
Abstract
Introduction:
Birth defects are a leading cause of neonatal mortality worldwide, particularly in low- and middle-income countries. In Latin America, longitudinal studies on BD prevalence and mortality remain limited.
Objectives:
To describe BD epidemiology in Bogotá and Cali (2002-2019), focusing on prevalence, in-hospital mortality, and associated maternal and neonatal factors.
Methods:
We conducted a retrospective, population-based cohort study using PREVERDEC surveillance data from 558 057 births, following Latin American Collaborative Study of Congenital Malformations (ECLAMC) methodology. BD prevalence was expressed per 10 000 live births, and Cox regression identified mortality risk factors.
Results:
BD prevalence was 126.8 (95% CI: 123.9-129.8) per 10 000 live births, with musculoskeletal anomalies most common. Neonatal mortality was 0.26 per 1000 live births. Mortality risk was higher in preterm infants, those with major BD, and circulatory system defects.
Conclusion:
This study provides updated evidence on BD in Colombia, highlighting risk factors for adverse outcomes.
Introduction
Birth defects (BD) arise from disruptions in morphogenesis, leading to structural abnormalities that can be detected during intrauterine development or at birth. BD are classified into 2 categories: minor BD, which do not require medical intervention, and major BD, which may necessitate intervention due to their potential to impair function or cause death. 1 Approximately 60% of the causes of BD in humans remain unknown. However, around 25% of cases are considered “multifactorial,” involving a complex interaction between genetic predispositions and environmental risk factors, such as maternal exposure to specific substances during pregnancy. Other associated risk factors include advanced maternal and paternal age, parental consanguinity, and higher birth order. 2
The European Platform on Rare Disease Registration (EUROCAT) reported a total prevalence of major BD of 239 per 10 000 births between 2003 and 2007. 3 In Latin America, the Latin American Network for Congenital Malformations (ReLAMC) documented a prevalence of 111 cases per 10 000 live births (LB). 4 In Colombia, the National Institute of Health recorded a prevalence of 146 cases per 10 000 LB in 2021. 5
According to the Global Burden of Disease study (1990-2019), which reports incident cases, the most frequently affected system was the cardiovascular system (39.3%), followed by the musculoskeletal (26.99%) and the digestive system (10%). Notably, congenital heart defects were the leading cause of mortality in this cohort, accounting for 39.49% of all deaths. 6
According to a 2016 World Health Organization (WHO) report, approximately 303 000 neonates worldwide die every year within the first 4 weeks of life due to a BD. A case-control study conducted between 2015 and 2018 on 2199 women in Iran identified several factors associated with mortality from BD. The most relevant factors, in descending order of significance, were cesarean delivery, and maternal age of 35 years or older. Other factors included residence in rural areas, maternal smoking, consanguineous marriage, and birth weight ≤2500 g. 7
Colombia has implemented the National Birth Defects Surveillance System, coordinated by the National Health Institute, as a public health initiative. Its purpose is to standardize the reporting process of BD and improve case detection within healthcare facilities. Furthermore, Colombia has been a regular contributor to the Latin American Collaborative Study of Congenital Malformations (ECLAMC), an endeavor that strives to improve surveillance, education, and research on BD within the region.
Despite these efforts, nationwide studies that conduct longitudinal observation on prevalence and mortality related to BD are nonetheless quite sparse. Most existing reports are limited in geographic or time span. This study seeks to address that gap by analyzing data from a large, multicenter surveillance population over an 18-year period to characterize the burden and mortality-related factors of birth defects.
The study is based upon an epidemiologic paradigm that identifies BD as high contributors to perinatal and infant mortality and is shaped by biological, health care, and societal determinants. The study is further informed by the perspective associated with the life course orientation that highlights the role of prenatal and perinatal exposure in shaping child survival levels. The study is located within the methodological context of the ECLAMC, which defines uniform criteria for surveillance and maximizes comparability across countries.
The goal of this retrospective cohort study was to characterize the epidemiology of BD recorded by the PREVERDEC surveillance system in Bogotá and Cali (2002-2019), with a focus on their prevalence and in-hospital mortality. We also examined key maternal and neonatal factors to identify groups at greatest risk.
Materials and Methods
Study Design
A retrospective, longitudinal, population-based study was conducted following the approach of the ECLAMC. All newborns with BD were systematically evaluated using a standardized manual of procedures, with certified physicians performing physical examinations to document the defects. Additional data on pregnancy and perinatal variables were collected through direct interviews with the mothers. 8 Ethical approval was waived by the local Ethics Committee of our institution, as the study was retrospective and all procedures were part of routine care (approval code: FM-CIE-8324-14).
Data collection was conducted at 56 hospitals in Bogotá and Cali, which together account for approximately 16.1% and 35.9% of all births in those cities, respectively, based on 2017 estimates. 4 The collected data were filtered based on medical criteria and securely stored on servers provided by Pontificia Universidad Javeriana and the Bogotá Secretary of Health.
The cases included in this study were defined as LB or stillbirths weighing more than 500 grams, delivered at hospitals affiliated with the surveillance system between January 2002 and December 2019, and exhibiting a BD. Further classification of cases was conducted using ICD-10 codes according to the affected system: Nervous (Q00-Q07), Eye-Ear-Face-Neck (Q10-Q18), Circulatory (Q20-Q28), Respiratory (Q30-Q34), Cleft Lip and Cleft Palate (Q35-Q37), Digestive (Q38-Q45), Genital (Q50-Q56), Urinary (Q60-Q64), Musculoskeletal (Q65-Q79), and Other BD (Q80-Q89).
From an initial registry of 7857 cases, we excluded those with missing data on key variables (gestational age, birth outcome, or survival status; n = 787, 9.9%). After exclusions, our final cohort comprised 7076 neonates.
Cases were further classified as major or minor BD based on the Centers for Disease Control and Prevention definitions. Minor BD were defined as “structural changes that pose little or no significant health problems and typically have limited social or cosmetic consequences for the affected individual.” 9 In contrast, major BD were defined as “structural changes that have significant medical, surgical, social, or cosmetic consequences for the affected individual, often requiring medical intervention.” 9
Statistical Analysis
The collected data were analyzed using RStudio and R v4.4 for Windows 11. Demographic data were first analyzed according to variable type: continuous variables were summarized using mean and standard deviation, while nominal variables were described using count and percentage of the total. The continuous variables included maternal age, paternal age, gestational age, birth weight, and birth height. The nominal variables included sex at birth (male, female, indeterminate), multiple pregnancy, compliance with prenatal visits, and compliance with obstetric ultrasounds (OUS). Birth weight was classified by gestational age as low, normal, or high, based on the International Fetal and Newborn Growth Consortium for the 21st Century (INTERGROWTH-21st) criteria. 10 Compliance with prenatal visits and obstetric ultrasounds was defined according to WHO guidelines, which recommend 8 prenatal visits and at least 1 ultrasound before 24 weeks of gestation. 11
The prevalence of BD was calculated as cases per 10 000 LB with a 95% confidence intervals using the Poisson distribution. Additionally, prevalence per 10 000 total births was calculated, including stillbirths. The denominator for the prevalence calculation was based on LB, in accordance with the consensus established in previous BD studies. 12 Prevalence rates were determined both annually and by birth defect system groups.
We performed a Poisson regression analysis to investigate the relationship between the total number of cases and the number of births, adjusting for hospital-level differences and the number of hospitals operating each year. Each observation in the dataset corresponded to a specific hospital in a given year, with the dependent variable being the number of cases reported. The independent variables included the year, modeled as a continuous variable to capture temporal trends, and hospital, treated as a categorical variable to account for differences across facilities. This approach acknowledges that hospital-level characteristics (diagnostic capacity, referral patterns, resource availability) may influence observed prevalence rates.
To adjust for differences in hospital sizes, the logarithm of the number of births in each hospital-year was included as an offset in the model. This allowed us to control for varying exposure levels across hospitals. Additionally, we accounted for the changing number of hospitals operating in different years to ensure that variations in the availability of healthcare services did not bias the results.
The stillbirth rate of BD was calculated as the proportion of stillbirths among the total cases, with stillbirths defined as the death of a fetus with a gestational age greater than 28 weeks and a birth weight above 500 g. Neonatal mortality was estimated as the proportion of deaths occurring during the first 28 days of extrauterine life.
A Cox proportional hazards regression analysis was conducted using R v4.4 and RStudio v2024.04.0 to evaluate the impact of various covariates on individual survival among livebirths. The selection of covariates for inclusion in the model was based on a comprehensive review of relevant literature and clinical significance. The multivariate model included the following variables: low birth weight (<2500 g), preterm birth (<37 weeks), male sex at birth, maternal age (<20 years), multiple pregnancy and maternal tobacco use during pregnancy. Circulatory, nervous and respiratory system BD were also included. The analysis incorporated all follow-up data up to the date of hospital discharge or death, whichever occurred first.
The results of the model are presented as hazard ratios (HR) along with their corresponding 95% confidence intervals, reflecting the risk of experiencing the event of interest associated with each covariate. The Kaplan-Meier method was employed to estimate the survival function until hospital discharge based on significant variables identified in the Cox model. This non-parametric technique calculates the probability of a subject surviving beyond a specific time point.
Results
During the study period from January 2002 to December 2019, a total of 7076 cases were identified. Among these, 98.99% (n = 7005) were LB, while 1.01% (n = 71) were stillbirths. Complete demographic data for all identified cases are presented in Table 1. When birth weight was classified according to gestational age, 12.46% of cases had low birth weight, and 7.53% had high birth weight. Prenatal diagnosis was established in 809 cases (11.43%).
Demographic Characteristics of Cases.

Abbreviation: OUS, obstetric ultrasound.
Among a total of 558 057 births, a prevalence rate of 126.80 (95% CI 123.86-129.79) cases per 10 000 births was observed. Furthermore, among 555 729 LB during the study period, the estimated prevalence rate was 126.05 (95% CI 123.12-129.04) cases per 10 000 LB. When calculating the prevalence rate by city, a higher rate was observed in Cali. A total of 82 937 LB and 1379 cases were registered in Cali, resulting in a prevalence rate of 166.27 (95% CI 157.61-175.29) cases per 10 000 LB. In Bogotá, 474 872 LB and 5626 cases were recorded, yielding a prevalence rate of 119 (95% CI 115.91-122.15) cases per 10 000 LB. Notably, cases in Cali were reported only beginning in 2010. The prevalence rate per year and the expected prevalence according to a Poisson regression can be observed in Figure 1.

Observed and expected prevalence rate for birth defects (2002-2029).
When cases were classified as major or minor BD, the prevalence rates observed were 86.23 (95% CI 83.81-88.70) cases per 10 000 births for major BD and 42.04 (95% CI 40.35-43.78) cases per 10 000 births for minor BD.
The most common BD were those affecting the musculoskeletal system and the eyes, ears, face, and neck, while defects of the respiratory system were the least prevalent. The prevalence by system, along with the corresponding prevalence rates for major and minor BD, is presented in Table 2. When examining the prevalence rates by system and year, a positive trend was observed for all systems except for the eyes, ears, face, neck, and nervous system; these findings are illustrated in Figure 2.
Cases and Prevalence Rate by System.

Abbreviation: CI, confidence interval.
Cases per 10 000 live births.

Prevalence rate of birth defect classified by system affected (2002-2019).
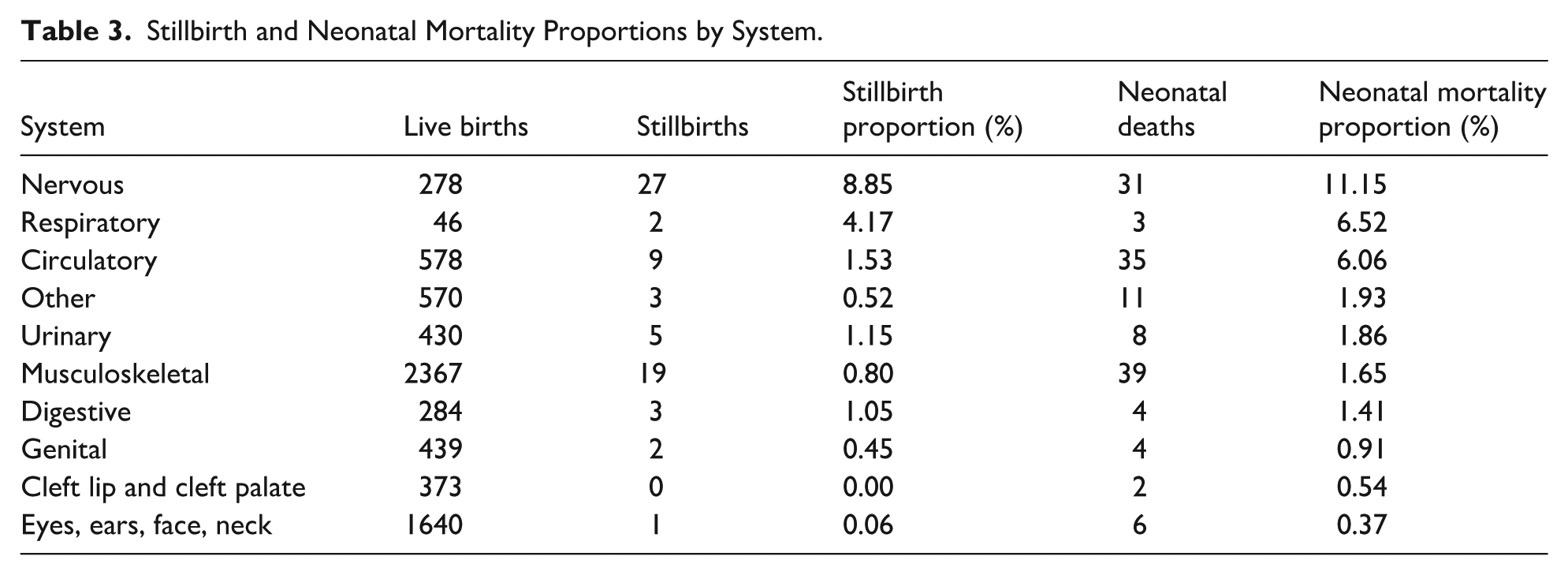
In terms of stillbirth rates, higher rates were observed for BD affecting the nervous and respiratory systems, while lower rates were noted for BD involving the eyes, ears, face, and neck. The 3 deaths reported in the “other” category included 2 cases of acardiocephaly and 1 case of sirenomelia.
A total of 143 intra-hospital neonatal deaths were recorded, resulting in a neonatal mortality rate of 0.26 deaths per 1000 live births. Stillbirth and mortality rates for each system are presented in Table 3. When adjusted using a Cox regression model, 3 variables were found to be associated with an increased risk of mortality: preterm birth, major BD, and circulatory system BD. A complete analysis can be found in Figure 3.
Stillbirth and Neonatal Mortality Proportions by System.

Forest plot of cox proportional hazards model for mortality caused by birth defects.
Kaplan-Meier curves were generated for 3 variables identified as statistically significant in the Cox model: preterm birth, major versus minor BD, and circulatory system BD. These curves are presented in Figure 4.

Kaplan Meier survival curves for patients with birth defects and (A) preterm birth. (B) Major birth defect. (C) Circulatory system birth defects.
Discussion
Multiple studies have documented substantial regional variation in the prevalence of BD. A comprehensive analysis utilizing an age-period-cohort framework examined data from the Global Burden of Disease Study spanning 1990 to 2019. This analysis estimated a global prevalence of 255 cases per 10 000 LB in 2019. Region-specific prevalence rates were also reported, with notable disparities observed across Central Europe, Central Asia, and Andean Latin America, where prevalence rates were 203.3, 350.5, and 162.4 cases per 10 000 LB, respectively. 13
In regional studies, higher prevalence rates have been reported by the EUROCAT, with an incidence of 239 cases per 10 000 LB recorded between 2003 and 2007. 3 However, it remains essential to contextualize these findings with data from low- and middle-income countries (LMICs). Notably, our study identified a higher prevalence compared to recent estimates from Latin American studies; for instance, the ReLAMC reported a prevalence of 111 cases per 10 000 LB. 4
When comparing our findings with previous reports from Colombia, the prevalence rates identified in our study are lower than the 2021 figures reported by the National Institute of Health, which documented 146 cases per 10 000 LB. 5 A separate surveillance study on congenital malformations in Latin America reported a prevalence of 354 cases per 10 000 LB (95% CI: 334-375) in Bogotá and 268 cases per 10 000 LB (95% CI: 252-285) in Cali for the period 2017 to 2019. 4 It is important to note that other studies and registries frequently include cases with multiple BD, potentially increasing prevalence estimates. The observed differences in prevalence between Europe and Latin America may be explained by the more comprehensive surveillance systems for BD in high-income countries.
Furthermore, the study conducted by the ReLAMC analyzed national registries across Latin American countries, revealing that Colombia’s coverage reached only 59.3% of regional registries, compared to an 82.2% coverage rate in other Latin American countries. 4 This disparity highlights significant deficiencies in surveillance and registration systems in Colombia, particularly in rural areas. The underdiagnosis and low registration rates undermine the comprehensiveness and effectiveness of studies and surveillance efforts in the country.
A comparison of BD prevalence rates by system in our study with those reported in other investigations reveals notable differences. Our study demonstrated a higher prevalence of musculoskeletal system BD, followed by anomalies affecting the eyes, ears, face, and neck, and the circulatory system. These findings are consistent with those from a study conducted in Hokkaido, Japan, by Hanaoka et al, where musculoskeletal system BD had the highest prevalence, with 41 cases per 10 000 live births (LB), followed by circulatory system anomalies. 14 In contrast, a study by Shrestha et al (2017-2018) reported a higher prevalence of genitourinary BD, with 16 cases per 10 000 LB, followed by musculoskeletal and cardiovascular system anomalies. 15 Similarly, a cohort study by Chen et al identified cardiovascular system BD as the most prevalent, with 86.08 cases per 10 000 LB, followed by genitourinary and musculoskeletal anomalies. 16 These differences may be due to variations in diagnostic practices and the thoroughness of surveillance systems across different birth cohorts, which could influence the identification and reporting of specific types of birth defects.
Mortality rates associated with BD vary significantly across registries from different countries. In high-income settings, these rates tend to be lower. For example, Sattolo et al reported a BD-associated mortality rate of 1.3 per 1000 LB in Canada. 17 Similarly, Groen et al, utilizing data from the EUROCAT, documented a mortality rate of 1.27 per 1000 LB. 18 In contrast, data from LMICs in Latin America indicate higher rates. Barboza-Argüello and Benavides-Lara, using data from Costa Rica’s National Institute of Statistics and Census, reported a BD-associated mortality rate of 3.19 per 1000 LB. 19 In our study, the mortality rate was considerably lower, at 0.26 per 1000 LB. This difference is possibly influenced by the fact that only in-hospital deaths were recorded.
Our study identified a significantly elevated risk of mortality associated with BD in preterm births (HR: 5.62; 95% CI: 2.76-11.50). This finding aligns with research by Benjamin et al, 20 which found that preterm birth accounted for 51.7% of neonatal mortality in infants with BD. The study also reported an 11.4- to 17.8-fold higher risk of mortality in preterm infants compared to those born at term. Furthermore, in the United States, a 40% increase in BD-associated mortality was observed among preterm infants covered by public insurance compared to those with private insurance. 21 These findings suggest that a comprehensive perinatal approach, including early diagnosis and optimal surveillance for BD, could mitigate mortality related to preterm birth and BD by enabling timely, specialized care.
Among the factors associated with increased mortality in our study, the presence of major BD was a significant determinant. This association was first described by Druschel et al in New York, where infants with major BD were 6.3 times more likely to die compared to those with minor BD. 22 Furthermore, an association with low birth weight (LBW) and very low birth weight (VLBW) has also been described. In a German cohort, infants with VLBW and major BD had an infant mortality rate of 28.5%, compared to 11.5% in those with VLBW and minor BD. 23
Previous studies have confirmed the association between circulatory system defects and neonatal mortality. A birth cohort study from Quebec, Canada (2006-2020), found that cardiovascular malformations were linked to increased mortality before 14 years of age, with HR of 8.36 in males and 9.18 in females. Notably, critical congenital heart defects (CHDs) had nearly 5 times the HR compared to non-critical CHD. 17 Similarly, a study conducted in Costa Rica reported significantly higher mortality rates among infants with CHD compared to those with other BD. 19
The findings of this study have many programmatic and policy-level implications. First, the development and expansion of prenatal screening and diagnostic programs can facilitate the early detection of BD and streamline referral networks for specialist medical care. Second, expanding the coverage of BD surveillance systems would provide more comprehensive evidence vital for the planning and evaluation of preventive interventions. Third, the expansion of access to timely surgical and medical services among neonates is vital in reducing mortality levels related to these conditions. Additionally, the strengthening of maternal health programs (in relation to the management of chronic and pregnancy-related disorders) is important in reducing the prevalence of BD.
One of the major limitations of this study was the lack of data on the specific causes of death. Previous studies have indicated that BD are rarely the direct cause of mortality. 17 Additionally, the limited surveillance period restricted the ability to estimate long-term survival into childhood. As with systems reliant on human data entry, a margin of error in case registration was observed, affecting the analysis of certain variables. Furthermore, because our analysis draws exclusively on data from urban hospitals in Bogotá and Cali, it may not be generalizable to rural areas or other regions of Colombia, where surveillance coverage and healthcare access differ. Future studies that incorporate rural and peripheral facilities will be needed to fully capture the national burden of birth defects.
The primary strength of this study lies in its focus on isolated cases, enabling a more precise characterization of this specific patient subgroup, without the confounding influence of complex cases involving multiple BD. Additionally, the inclusion of data from 2 major cities in Colombia, encompassing 56 hospitals, provides broad coverage of LB, enhancing the reliability of the observed prevalence rates. The neonatal mortality analysis offers valuable insights into factors associated with early death in LMICs. Furthermore, the extensive range of variables collected according to the ECLAMC methodology allows for a comprehensive assessment of prenatal and postnatal factors potentially linked to BD.
Conclusion
This study presents a cohort of BD cases in Bogotá and Cali, Colombia, providing a comprehensive analysis of their epidemiological patterns, demographic characteristics, and factors associated with mortality. A higher prevalence compared to previous Latin American studies was observed, highlighting improvements in national screening programs, improvements in health education for the general population, healthcare coverage, access and utilization. The mortality analysis identified significant associations with nonmodifiable factors, such as preterm birth, circulatory system defects, and major BD. Establishing accurate prevalence and mortality rates is crucial for guiding healthcare and government initiatives to improve outcomes for patients with BD in LMICS and underserved communities.
Footnotes
Acknowledgements
To the Program for the Prevention and Surveillance of Birth Defects and Rare Diseases and the Health Secretary of Bogotá.
ORCID iDs
Ethical Considerations
Ethical approval was waived by the local Ethics Committee of Pontificia Universidad Javeriana, as the study was retrospective and all procedures were part of routine care (approval code: FM-CIE-8324-14).
Author Contributions
Pablo Pineda-Sanabria: Study design—literature review—material preparation—data analysis—writing and editing manuscript. Esteban Portilla-Rojas: Study design—literature review—material preparation—data analysis—writing and editing manuscript. Catalina Arbelaez-Hoyos: Study design—literature review—writing manuscript. Valentina Baquero-Castro: Study design—literature review—writing manuscript. Juliana Lores: Editing manuscript—final manuscript approval. Karen Sarmiento: Editing manuscript—final manuscript approval. Ignacio Zarante: Editing manuscript—final manuscript approval.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Due to confidentiality of patient records, data analyzed are not publicly available.