
Abstract
Background:
Congenital abnormalities are a major cause of infant mortality, impacting healthcare and quality of life. This study analyzed trends in incidence and mortality from 1990 to 2021 using secondary data.
Methods:
An ecological study was conducted using the 2021 Global Burden of Disease dataset. Joinpoint regression analysis examined trends, while ArcMap GIS and the Moran I test assessed spatial distribution.
Results:
Mortality rates declined annually by 6.3% in males and 4.2% in females, while incidence rates decreased by 0.5% and 0.9%, respectively. Hot spots for incidence in 2021 were Sistan and Baluchestan and Khorasan Razavi, while Kerman had the highest neonatal mortality.
Conclusion:
Incidence and mortality of congenital abnormalities are decreasing in Iran, but eastern provinces remain high-risk areas.
Introduction
Congenital abnormalities are a range of structural or functional malformations that can be diagnosed before birth, at birth, or in later stages of life.1,2 Congenital abnormalities are the main cause of infant mortality and can have a significant impact on the health care system and the quality of life of the individuals and families. For instance, mothers of newborns with major congenital abnormalities demonstrated a higher utilization of healthcare resources, and following the delivery of an impacted offspring, the utilization of psychiatric services rose by 13 years.3 -5 Globally, after controlling child mortality due to infectious diseases, deaths caused by congenital abnormalities have been increasing. 6
Worldwide, about 6% of newborns had some kind of congenital abnormalities, and every year more than 170 000 children die between 1 and 59 months due to congenital abnormalities. 7 In 2019, congenital abnormalities were introduced as the fourth leading cause of death for children under 5 years of age. 8 Congenital heart malformation is the second cause of death in infancy the main cause of death in children under 5 years of age and the third cause of death in children aged 5 to 14 years. 9
Since deaths due to congenital abnormalities occur early in life, years of life lost (YLL) increase. 10 Studies have shown that these abnormalities occur more often in countries with lower socio-economic status and are considered one of the important causes of infant mortality in these countries.11 -13
A wide range of factors, including environmental, genetic, and social factors can cause congenital abnormalities.14,15 Also, studies have shown the effect of factors such as family marriages, contraceptive methods, alcohol and smoking during pregnancy, family history of genetic disorders, and mother’s age in the occurrence of congenital abnormalities.16 -20 In Iran, in the city of Tabriz between 2000 and 2011, the prevalence of congenital abnormalities was estimated to be 202.3 per 10 000 births. 21
Since no study has examined the incidence and mortality of congenital abnormalities in Iran, and due to the lack of information hindering effective health policies, this study aims to investigate the incidence of congenital abnormalities at birth and the mortality of congenital abnormalities in Children under 28 days in Iran during 1990 to 2021 was designed using secondary data.
Method
Study Design & Data Access
This ecological study was conducted by using the Global Burden of Disease (GBD) study last version dataset (2021). This resource is freely accessible to all researchers and offers estimates for various metrics including incidence and mortality. These metrics are available for both genders and across different age groups, enabling comparisons over the period from 1990 to 2021. 22
data on the incidence and death rates of congenital abnormalities were collected from 1990 to 2021. The data was categorized by sex and focused on both Iran as a whole and its individual provinces. Incidence data pertained to cases occurring at birth, while death data included cases within the first 28 days of life.
Congenital Abnormalities
Congenital abnormalities are abnormalities in body structure or function that originate prenatally and may be visible at birth or remain hidden. 23 This study encompasses a range of conditions such as neural tube defects, congenital heart anomalies, orofacial clefts, Down syndrome, Turner syndrome, Klinefelter syndrome, other chromosomal abnormalities, congenital musculoskeletal and limb anomalies, urogenital congenital anomalies, digestive congenital anomalies, and various other congenital abnormalities (The corresponding ICD-10 codes for these conditions are provided at the end of the manuscript).
Statistical Analyses
To investigate the trends in the incidence and mortality rates associated with congenital abnormalities from 1990 to 2021, we employed Joinpoint regression analysis using the Joinpoint Regression Program. In this approach, we utilize the annual incidence and mortality rates for the specific disease, along with the standard error (SE) as inputs for the model. We then calculate the annual percentage change (APC) with a 95% confidence interval for years exhibiting a change in trend. Additionally, we estimate the average annual percentage change (AAPC) for both genders in diverse geographic regions.
The model is based on the equation

Connection points, representing years with trend changes, are identified, and the significance of these trends is determined using the Monte Carlo permutation method. This allows us to assess the trend changes between these points and evaluate their statistical significance.
Furthermore, we employed ArcMap GIS software and the Moran I test to analyze the spatial distribution and geographical correlations.
Results
Trend Analysis
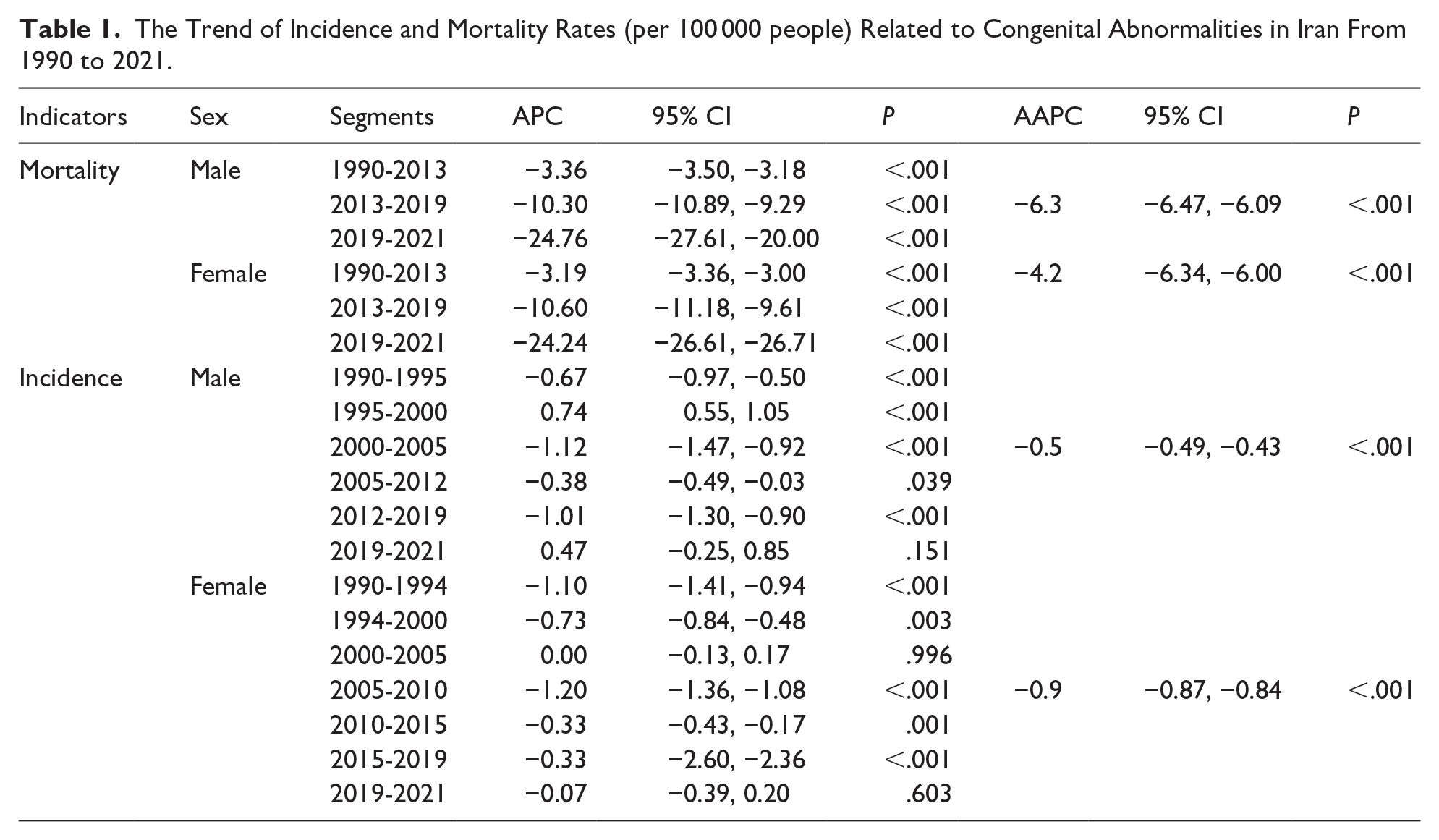
The AAPC in mortality from congenital abnormalities showed an annual decrease of 6.3% for males and 4.2% for females. Additionally, the AAPC in the incidence of congenital abnormalities decreased by 0.5% for males and 0.9% for females.
Table 1 presents the details of the AAPC and the APC, while Figure 1 illustrates the trends in incidence and mortality due to congenital abnormalities. Table 2 also shows the values of the AAPC related to the occurrence and mortality of this disease in the provinces.
The Trend of Incidence and Mortality Rates (per 100 000 people) Related to Congenital Abnormalities in Iran From 1990 to 2021.

(a) Incidence rate in female, (b) incidence rate in male, (c) mortality rate in female, and (d) mortality rate in male.
The Trend of Incidence and Mortality Rates (per 100 000 People) Related to Congenital Abnormalities Across the Provinces of Iran From 1990 to 2021.

Geographical Distribution
Based on the data, the incidence of congenital abnormalities in 2021 in Iran was approximately 4413 and 5426 per 100 000 individuals for females and males, respectively. Additionally, the mortality rate in 2021 in Iran was around 885 and 1131 per 100 000 individuals for females and males, respectively.
In 2021, the most common cause of death among both males and females was linked to cardiac issues. Additionally, the greatest occurrence rates in females and males that year were associated with heart problems and congenital musculoskeletal and limb anomalies, respectively.
Figures 2 and 3 provide a detailed overview of the geographical distribution of the incidence and mortality rates associated with congenital anomalies, highlighting hot spots and geographical correlations.
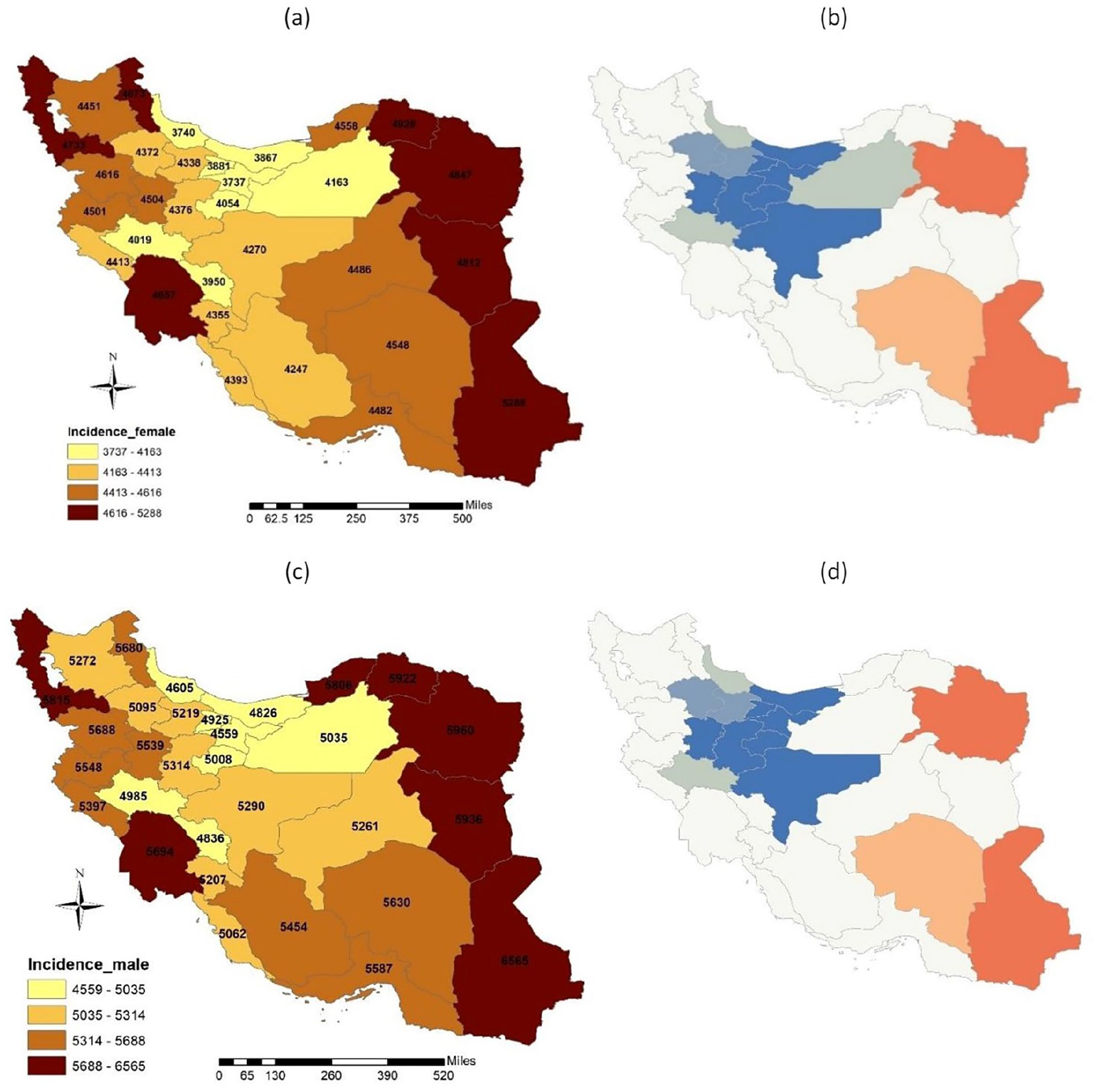
(a) incidence rate in female, (b) geographical correlation for incidence rate in female with P-value: <.001 and Z-score: 4.48, (c) incidence rate in male, d:) geographical correlation for incidence rate in male with P-value: <.001 and Z-score: 4.32.

(a) mortality rate in female, b:) geographical correlation for mortality rate in female with P-value: <.001 and Z-score: 3.51, (c) mortality rate in male, (d) geographical correlation for mortality rate in male with P-value: <.001 and Z-score: 3.16.
The hot spots for the incidence rate in 2021 for both males and females included the provinces of Sistan & Baluchestan as well as Razavi Khorasan, while the cold spots included Tehran, Isfahan, Qom, Mazandaran, Alborz, Hamadan, and Markazi.
For the death rate due to this disease in children under 28 days in 2021, the hot spot for both males and females was Kerman province. The cold spots for males included Hamedan, Markazi, Qom, Tehran, Alborz, and Qazvin provinces, while for females, the cold spots included Hamadan, Qom, Markazi, and Tehran provinces.
Discussion
Congenital abnormalities can increase neonatal mortality rates. 24 They stand as the primary reason for infant deaths in the United States and rank fourth globally, causing around 295 000 deaths each year. 25 Several studies have highlighted the substantial occurrence and fatality of congenital abnormalities, notably during the COVID-19 pandemic in Iran.26 -28 In Iran, the expansion of healthcare coverage, with 90% of the population now covered by insurance, has significantly improved access to medical services. Additionally, increased health literacy and awareness among women have contributed to better health outcomes and a reduction in congenital abnormality related morbidity and mortality.29,30 This study showed an overall decrease in the morbidity and mortality rates of congenital anomalies among both sexes in Iran, likely due to the aforementioned factors as well as the decline in birth rates (Table 3).
The Trend of Live Births in Iran During 1990 to 2021.

Only a limited number of studies conducted in Iran have explored the prevalence of congenital abnormalities, yielding conflicting findings. One instance is a study from northern Iran employing the Tabriz Congenital Abnormalities Registration Program (TRoCA), which documented a rise in these conditions between 2000 and 2020. Conversely, research in Shahrekord indicated a decline in congenital hypothyroidism cases from 2006 to 2014.31,32 Additionally, investigations in Chongqing noted a downward trend in these ailments from 2007 to 2020, while a study in Ethiopia observed an uptick in cases from 2017 to 2019.33,34
Research indicates a strong connection between parental consanguinity and the presence of congenital abnormalities. 35 Our study highlighted that the highest rate of such conditions was found in Sistan and Baluchistan province. This trend can be attributed to cultural norms, ethnic factors, and limited access to screening services in the region. This aspect could not be examined in this descriptive study, highlighting one of its limitations.
Just like our research, several studies have indicated that the primary form of congenital abnormality is associated with cardiac malformations.7,36 A research conducted in South Africa in 2018 revealed a central birth prevalence rate of 15.57 per 1000 live births for congenital abnormalities, with the musculoskeletal system (32%) being the most commonly affected, followed by circulatory system malformations (19%). 37 Similarly, a study in Santa Catarina found that the average prevalence of congenital abnormalities during the same period was 8.9 per 1000 live births, slightly increasing from 9.4 per 1000 live births in 2010 and 8.2 per 1000 in 2018. 38
In a meta-analysis conducted in 2020, it was found that there has been a notable increase in the survival rates of children with specific birth defects in recent years. Additionally, a study in the United States revealed a declining trend in the mortality rates associated with congenital heart defects from 1999 to 2017.39,40
This study provides an important overview of the current status of congenital anomalies in Iran, highlighting trends in incidence and mortality. Given the high prevalence of consanguineous marriages, the aging population, and recent national policies promoting higher birth rates, monitoring congenital anomalies is crucial for healthcare planning and preventive strategies. Understanding these trends can help policymakers and healthcare providers develop targeted interventions to reduce the burden of these conditions. However, as a descriptive study, this research is limited in establishing causal relationships, and further analytical studies are needed to explore the underlying determinants of these trends.
Conclusion
This research showed that, overall, there is a decreasing trend in the incidence and mortality rates of congenital anomalies in both females and males in Iran. The hot spots for occurrence and death caused by these anomalies are concentrated in the east of Iran. For a more detailed analysis, future studies are recommended to investigate the subsets of congenital anomalies more deeply.
ICD-10 Codes for Congenital Abnormalities
The following table provides the ICD-10 codes for the congenital abnormalities discussed in this study:
Neural tube defects: Q00-Q01.9, Q05-Q05.9, Q07.01, Q07.03
Congenital heart anomalies: Q20-Q27, Q27.1-Q28.9
Orofacial clefts: Q35-Q37.9
Down syndrome: Q90-Q90.9
Turner syndrome: Q96-Q96.9
Klinefelter syndrome: Q98-Q98.9
Other chromosomal abnormalities: Q74.8, Q75.1, Q75.4, Q75.8, Q79.6, Q87-Q87.89, Q91-Q93.9, Q95, Q95.9, Q97-Q97.9, Q99-Q99.9
Congenital musculoskeletal and limb anomalies: Q65-Q65.2, Q65.8-Q66.1, Q68, Q68.1-Q68.2, Q68.6-Q74, Q74.1-Q74.5, Q74.9-Q75.0, Q75.5-Q76, Q76.1-Q76.49, Q76.8-Q79, Q79.8-Q79.9
Urogenital congenital anomalies: P96.0, Q50-Q52.2, Q52.4, Q52.6-Q52.9, Q54-Q55.2, Q55.22-Q57, Q64-Q64.19
Digestive congenital anomalies: Q38-Q38.0, Q38.3-Q38.4, Q38.6-Q43, Q43.1-Q45.8, Q79.0-Q79.59
Other congenital abnormalities: G71.2, Q02-Q04.9, Q06-Q07.0, Q07.9, Q10-Q15.9, Q17-Q18.9, Q27.0, Q30-Q34.9, Q38.1-Q38.2, Q38.5, Q39.0, Q41.9, Q53.0-Q53.9, Q56.20-Q56.21, Q63.3, Q65.3-Q65.6, Q66.2-Q67.8, Q68.0, Q68.3-Q68.8, Q74.0, Q75.2-Q75.3, Q76.0, Q76.5-Q76.7, Q80-Q86.8, Q89-Q89.8, Q95.0-Q95.11
Footnotes
Acknowledgements
The authors appreciate the Vice-Chancellor of Research of Shahid Sadoughi University of Medical.
Ethical Considerations
This study was supported by Shahid Sadoughi University of Medical Sciences (Ethical code: IR.SSU.SPH.REC.1403.119)
Author Contributions
MTS: Conception and design. MK and MA: provision of study materials and collection of data. MK and MTS: Data analysis and interpretation. MTS serves as the lead author and guarantor. All the authors contributed to the research and agreed to be responsible for all aspects of this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.