
Abstract
Background:
Vaccination is a vital public health intervention for reducing child mortality from vaccine-preventable diseases. Despite progress, disparities persist in fragile settings such as Somalia. Galmudug State faces challenges including socioeconomic inequalities, geographic barriers, insecurity, and limited healthcare infrastructure. This study examined maternal and child vaccination coverage in Galmudug, focusing on socio-demographic, healthcare, and geographic factors.
Methods:
This descriptive study analyzed secondary data from the 2021 Galmudug Health and Demographic Survey, which included 1741 households. Vaccination coverage was assessed for children aged 12 to 23 months alongside maternal education, wealth, and residence type.
Results:
Only 9% of children were fully vaccinated. Coverage was highest among educated mothers and wealthier households, with 14% in urban areas compared with 2% in nomadic populations. Low antenatal care attendance (66% had no visits) and high dropout rates further limited coverage.
Conclusion:
Improving vaccination requires expanding maternal education, increasing antenatal care access, and implementing mobile health services and awareness programs.
Keywords
Introduction
Immunization is one of the most cost-effective public health interventions, preventing an estimated 2 to 3 million deaths annually and contributing substantially to the reduction of child morbidity and mortality worldwide.1,2 Despite global progress, vaccination coverage remains inequitable, with persistent gaps in low- and middle-income countries (LMICs), particularly in fragile and conflict-affected settings.3,4 The World Health Organization (WHO) and partners have emphasized the importance of reaching underserved populations through the Immunization Agenda 2030 (IA2030), which calls for targeted strategies to address geographic, socioeconomic, and gender-related barriers to vaccination.1,5
Somalia faces profound challenges to achieving universal vaccination coverage due to protracted conflict, internal displacement, and weak health infrastructure.6 -8 National estimates indicate that coverage for basic childhood vaccines remains among the lowest globally, with wide disparities between urban, rural, and nomadic populations.8,9 The 2021 Galmudug Multiple Indicator Cluster Survey (GMICS) revealed substantial intra-state variation, with rural and nomadic households facing the greatest barriers to accessing routine immunization services.9,10
Several factors have been linked to low vaccination uptake in fragile states, including limited access to health facilities, vaccine stockouts, lack of maternal awareness, and sociocultural norms affecting healthcare utilization.11 -15 In Somalia, existing studies have identified maternal education, household wealth, and antenatal care (ANC) attendance as potential predictors of full immunization, but few have examined these factors within a health equity framework or disaggregated results by population type.16 -18
This study addresses these gaps by assessing the coverage, disparities, and associated factors for maternal and child vaccination in Galmudug State, Somalia, using GMICS 2021 data. The analysis examines differences by residence type (urban, rural, nomadic) and applies both descriptive methods to explore independent patterns of full vaccination. This study therefore aims to inform context-specific strategies for enhancing immunization coverage. The findings will contribute to Somalia’s national immunization program and help meet the targets of the Immunization Agenda 2030 by applying a health equity lens.
Despite ongoing efforts, vaccination coverage in Somalia—particularly in Galmudug State—remains below national and international targets, with persistent disparities across urban, rural, and nomadic populations. Structural constraints such as limited health facilities, vaccine stockouts, insecurity, and sociocultural barriers including awareness and mobility challenges impede access and continuity of care. This study descriptively examines maternal and child vaccination coverage and associated disparities by residence type, socioeconomic status, and maternal healthcare utilization, providing a baseline for equity-focused programing and future analytical work.
Methods
Study Design and Setting
This descriptive, cross-sectional study used secondary data from the 2021 Galmudug Health and Demographic Survey (GMHDS). The GMHDS is a population-based household survey conducted by the Somalia Ministry of Health in collaboration with UNICEF, designed to be representative of urban, rural, and nomadic populations. The survey provides comprehensive information on maternal and child health indicators, including vaccination coverage, antenatal care (ANC) utilization, and key sociodemographic determinants.
Galmudug State, located in central Somalia, comprises urban centers, rural villages, and nomadic pastoralist communities. The state’s estimated population in 2021 was approximately 2.5 million, with over one-third living in rural areas and about 25% classified as nomadic. Health service coverage is limited; fewer than 40% of settlements are within 5 km of a functioning health facility. Routine immunization services are provided through fixed health centers and outreach/mobile clinics, but vaccine stockouts and workforce shortages are frequent challenges.
Study Population and Sampling Design
The analysis included women aged 15 to 49 years who had at least 1 child aged 12 to 23 months at the time of the survey, considering only the most recent live birth for vaccination status assessment; children with incomplete vaccination data (missing both vaccination card and maternal recall) were excluded. The GMHDS employed a multistage stratified sampling design to ensure representativeness, utilizing a 3-stage selection process (enumeration areas, households, eligible women) in urban and rural areas, and a 2-stage design (temporary nomadic settlements, households) in nomadic areas. A total of 1741 households across 60 enumeration areas were sampled, covering 6 strata defined by urban, rural, and nomadic residency in both north and south Galmudug. Households absent during visits were replaced according to GMHDS protocols, with minimal refusals (<2%) accounted for in the sampling weights.
Study Variables
Outcome Variables
The primary outcome was “fully vaccinated” status, defined as a child having received all basic WHO-recommended vaccines (BCG, 3 doses of pentavalent vaccine, 3 doses of oral polio vaccine excluding the birth dose, and 1 dose of measles-containing vaccine) by 12 months of age. Vaccination status was ascertained using both health card records and caregiver recall when cards were unavailable. A secondary outcome was “partially vaccinated” status, defined as receipt of at least 1 but not all recommended vaccines. Dropout rates were calculated for selected antigens using the formula: (first-dose coverage − last-dose coverage)/first-dose coverage × 100.
Independent Variables
Independent variables included maternal sociodemographic characteristics (age, education, occupation, marital status), household characteristics (wealth quintile, residence type, distance to health facility), and maternal healthcare utilization indicators (ANC attendance, place of delivery, skilled birth attendance). Residence type was categorized as urban, rural, or nomadic per GMICS classification.
Conceptual Framework
The analysis was guided by the WHO Commission on Social Determinants of Health framework, adapted for immunization equity research, which conceptualizes vaccine uptake as influenced by structural determinants (eg, socioeconomic status, residence type) and intermediary determinants (eg, maternal health-seeking behavior, access to services).
Data Analysis
Descriptive statistics—including frequencies, percentages, and cross-tabulations—were used to summarize the distribution of vaccination coverage by sociodemographic and maternal healthcare utilization characteristics. Dropout rates for key antigens were calculated to assess vaccination continuity. All estimates were weighted to account for the complex survey design. Data analysis and visualizations (bar charts, pie charts, and line graphs) were conducted using Stata version 17.0 (StataCorp, College Station, TX). Given the study’s exploratory baseline aim, analyses were intentionally descriptive to profile equity gaps without making inferential claims. Resource and data-quality constraints common in fragile settings influenced this decision; consequently, multivariable models and concentration-index methods were not applied in this manuscript.
Ethical Approval and Informed Consent
This study analyzed publicly available, fully anonymized secondary data from the 2021 Galmudug Health and Demographic Survey (GMHDS). The GMHDS protocol was reviewed and approved by the Somalia Ministry of Health and Human Services Institutional Review Board (IRB). Because the dataset contains no personal identifiers, the need for additional ethical approval for this secondary analysis was waived by the same IRB. Written informed consent was obtained by GMHDS field teams from all respondents at the time of the original survey; consent was implicit in respondents’ voluntary participation. All analyses for the present study were conducted on anonymized records, with no attempt made to re-identify participants.
Results
Socio-Demographic and Healthcare Characteristics of the Study Population
A total of 1248 mother–child pairs were included in the analysis (Table 1). Most participants resided in rural areas (48.3%), followed by urban (34.1%) and nomadic (17.6%) settings. Nearly half of the mothers were aged 25 to 34 years (46.5%), with the majority having no formal education (71.2%) and being unemployed (58.4%). More than half (54.8%) reported attending at least 1 antenatal care (ANC) visit during their most recent pregnancy, and 38.7% delivered in a health facility. Wealth distribution was skewed toward the lowest quintiles in rural and nomadic households.
Background Characteristics of Women Aged 15 to 49.

Antenatal and Delivery Care Utilization
Overall, 54.8% of mothers attended at least 1 antenatal care (ANC) visit during their most recent pregnancy (Table 2). Attendance was highest in urban areas (68.9%), followed by rural (52.1%) and nomadic settings (37.4%). The proportion of women delivering in a health facility was 38.7% overall, with urban areas reporting 55.2%, rural areas 34.6%, and nomadic communities 19.3%. Skilled birth attendance showed a similar pattern, with an overall rate of 40.1%, ranging from 57.8% in urban settings to 21.7% in nomadic areas. These differences highlight geographic disparities in access to and utilization of maternal health services.
Antenatal and Delivery Care Utilization.

Table 2 presents ANC coverage disaggregated by residence type (urban, rural, nomadic), while Figure 1 visualizes ANC attendance by children’s vaccination status. Presenting both provides complementary perspectives—geographic differences in ANC uptake (Table 2) alongside the relationship between ANC attendance and full, partial, or zero vaccination status (Figure 1).

Proportion of ANC attendance.
Vaccination Coverage
Overall, 48.6% (95% CI: 45.5–51.7) of children were fully vaccinated, 36.4% (95% CI: 33.5–39.3) were partially vaccinated, and 15.0% (95% CI: 12.9–17.4) had not received any vaccines (Table 3). Among fully vaccinated children, 63.5% had documented vaccination cards, while 36.5% relied on caregiver recall. Coverage was highest in urban areas (61.3%), followed by rural (44.8%) and nomadic (29.5%) settings. Descriptive trends indicated that vaccination coverage increased with maternal education—from 42.7% among mothers with no education to 64.2% among those with secondary or higher education. In addition to full vaccination, partial vaccination represented a substantial share of outcomes. Partial coverage was more common among rural and nomadic households than urban households and among mothers with fewer antenatal care contacts. These patterns highlight persistent gaps in continuity of the vaccination schedule, even when initial contact is achieved (Figure 2).
Coverage of Individual Vaccines Among Children Aged 12 to 23 months.

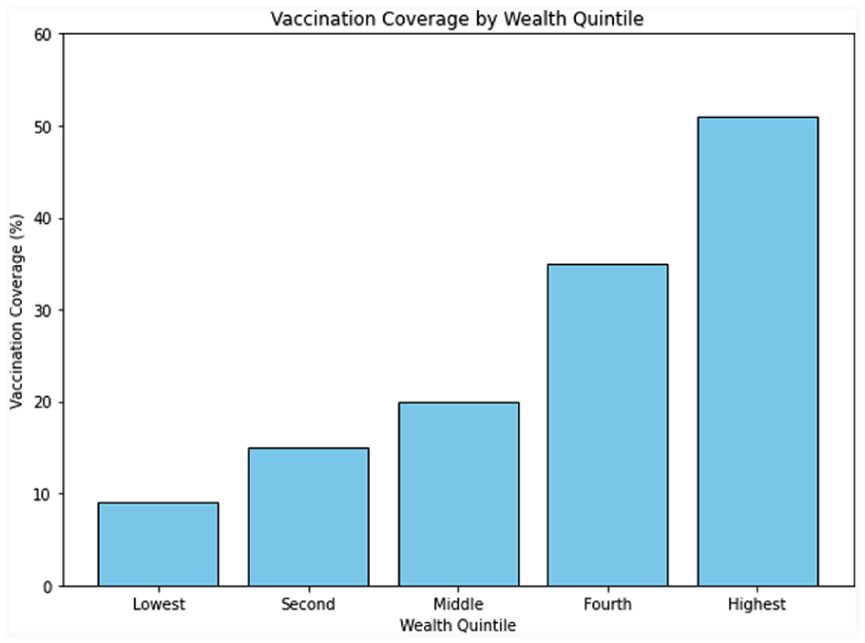
Vaccination coverage by wealth.
Regional and Geographic Disparities
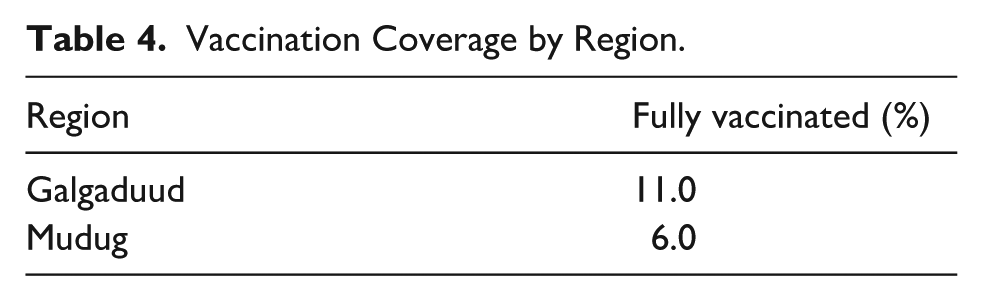
Significant geographic disparities were observed, with full vaccination rates being highest in urban areas (14%) and lowest among nomadic populations (2%; Figure 3). Regional variations were also evident, with Galgaduud achieving an 11% full vaccination rate compared with 6% in Mudug (Table 4).

Vaccination coverage by residence type.
Vaccination Coverage by Region.
Disparities in Coverage
The descriptive analysis revealed substantial inequalities in vaccination coverage by socioeconomic status, maternal healthcare utilization, and place of residence (Table 4). In urban areas, the gap between the highest and lowest wealth quintiles was 22 percentage points (72.4% vs 50.4%), while among nomadic populations the gap widened to 28 percentage points (43.5% vs 15.5%). Coverage varied considerably by geographic subgroup, ranging from above 70% in the highest-performing urban areas to below 15% in the lowest-performing nomadic settlements, with some small settlements recording coverage levels of less than 5%. Maternal healthcare use was strongly associated with higher coverage: 61.8% of children whose mothers attended at least 1 ANC visit were fully vaccinated, compared to 35.2% among those whose mothers received no ANC.
Dropout Rates Between Vaccine Doses
Dropout from the first to the third dose of pentavalent vaccine was 18.7%, while dropout between Bacillus Calmette–Guérin (BCG) and measles-containing vaccine was 21.4% (Figure 4). Dropout rates were consistently higher in nomadic populations compared to rural and urban households, suggesting that follow-up challenges and mobility may hinder completion of the vaccination schedule.

Dropout rates for the immunization schedule.
Discussion
This study provides a descriptive overview of maternal and child vaccination coverage in Galmudug State, Somalia, revealing persistent inequalities across geographic, socioeconomic, and maternal healthcare utilization dimensions. The findings are consistent with earlier evidence showing that children in rural and nomadic communities experience markedly lower coverage compared to urban counterparts due to barriers such as distance from health facilities, insecurity, and mobility constraints.7,19,20 Nomadic populations, in particular, often lack sustained access to fixed immunization services, echoing patterns reported in other pastoralist settings within the Horn of Africa, including Ethiopia’s Somali Region, cross-border communities in Kenya and Nigeria, and fragile areas within Somalia such as Mogadishu, where studies have highlighted high prevalence of missed opportunities for vaccination.9,21 Such populations often experience disruption in health service continuity due to seasonal migration n, compounded by limited health infrastructure and challenging terrain.6,8
The strong positive association between antenatal care (ANC) attendance and full vaccination aligns with evidence from Somalia and other low-resource settings demonstrating that ANC provides a critical platform for linking mothers to child immunization services.19,20,22 In Galmudug, however, ANC coverage remains low—especially among nomadic and rural mothers—reflecting broader systemic and cultural barriers documented in fragile contexts, including limited service availability, costs associated with transport, and social norms that may discourage facility attendance.7,19 Integrating immunization services into ANC visits, as recommended by WHO and national immunization strategies, could help bridge service gaps for these populations.1,2,23
Dropout rates between early and later vaccine doses were notable, particularly between BCG and measles. Similar trends have been observed in other conflict-affected or pastoralist regions, where logistical challenges, seasonal migration, and weak follow-up mechanisms contribute to incomplete schedules.19,20,24 In Galmudug, cold chain interruptions, health worker shortages, and insecurity in hard-to-reach settlements likely exacerbate these patterns.7,19 Strategies such as mobile vaccination teams, flexible outreach schedules, and improved tracking systems could help reduce dropouts, especially among nomadic communities.9,23,24
Beyond structural barriers, socio-cultural dynamics—including gender norms and women’s decision-making autonomy—are important determinants of service uptake in Somalia. Similar findings in Nigeria have shown that maternal autonomy and attitudes toward gender norms are strongly associated with childhood immunization.25 -27 Male-dominated household decision-making, competing domestic responsibilities, and cultural expectations around maternal mobility may limit mothers’ ability to attend both ANC visits and immunization appointments.7,19,28 Evidence from other parts of the Horn of Africa indicates that targeted community engagement, involvement of male household heads, and women’s empowerment initiatives can improve vaccination uptake9,10,30
Geographic disparities observed in this study are consistent with reports from other fragile states such as Chad, South Sudan, and Afghanistan, where residence, wealth, and maternal service utilization strongly influence vaccination coverage. In Somaliland, analysis of the 2020 DHS similarly found that maternal education and ANC attendance were key drivers of vaccination uptake.29 -32 However, Somalia’s high proportion of nomadic populations presents distinct delivery challenges that require tailored approaches. In addition to mobile vaccination teams, integrating immunization with broader maternal and child health outreach—such as nutrition screening, deworming, and antenatal services—can enhance service uptake and cost-effectiveness.19,23,33
From a policy perspective, these findings align with the Somalia National Immunization Strategy 2022 to 2026 and the Immunization Agenda 2030.1,2,33 Equity-focused interventions should prioritize underserved nomadic and rural populations, with targeted resource allocation, service delivery innovations, and culturally sensitive health promotion campaigns. For nomadic communities, service delivery models should account for migratory patterns and seasonal settlement locations.9,19 For rural populations, expanding fixed-post outreach, improving transport infrastructure, and enhancing health worker availability are critical.5,7,23
Community engagement strategies are equally vital. Demand-generation activities that address misinformation, leverage trusted local leaders, and engage women’s groups can strengthen vaccine confidence and acceptance.6,28 Integrating gender-sensitive approaches into vaccination campaigns can ensure that women are not only recipients but also active decision-makers and advocates for child health within their households and communities.7,28
Conclusion
This study highlights persistent inequities in maternal and child vaccination coverage in Galmudug State, Somalia, with particularly low rates among nomadic populations and households in the lowest wealth quintiles. The strong association between maternal healthcare utilization and vaccination underscores the need to integrate immunization services with antenatal and postnatal care platforms. Addressing these gaps will require targeted, equity-focused interventions such as mobile vaccination teams for nomadic groups, expanded community-based delivery points, and culturally sensitive health promotion addressing gender and decision-making barriers. These findings align with the priorities outlined in Somalia’s National Immunization Strategy 2022 to 2026 and the Immunization Agenda 2030, and underscore the urgency of tailored approaches to ensure no child is left behind.
Limitations
This study has several limitations. First, the use of secondary data from the GMHDS 2021 limited the analysis to variables collected in the survey, potentially omitting other important determinants of vaccination coverage. Second, vaccination status was determined via both vaccination card verification and maternal recall; the latter is prone to recall bias, which may have led to misclassification of coverage status. Third, the cross-sectional design precludes causal inference between explanatory factors and vaccination outcomes. Fourth, although the analysis highlights associations between maternal healthcare utilization, socioeconomic status, and coverage, no inferential statistical models were applied, restricting the ability to adjust for confounding factors. Finally, nomadic and hard-to-reach populations may have been underrepresented despite efforts in the survey’s sampling strategy, potentially biasing estimates downward for these groups.
Future studies should employ longitudinal designs, qualitative inquiry, and inferential equity-focused analyses (eg, regression and concentration indices) to better understand and address the drivers of vaccination disparities in Somalia and to test the observed patterns for targeted interventions.
Footnotes
Acknowledgements
The authors acknowledge the Somalia National Bureau of Statistics for providing the data available for this study.
Authors’ Note
Abdihakim Elmi Abdishakur is now affiliated to Hodan Hospital, Mogadishu, Somalia.
Ethical Considerations
This study analyzed publicly available, fully anonymized secondary data from the 2021 Galmudug Health and Demographic Survey (GMHDS). The GMHDS protocol was reviewed and approved by the Somalia Ministry of Health and Human Services Institutional Review Board (IRB). Because the dataset contains no personal identifiers, the need for additional ethical approval for this secondary analysis was waived by the same IRB.
Consent to Participate
Written informed consent was obtained by GMHDS field teams from all respondents at the time of the original survey; consent was implicit in respondents’ voluntary participation. All analyses for the present study were conducted on anonymized records, with no attempt made to re-identify participants.
Author Contributions
AA and SH conceptualized the study, designed the methodology, performed data analysis, visualized the results, and wrote the manuscript. MMA, AMM and MDH contributed by providing critical reviews and editing the manuscript. JS offered additional insights and technical support during the manuscript preparation. All authors have reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Clinical Trial Number
Not applicable.