These factors explained 14.2% of the initial community-level variance (PCV = 14.2). Conversely, adding only community-level factors (Model II) resulted in a variance of 0.444 (ICC = 11.9%, MOR = 1.86) and explained 20.1% of the community variance (PCV = 20.1%). This suggests that the included community-level factors (residence and region) have a slightly stronger explanatory power for the between-community variation than the individual-level factors alone.
Random Effect and Model Comparison of Individual- and Community-Level Factors Associated With BCG Vaccination.
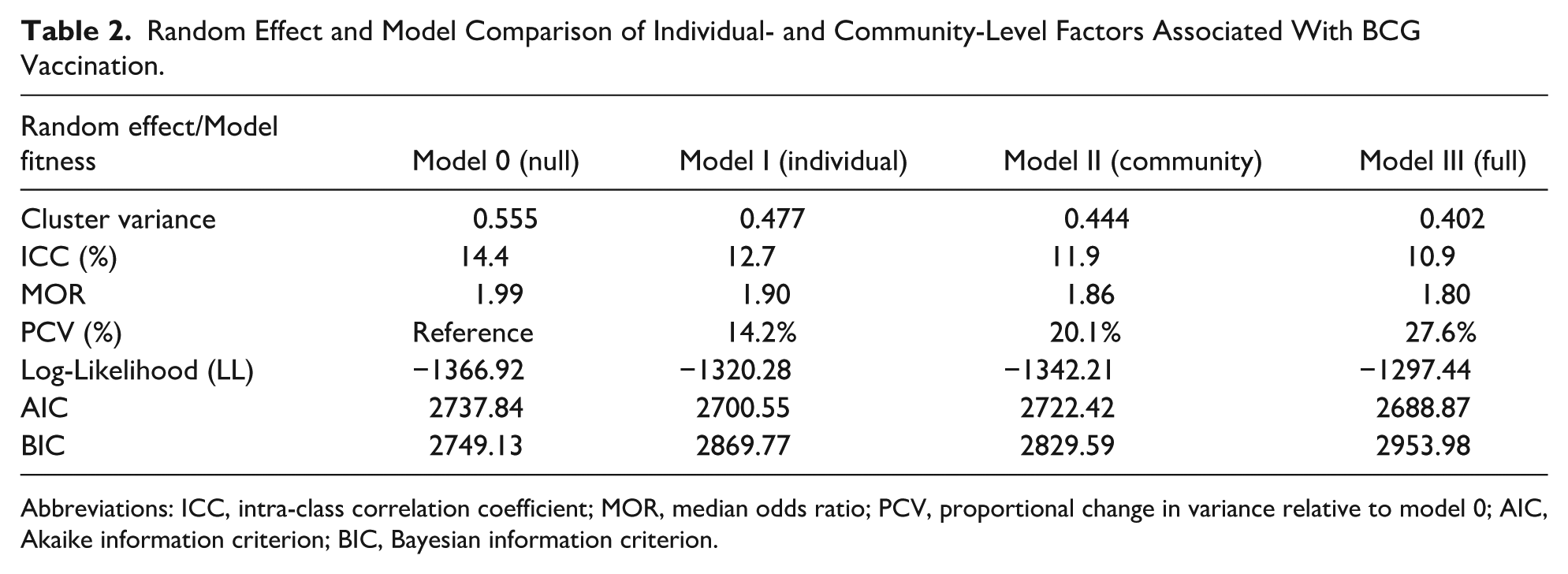
Abbreviations: ICC, intra-class correlation coefficient; MOR, median odds ratio; PCV, proportional change in variance relative to model 0; AIC, Akaike information criterion; BIC, Bayesian information criterion.
The final model (Model III), which included both individual and community factors, achieved the lowest cluster variance (0.402), ICC (10.9%), and MOR (1.80). All predictors combined explained 27.6% of the initial between-community variance (PCV = 27.6%). The persistence of significant cluster variance (P < .0001) and an MOR substantially above 1 highlights the continued importance of the community context. Model fit assessment using Log-Likelihood, AIC, and BIC showed progressive improvement across models. Model III yielded the lowest AIC (2688.87), indicating the best fit to the data while accounting for the model complexity. Consequently, Although the BIC for Model III (2953.98) was slightly higher than for other models, reflecting its penalty for a greater number of parameters, the lower AIC and the strong theoretical justification for including both individual and community predictors support its selection as the final model for its enhanced explanatory power. Model III was used to interpret the fixed effects.
Fixed Effects
Table 3 presents the fixed effects results (adjusted odds ratios [aOR] with 95% confidence intervals [CI) from the final multilevel logistic regression model (Model III). At the individual level, maternal education, child’s sex, wealth quintile, media exposure of the mother, mother’s age, place of delivery, number of ANC visits, and child’s size at birth were not significantly associated with BCG vaccination in the final adjusted model.
Multilevel Multivariate Logistic Regression of Individual- and Community-Level Factors Associated With BCG Vaccination.
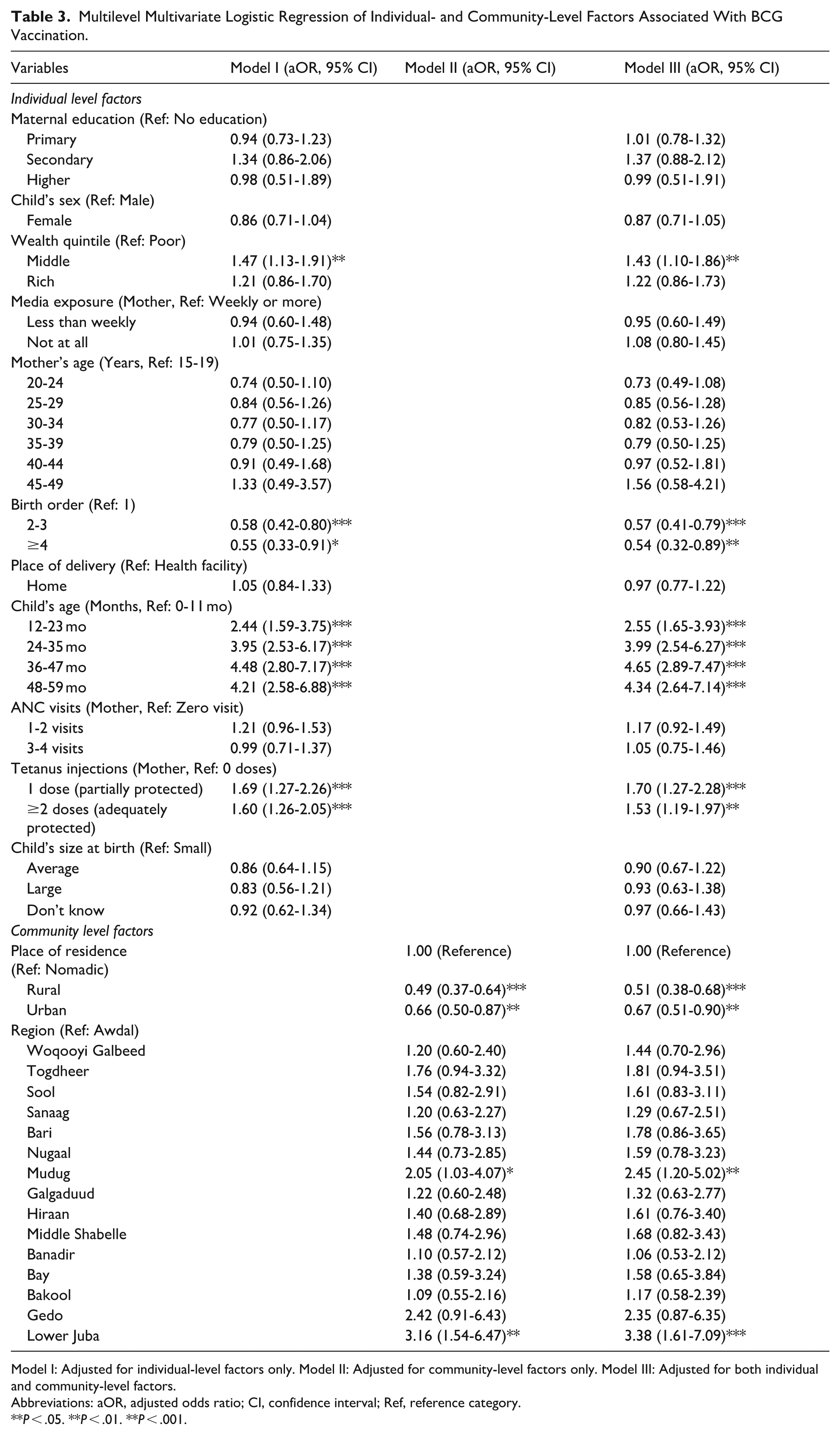
Model I: Adjusted for individual-level factors only. Model II: Adjusted for community-level factors only. Model III: Adjusted for both individual and community-level factors.
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; Ref, reference category.
P < .05. **P < .01. **P < .001.
However, birth order was significantly associated with BCG vaccination status. Children of birth order 2-3 (aOR = 0.57, 95% CI: 0.41-0.79) and those of birth order ≥4 (aOR = 0.54, 95% CI: 0.32-0.89) had significantly lower odds of being vaccinated than first-born children.
Child age was a strong predictor. Compared to children aged 0 to 11 months, those aged 12 to 23 months (aOR = 2.55, 95% CI: 1.65-3.93), 24 to 35 months (aOR = 3.99, 95% CI: 2.54-6.27), 36 to 47 months (aOR = 4.65, 95% CI: 2.89-7.47), and 48 to 59 months (aOR = 4.34, 95% CI: 2.64-7.14) had significantly higher odds of BCG vaccination.
Maternal tetanus toxoid (TT) vaccination status was also a significant factor. Children whose mothers received 1 dose of TT (aOR = 1.70, 95% CI: 1.27-2.28) or 2 or more doses of TT (aOR = 1.53, 95% CI: 1.19-1.97) had higher odds of BCG vaccination than children whose mothers received no TT.
At the community level, place of residence was significantly associated with BCG vaccination status. Children in rural (aOR = 0.51, 95% CI: 0.38-0.68) and urban (aOR = 0.67, 95% CI: 0.51-0.90) areas had lower odds of being vaccinated than those in nomadic areas (reference).
Significant regional disparities persisted after controlling for the other factors. Compared with children in the Awdal region (reference), those in Mudug (aOR = 2.45, 95% CI: 1.20-5.02) and Lower Juba (aOR = 3.38, 95% CI: 1.61-7.09) had significantly higher odds of BCG vaccination. The other regions did not show statistically significant differences compared to Awdal in the final model.
Discussion
This study aimed to identify individual and community-level factors influencing BCG immunization coverage among children aged 6 to 59 months in Somalia, utilizing data from the 2020 Somalia Demographic and Health Survey (SDHS). In our study, the prevalence of BCG vaccination among children aged 6 to 59 months in Somalia was 57.3%. This figure, while indicative of a majority of children receiving the vaccine, still falls short of the universal coverage targets aimed for by global and national immunization programs, especially considering BCG is recommended at birth or shortly thereafter to provide early protection against tuberculosis. 21 The observed coverage in Somalia was considerably higher than that in studies conducted in Northern Somalia and Indonesia.14,17 Somalia’s BCG coverage faces significant challenges compared to other East African nations. For instance, studies in Ethiopia have reported varying but often higher BCG coverage rates; a 2019 study by Tsehay et al on BCG scar prevalence found coverage over 80% in some areas, 22 while a multilevel analysis of the 2016 Ethiopian DHS data showed about 79.9% BCG coverage. 23 The relatively low coverage in Somalia likely reflects protracted conflict, a fragmented health system, and difficulties in accessing healthcare services, which act as significant barriers for married women and their families in seeking preventative care for their children.
In our study, birth order was a significant determinant of BCG vaccination. Children of birth order 2-3 (aOR = 0.57) and those of birth order ≥4 (aOR = 0.54) had significantly lower odds of being vaccinated than first-born children. This finding aligns with several studies conducted in low- and middle-income countries (LMICs). For instance, studies in Ethiopia were negatively associated with complete immunization.24,25 Similarly, research in Senegal has indicated that later-born children are less likely to be fully immunized. 26 The variation in the findings could be due to several factors. In the Somali context, particularly for married women, an increase in family size may lead to resource dilution, both financially and in terms of maternal time and attention per child. Furthermore, mothers may perceive themselves as more experienced with subsequent children. They may underestimate the necessity of timely vaccination clinic visits or face increased logistical challenges in bringing multiple children to health facilities for vaccination. Previous studies have highlighted that maternal overload and transportation difficulties are significant barriers to accessing child health services in SSA. 27
Child’s age was a strong predictor of BCG vaccination. Compared with children aged 0 to 11 months, older children in the age groups 12-23 months (aOR = 2.55), 24 to 35 months (aOR = 3.99), 36 to 47 months (aOR = 4.65), and 48 to 59 months (aOR = 4.34) had significantly higher odds of BCG vaccination. This finding is consistent with a study conducted in northern Somalia, 17 where children older than 23 months had greater odds of being ever vaccinated. This pattern suggests significant missed opportunities for BCG vaccination at birth or within the first few months of life, which is the recommended time. The higher odds among older children likely reflect the cumulative probability of vaccination over time, including catch-up vaccinations, rather than optimal, timely immunization. Alternatively, as the reviewer insightfully suggests, this trend could indicate a deterioration of the immunization program in the years immediately preceding the survey, resulting in lower coverage for the youngest cohorts. This delay undermines the primary goal of BCG, which is to protect young infants from severe TB when they are most vulnerable. 28 This finding points to a critical gap in ensuring birth-dose administration and highlights the need for strategies that focus on timely vaccination. The reasons for the low uptake in the 0 to 11-month group could include barriers to accessing postnatal care, lack of awareness about the need for BCG vaccination at birth, or health system weaknesses in delivering vaccines immediately after birth, particularly for home deliveries, which are common in Somalia.
Maternal tetanus toxoid (TT) vaccination status was significantly associated with higher odds of child BCG immunization. Children whose mothers received 1 dose of TT (aOR = 1.70) or 2 or more doses (aOR = 1.53) had higher odds of BCG vaccination than children whose mothers received no TT dose. This is consistent with findings from various SSA countries, including Nigeria, 29 Ethiopia, 30 and Senegal, 26 where maternal utilization of antenatal care (ANC) services, which often includes TT vaccination, is linked to improved childhood immunization. This association can be explained by the increased contact between TT-vaccinated mothers and the healthcare system. Such interactions provide opportunities for health education, counseling on the benefits of child immunization, and building trust in health services, which are crucial for married women making healthcare decisions for their children. Mothers who access maternal health services, such as TT vaccination, are likely to be more health-conscious and receptive to preventive health measures for their children.
Children from the middle wealth quintile had higher odds (aOR = 1.43) of receiving BCG vaccination than those from poor families. This finding aligns with numerous studies conducted in Ethiopia, 31 Indonesia 31 and Bangladesh. 32 While the effect size is moderate, it highlights a persistent equity gap. Although the BCG vaccine is often provided free of charge in public facilities, indirect costs such as transportation, lost wages for the day, and childcare for other children can pose significant financial barriers for poorer families, particularly in a country like Somalia with limited social safety nets. Even a modest improvement in financial accessibility for the poorest households could translate into meaningful gains in national coverage. Wealthier households may also have better access to information, live in areas with better service availability, and be more empowered to overcome logistical hurdles in accessing healthcare. Our study found that place of residence was significantly associated with BCG vaccination, with children in rural (aOR = 0.51) and urban (aOR = 0.67) areas having lower odds of vaccination than those in nomadic areas. This indicates that nomadic children in Somalia were more likely to receive BCG vaccinations. This finding is particularly noteworthy and contrasts with some studies.33,34 Immunization services in Somalia are delivered through a mix of fixed health facilities, outreach programs, and mobile teams often run by non-governmental organizations, which are specifically designed to reach remote and mobile populations. The higher BCG coverage among nomadic children in Somalia could be attributed to several factors, While the reasons are not immediately clear from our data, 1 possibility is the success of targeted outreach campaigns or mobile health teams specifically designed to reach these mobile populations. However, this remains speculative. This finding warrants further qualitative investigation to understand the specific health-seeking behaviors and programmatic factors that may be driving this unexpected and positive outcome.
Significant regional disparities in BCG vaccination were also observed. Children in the Mudug (aOR = 2.45) and Lower Juba (aOR = 3.38) regions had significantly higher odds of BCG vaccination than those in the Awdal region. Regional variations in immunization coverage are well-documented in many countries.35,36 These disparities in Somalia could be due to differences in the functionality of the health system across regions, varying levels of security and stability affecting service delivery, the presence and effectiveness of NGOs and international partners supporting immunization programs, resource allocation, and fidelity of health policy implementation. Specific health initiatives or better-managed vaccination campaigns in Mudug and Lower Juba may explain their higher coverage rates.
Study Limitations
This study has several limitations inherent to its design and data source. First, the cross-sectional nature of the Somalia Demographic and Health Survey (SDHS) data precludes the establishment of causal relationships between the identified determinants and BCG vaccination; we can only infer statistical associations. Second, the measurement of our outcome variable relied on both vaccination cards and maternal recall. The use of maternal recall is subject to potential recall and social desirability biases, which may lead to an over- or under-estimation of the true vaccination coverage. Third, while our analysis controlled for a wide range of variables, the potential for unmeasured confounding remains. Factors not captured in the SDHS, such as the quality of local healthcare services, community-level health beliefs, or the specific impact of regional insecurity on service delivery, could also influence vaccination uptake. Finally, the generalizability of our findings is constrained as the survey data did not include the Middle Juba and Lower Shabelle regions. Consequently, while the study is representative of the surveyed areas, our results may not fully reflect the vaccination dynamics across the entire nation, and the interpretation of these “nationwide” estimates should consider this geographic limitation.
Conclusion
BCG vaccination coverage in Somalia is 57.3%, far below the 90% WHO target. Key drivers of inequity include birth order, maternal health service utilization, household wealth, and geography. To improve coverage, we recommend several actionable policy interventions. First, health programs should design campaigns specifically targeting mothers of higher birth-order children, addressing potential barriers like time constraints and perceived lower risk. Second, maternal and child health services must be better integrated; every antenatal and postnatal visit, including for tetanus toxoid vaccination, should be leveraged as an opportunity to check and provide infant vaccinations. Third, financial and logistical barriers for the poorest households must be reduced, potentially through community transport vouchers or conditional cash transfers. Finally, while nomadic populations showed higher coverage, outreach efforts must be sustained and a deeper understanding of this success is needed, while targeted mobile immunization strategies should be intensified for underserved rural and urban communities, particularly in low-performing regions. Implementing these tailored strategies is essential for moving Somalia toward equitable protection against childhood tuberculosis.
Footnotes
ORCID iDs
Author Contributions
MMA and YSAH conceived the study. The design was developed under MMA’s lead in collaboration with the team. MAO prepared the materials and collected the data, and also carried out the analyses and interpreted the results. ASA, MMA, and YSAH wrote the first draft. All authors contributed to subsequent writing, review, and editing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.