
Abstract
Objective
The association between comorbidities and inpatient mortality with sudden sensorineural hearing loss (SSNHL) has not been investigated. Therefore, this study aimed to provide a 14-year nationwide incidence, and identify risk factors and comorbidities of SSNHL inpatient mortality.
Methods
Data were obtained from the Taiwan National Health Insurance Research Database for 2000 to 2013. Inpatient mortality of 31,258 patients hospitalized with a diagnosis of SSNHL was recorded and analyzed.
Results
Sixteen patients with SSNHL exhibited mortality with a percentage of 0.05% and an incidence of less than 0.01 per 100,000 people per year. The risk of variables among inpatient mortality was associated with older age (adjusted odds ratio [OR]: 1.042, 95% confidence interval [CI]: 1.009–1.077) and the presence of catastrophic illness (adjusted OR: 4.949, 95% CI: 1.290–18.996). Potential comorbidities included hematologic diseases, cancers, chronic hepatitis, gastrointestinal bleeding, chronic obstructive pulmonary disease, seizures or convulsions, coronary artery disease, diabetes mellitus, and varicose veins and their associated complications.
Conclusions
This 14-year nationwide study shows that inpatient mortality rate for SSNHL is relatively rare, but suggests we should still be aware of the potential for such underlying conditions to cause SSNHL as well as the mortality associated with these conditions.
Introduction
Sudden sensorineural hearing loss (SSNHL) is a unique and enigmatic disorder defined as a >30 dB sensorineural loss over three contiguous frequencies occurring within 3 days. 1 SSNHL commonly affects only one ear, and 70% of cases are idiopathic. 2 Therefore, the treatment has multiple therapeutic modalities based on specific etiopathological theories including vascular, viral, autoimmune, traumatic, and stress-induced events. Based on a nationwide survey over 14 years, we previously reported that the incidence of inpatient SSNHL has increased gradually during this time. 3 The incidence of inpatient SSNHL from 2000 to 2013 was 9.76 per 100,000 people per year. Men were more commonly affected than women, and hospitalized patients with SSNHL most commonly presented in the age group of 45 to 64 years.
This survey also showed that some patients had mortality with a coexisting diagnosis of inpatient SSNHL. Although SSNHL itself is not fatal, some case reports suggest that death occurred in relation to SSNHL.4–8 For example, Ogino-Nishimura et al. 4 reported death from a pheochromocytoma crisis caused by systemic corticosteroids used in the treatment of patients with SSNHL. Adams et al. 5 described three cases of malignant meningitis from undiagnosed esophageal cancer which presented with SSNHL, causing rapid patient death, while Greene et al. 6 suggested that paraneoplastic syndrome may be a masquerade of autoimmune inner ear disease related to SSNHL. Sanecka et al. 7 advocated the risk of sudden cardiac death in patients with hearing loss through early diagnosis of Jervell and Lange–Nielsen syndrome. Arnold and Vosteen reported the death of a patient from a subarachnoid hemorrhage after experiencing sudden hearing loss in her right ear caused by a large aneurysm of the basilar artery, 8 while Ito et al. 9 documented a case of life-threatening pyogenic ventriculitis, complicating endocarditis, presenting as sudden hearing loss. Because most SSNHL patients first seek medical help in an otorhinolaryngological department, we should be aware of these underlying coexisting and catastrophic diseases.
To our knowledge, no large-scale study has previously addressed the association between comorbidities and inpatient mortality with SSNHL. Therefore, in this study, we analyzed the Taiwanese nationwide database to investigate the incidence and potential comorbidities in SSNHL patients with mortality over a 14-year period.
Materials and methods
Data sources
The present study used data from the National Health Insurance Research Database (NHIRD) to investigate inpatient mortality in patients with SSNHL over a 14-year period using the inpatient Longitudinal Health Insurance Database in Taiwan (2000–2013).
Study design and sampled participants
This retrospective cross-sectional study enrolled patients who were hospitalized with a diagnosis of SSNHL (ICD-9-CM: 388.2) during 2000 to 2013. We excluded patients with missing information regarding age and sex. A total of 31,258 patients were enrolled in this study, and the inpatient mortality was recorded and analyzed.
Potential confounding variables
We considered variables believed to affect the survival and mortality of inpatients with sudden hearing loss—namely sex, age, catastrophic illness, urbanization level, surgery and level of medical care—as potential confounders. We defined catastrophic illness using the definition of the Ministry of Health and Welfare in Taiwan, which contains 30 categories that include cancer, hematological abnormality (coagulopathy, anemia), renal failure, generalized autoimmune diseases, chronic mental disorders, congenital metabolic disorders, major organ abnormality, massive burns, major organ transplantation, complicated nervous or musculoskeletal disorders, an injury severity score more than 16, respiratory failure, uncorrected malnutrition status, myasthenia gravis, spinal cord injuries, occupational diseases, cerebro-vascular diseases (acute stage), multiple sclerosis, leprosy, complicated liver cirrhosis, toxic effects of arsenic and its compounds, Creutzfeldt–Jakob disease, and rare diseases. 10 We also considered the following comorbidities: diabetes mellitus (ICD-9-CM: 250) [DM], hypertension (ICD-9-CM: 401–405) [HT], depression (ICD-9-CM: 296.2, 296.3, 296.82, 300.4, and 311), insomnia (ICD-9-CM: 780.52), stroke (ICD-9-CM: 430–438), chronic kidney disease (ICD-9-CM: 585) [CKD], osteoporosis (ICD-9-CM: 733.00–733.09), anemia (ICD-9-CM: 280–285), hyperlipidemia (ICD-9-CM: 272), and systemic lupus erythematosus (ICD-9-CM: 710.0) [SLE].
Statistical analysis
All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Categorical and continuous variables were evaluated using the chi-squared test, Fisher’s exact test, or t test, as appropriate. Poisson regression was used to identify the risk factors for inpatient mortality, and the results are presented as odds ratios (ORs) and 95% confidence intervals (CIs).
Ethics statement
The NHIRD provides encrypted patient identification numbers associated with relevant claims information. All analyzed data were devoid of identifiable personal information, so patient consent was not required to access the NHIRD. The Institutional Review Board of Tri-Service General Hospital approved this study (TSGHIRB No. 2-104-05-126) and waived the requirement of informed consent.
Results
Data from 2000 to 2013 revealed 31,258 cases (31,242 survival vs 16 mortality) of hospitalized patients with SSNHL in Taiwan. Patient characteristics are listed in Table 1. Overall, 16 patients with SSNHL exhibited inpatient mortality (12 men, four women; 0.05%), representing an incidence of less than 0.01 per 100,000 people per year. The mean age of the inpatient mortality group was 60.14 ± 18.01 years and that of the survival group was 50.29 ± 16.70 years (p = 0.018). There were higher percentages of men (75% vs 53.5%), patients aged >65 years (50% vs 20.6%), catastrophic illness (25% vs 2.6, p = 0.001%), and anemia (12.5% vs 1, p=0.012%) in SSNHL patients with mortality compared with those who survived. There were no significant differences in DM, HT, depression, insomnia, stroke, CKD, osteoporosis, hyperlipidemia, or SLE between the two groups. Approximately 94.7% of SSNHL patients who survived were hospitalized in the ENT department, compared with 43.8% of those with mortality (p < 0.001). Significantly longer hospitalized days (8.38 ± 10.27 vs 5.64 ± 2.88 days, p < 0.001) and higher costs (2880 ± 5146 vs 681 ± 676 USD, p < 0.001) were associated with SSNHL patients with mortality compared with those who survived.
Characteristics of patients with sudden sensorineural hearing loss.
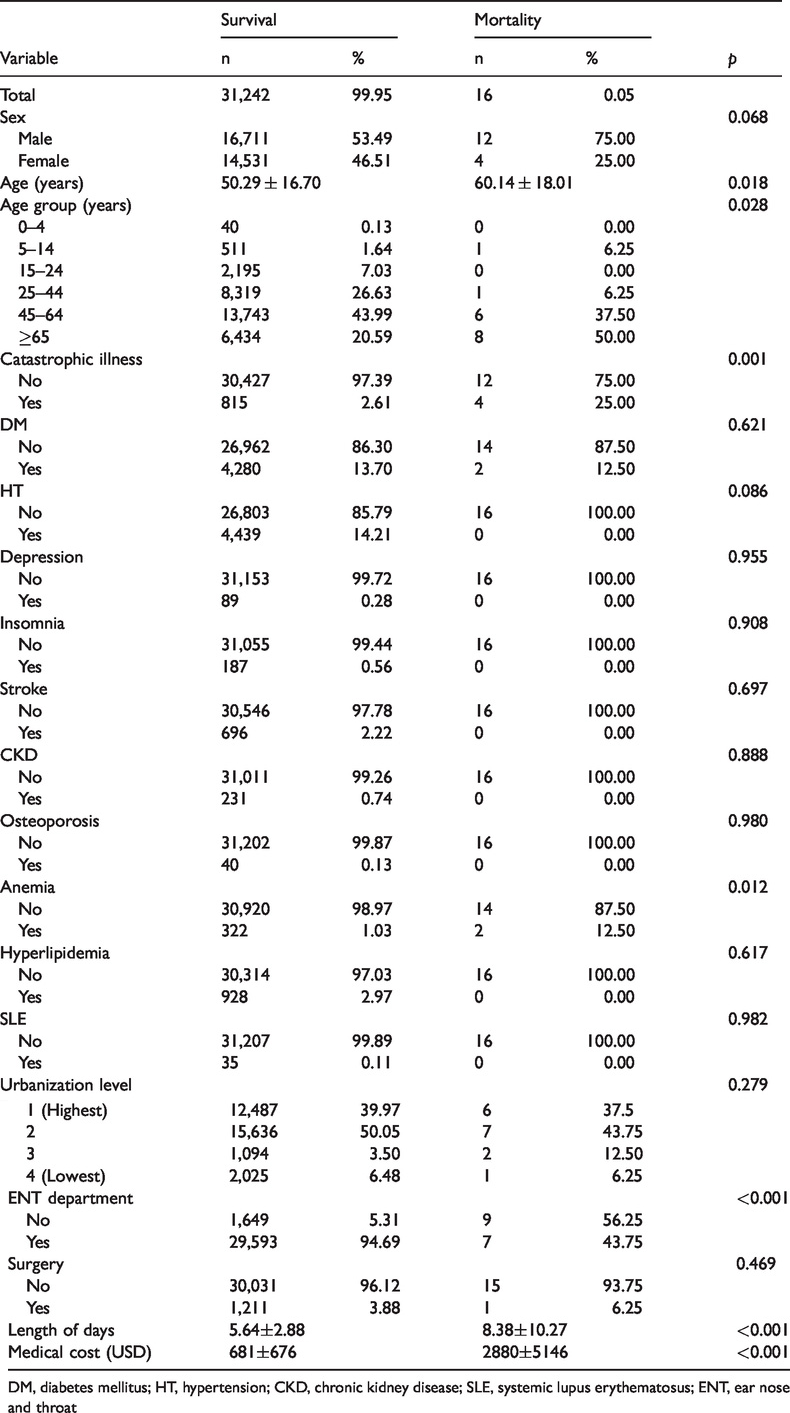
DM, diabetes mellitus; HT, hypertension; CKD, chronic kidney disease; SLE, systemic lupus erythematosus; ENT, ear nose and throat
Poisson regression with multivariate adjustment was used to evaluate the risk factor of inpatient mortality in SSNHL patients (Table 2). This revealed that the risk of variables among inpatient mortality with SSNHL is associated with older age (adjusted OR: 1.042, 95% CI: 1.009–1.077) and the presence of catastrophic illness (adjusted OR: 4.949, 95% CI: 1.290–18.996). A reduction in the risk of variables among inpatient mortality with SSNHL was shown to be associated with admission to the ENT department (adjusted OR: 0.056, 95% CI: 0.017–0.186). No significant differences in sex, urbanization level, level of hospital, surgery event, or other comorbidities were observed.
Poisson regression factors of mortality in patients with sudden sensorineural hearing loss.

OR, odds ratio; CI, confidence interval; DM, diabetes mellitus; ENT, ear, nose and throat
Adjusted OR: all variables listed in Table 1 were adjusted.
Details of SSNHL inpatient mortality are presented in Table 3. Of 16 mortalities, 12 occurred within 1 week of hospitalization. Eight patients older than 65 years, six patients from the 45- to 64-year age group, one 28-year-old patient, and one 12-year-old patient died. The various comorbidities and etiologies included hematologic diseases, cancers, chronic hepatitis, gastrointestinal (GI) bleeding, chronic obstructive pulmonary disease, seizure or convulsion, coronary artery disease, DM, and varicose veins and their associated complications such as organ failure. However, two patients (one 48-year-old woman and one 55-year-old man) with otologic diagnoses only (sudden hearing loss and tinnitus) died on the sixth day of hospitalization.
Details of mortality in patients with sudden sensorineural hearing loss.

*Included in the catastrophic illness defined by the Ministry of Health and Welfare, Taiwan.
Discussion
To the best of our knowledge, this is the first large-scale survey to indicate the incidence of inpatient mortality and potential comorbidities in patients with SSNHL from 2000 to 2013 in Taiwan. Taiwan’s National Health Insurance (NHI) is a single-payer compulsory health insurance policy launched in 1995 that covered >99.5% of the 23.74 million Taiwanese citizens in 2014; data from the NHI serve as a database with high validity and integrity to achieve accurate epidemiological estimates and in-hospital mortality.3,11
SSNHL patient mortality is relatively rare and barely reported. Chau et al. 2 has reviewed the etiology in adult SSNHL which commonly affects unilateral SSNHL, although 70% of SSNHL is idiopathic. Additionally, rapidly progressive hearing loss is often unilateral initially, but then progresses to bilateral involvement. 12 Therefore, the mortality of patients with unilateral SSNHL would be expected to be extremely rare, 12 yet Sara et al. 13 reported an overall mortality rate of 15.5% in bilateral SSNHL patients. In our present study, 16 cases of inpatient mortality (12 men, and 4 women) were identified, with an estimated mean mortality rate of 0.05% and a mortality incidence of less than 0.01 per 100,000 person-years. Table 2 shows that the risks of variables among inpatient mortality are associated with older age and the presence of catastrophic illness.
No previous reports have investigated the association between SSNHL and mortality in older individuals, although some have studied that between hearing impairment and mortality.14,15 Karpa et al. 14 indicated that hearing loss is associated with an increased risk of mortality through mediating variables, including disability in walking and self-rated health in older individuals. Fisher et al. 15 reported that older men with hearing impairment had a greater risk of dying from any cause, and particularly cardiovascular causes, within a median 5-year follow-up time. Catastrophic illness is not a common comorbidity, occurring in only 2.6% of SSNHL patients who survived, but was associated with a risk of variables among inpatient mortality as shown in Table 1. 3 In our report, seven out of 16 (43.8%) mortality cases with SSNHL had at least one catastrophic illness as shown in Table 3. A reduced risk of variables among inpatient mortality with SSNHL was associated with admission to the ear, nose and throat (ENT) department (adjusted OR: 0.056, 95% CI: 0.017–0.186). This suggests that patients admitted to departments other than ENT presented with more severe underlying comorbidities that led to mortality.
Based on Table 3 details of inpatient mortality, we surmise that most patients died from their severe underlying comorbidities, and that SSNHL was merely one of the manifestations in patients with mortality. This echoes why a higher mortality rate was observed in patients admitted to departments other than ENT, those with longer hospital stays, and those with higher medical costs. Coronary artery disease or DM were observed in three patients (cardiovascular diseases); vital organ failure, GI bleeding, and shock were observed in seven patients (unstable hemodynamics); and cancer and hematologic disease were found in six patients (hypercoagulability condition).16–19 However, there is still some causality that cannot be fully interpreted by the diagnoses alone. Two cases with a diagnosis of sudden hearing loss with or without tinnitus died on the sixth day of hospitalization. Given the lack of further evidence, we speculate that they died from complications of treatment or some undiagnosed or related diseases.8,20
We summarize the three possible causes of mortalities in patients with SSNHL as follows: 1) severe complications caused by systemic steroid application (e.g., pheochromocytoma crisis) leading to severe or uncontrollable HT, acute myocardial infarction, pulmonary edema, stroke, organ failure, and even death; 4 2) SSNHL presenting as a local manifestation of an underlying catastrophic illness such as autoimmune disease, antiphospholipid syndrome, cardiovascular disease, leptomeningeal carcinomatosis, or paraneoplastic syndrome;6,7,21–24 and 3) locally aggressive diseases, for example patients with SSNHL dying from large vestibular schwannomas that caused brain herniation and ruptured basilar artery aneurysms.8,20
Our study has several limitations. First, the identification of SSNHL was based on diagnosis codes (maximal coding with five diagnoses, N1 code to N5 code) so may not have been listed as the main diagnosis (N1 code). Second, the study does not provide clinical information of the patients’ direct causes of death and their hospital course. Finally, the study does not specify whether patients had uni- or bilateral SSNHL or disease severity and progression.
Conclusions
Our results reveal the relatively low incidence of inpatient mortality over a 14-year survey period in patients with SSNHL. They indicate that inpatient mortality for patients with SSNHL is likely caused by a severe underlying comorbidity or illness that precipitated SSNHL. We suggest that otolaryngologists should be aware of the potential for such underlying conditions to be causative of SSNHL, as well as the possible mortality associated with these conditions.
Footnotes
Author contributions
Hsin-Chien Chen conceptualized the study, Chao-Yin Kuo drafted the manuscript, and Chih-Hung Wang revised the manuscript for intellectual content. Chi-Hsiang Chung and Wu-Chien Chien analyzed or interpreted the data.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was funded in part by grants received from the Ministry of Science and Technology, Taiwan (MOST 107-2314-B-016-029 and MOST 108-2314-B-016-037 to HC Chen), Tri-Service General Hospital (TSGH-C108-037 and TSGH-D-109053 to H.C. Chen), and National Defense Medical Research grants, Taiwan, ROC (MAB-105-019 and MAB-106-003 to H.C. Chen). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.