
Abstract
Objective
Over 8 million newborns worldwide have congenital anomalies; 3.2 million have resultant disabilities. Ethiopia has a high burden of neonatal congenital anomalies, but research on predictors is limited. This study investigated predictors of neonatal congenital anomalies in eastern Ethiopia.
Methods
A facility-based unmatched case–control study on 387 mother–infant pairs (129 cases, 258 controls) in public hospitals was conducted. Data were obtained using an interviewer-administered structured questionnaire and a medical record review. Binary logistic regression with adjusted odds ratios (AOR) and 95% confidence intervals (CI) was used to identify predictors of congenital anomaly.
Results
Nervous system anomalies were most common 84 (65.1%), followed by gastrointestinal system anomalies 20 (15.5%). Maternal anemia (AOR: 4.37, 95% CI: 2.48–7.69), alcohol consumption during index pregnancy (AOR: 4.01, 95% CI: 1.88–8.54), khat chewing (AOR: 1.73; 95% CI: 1.04–2.85), rural residence (AOR: 1.73, 95% CI: 1.04–2.85) and antenatal care attendance (AOR: 0.43, 95% CI: 0.22–0.84) were significant predictors of congenital anomaly.
Conclusion
Several risk factors for congenital anomalies were identified. To reduce risk, antenatal care services should be improved and mothers encouraged to avoid harmful substances during pregnancy and maintain a healthy lifestyle. Intervention strategies are needed to target these risk factors.
Keywords
Introduction
Congenital anomalies are structural or functional defects that occur during pregnancy. 1 Such anomalies are the fifth leading cause of morbidity and mortality in children worldwide.2–5 They affect 8.1 million newborns worldwide, and more than 3.3 million babies die annually from these problems. In addition, over 3.2 million children have disabilities owing to congenital anomalies.6–8 Of every 10 children born with serious congenital anomalies, 9 are born in low- or middle-income countries (LMICs).8,9 Congenital abnormalities occur at a rate of 4.54 per 1000 live births in sub-Saharan Africa.10,11 According to recent evidence, the prevalence of birth defects is 1.9%, and such problems cause approximately 4% of neonatal deaths in Ethiopia.7,12
Congenital anomalies can cause long-term illness and disabilities, and can be fatal.1,13 They also place stress on mothers and society in general, causing problems for individuals, families, healthcare systems and societies.14,15 Congenital anomalies are caused by a combination of factors, including genetics, environment, maternal factors such as advanced maternal age, maternal illnesses such as diabetes mellitus, infection, maternal nutritional deficiencies such as iodine and folic acid, and exposure to medicinal and recreational drugs such as alcohol and tobacco.1,16,17
Maternal infections such as syphilis and rubella are the main causes of congenital anomalies in LMICs. 18 Furthermore, various studies in LMICs, including Ethiopia, have shown that risk factors such as urban residency, 19 insufficient antenatal care (ANC),20,21 alcohol consumption,7,22,23 and chewing khat leaves during pregnancy are associated with congenital anomalies.22,23 In addition, a study conducted in Nigeria and Ethiopia found that low birth weight 24 and preterm birth were linked to congenital anomalies.13,25,26
A new approach is needed to reduce congenital anomalies. It is essential to identify contextual factors to help prevent neonatal deaths and disabilities caused by congenital anomalies.2–5 Few studies have been conducted on predictors of congenital anomalies in Ethiopia.7,8,27 Therefore, the aim of the current study was to identify the predictors of congenital anomalies in the Harari region and the Dire Dawa administration in eastern Ethiopia.
Method and materials
Study setting and design
A multicenter unmatched case–control study was conducted from 1 May 2022 to 1 July 2022 at four neonatal intensive care units in public hospitals in the Harari region and the Dire Dawa administration in eastern Ethiopia. The study was conducted in Dilchora Referral Hospital and Sabian General Hospital in the Dire Dawa administration, and in Hiwot Fana Specialized University Hospital and Jugal General Hospital in the Harar region. These facilities provide care to more than 3 million people in the catchment areas, which include urban and rural residents of Harar and Dire Dawa, as well as people in the eastern Hararghe zone of Ethiopia’s Oromia region.
Population and eligibility criteria
All neonates (mother–infant pairs) diagnosed with congenital anomalies and admitted to hospitals were included in the study as cases. Neonates without congenital anomalies admitted to the hospitals during the study period were included as controls. Neonates born to mothers with severe mental illness, neonates born before 28 weeks of pregnancy and neonates admitted without biological mothers were excluded.
Sample size determination and sampling procedure
Using Epi Info Version 7.2.1 (Centers for Disease Control and Prevention, Atlanta, Georgia, USA), the required sample size was calculated according to the following assumptions: 95% confidence interval (CI), 80% power and 1:2 ratio of cases to controls. The proportion of exposure to pesticides was 4.03% for the controls and 13.23% for the cases,23,25 with a 10% nonresponse rate. Thus, the required sample size was 387 (129 cases and 258 controls).
The hospitals included in the study were chosen because they receive more than 90% of the neonatal admissions in eastern Ethiopia. The sample size was calculated using a probability proportional to size method based on the proportion of the average monthly client flow as determined from hospital registration records. According to the average 2-month hospital management information system report records, the total number of neonatal intensive care unit admissions for the four hospitals was 792, of which 656 neonates did not have congenital anomalies and 136 had congenital anomalies. Of these, 129 cases and 258 controls were included in the study.
Data collection method
Four midwives with BSc degrees collected data using a pretested, structured interviewer-administered questionnaire adapted from previous studies.26–28 The questionnaire was divided into five sections that measured sociodemographic, obstetric, maternal, lifestyle and neonatal factors. Following the maternal interview, the medical records were reviewed for fetal factors. This study included neonates with at least one overt birth defect. The outcome variable was assessed using data from medical records of neonates diagnosed with congenital anomalies by a pediatrician at admission.
Measurements
A
Data quality control
Before data collection, all data collectors and supervisors received 2 days of training. Before data collection, a pretest was conducted at a different hospital (Haramaya Hospital) on a sample that was 5% of the size of the study sample. Some changes were made to the data collection method based on the results of the pretest. The data collection procedure was closely monitored, and the completion of each questionnaire was checked daily. A logical checking technique was used to identify errors during the data cleaning process. Finally, double data entry was performed to ensure consistency. Data were kept in a file placed in a secure location accessed only by the principal investigator, and data confidentiality was ensured by not recording any names or personal identifying details.
Data processing and analysis
The data were entered into EpiData, Version 3.1 (EpiData Association, Odense, Denmark), and analyzed using IBM SPSS Statistics for Windows, Version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistical variables were examined using cross-tabulation. Frequency distributions and summary statistics were calculated for both groups. The association between covariates and outcome variables was assessed using multivariable logistic regression analysis. The variance inflation factor (>10) and standard error (>2) were used to assess multicollinearity, and the Hosmer–Lemeshow test (>0.05) was used to assess goodness of fit. The adjusted odds ratio (AOR) with 95% CI were used to test associations with the outcome variable; a p-value of <0.05 was considered statistically significant.
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee of the College of Health and Medical Sciences, Haramaya University (Ref No. IHRERC/078/2022). Following approval, an official written letter of cooperation was given to the administrative health bureau and the facilities. Written informed consent was obtained from all participants. Confidentiality was ensured throughout the study process.
Results
Sociodemographic characteristics
This study included 387 mother–infant pairs, and the response rate was 100%. The mean (standard deviation) age of the mothers in the case and control groups was 27.82 (6.15) years and 25.83 (5.62) years, respectively. The age of the women ranged from 16 to 35 years. Sixty-four (49.6%) cases and 82 (31.8%) controls resided in rural areas. In terms of maternal education, 56 (43.4%) cases and 87 (33.7%) controls received primary education, respectively (Table 1).
Sociodemographic characteristics of mothers of neonates admitted to public hospitals in eastern Ethiopia, 2022 (n = 387).

*Others (Single, widowed, separated).
Types of overt congenital anomalies
In the 129 cases, the most common types of congenital anomalies were nervous system anomalies 84 (65.1%), such as meningoencephalocele (n = 27), hydrocephalus (n = 24), spinal bifida (n = 23), anencephaly (n = 6) and encephalocele (n = 4). The next most common type was gastrointestinal system anomalies (20, 15.5%), such as omphalocele (n = 9), gastroschisis (n = 5) and imperforate anus (n = 6); followed by musculoskeletal system anomalies (16, 12.4%), such as cleft lip and/or palate (n = 8) and club foot (n = 8); and genitourinary system anomalies (9, 7%), such as hypospadias (n = 5) and ambiguous genitalia (n = 4) (Figure. 1).

Types of overt congenital anomalies among neonates admitted to public hospitals in eastern Ethiopia, 2022 (n = 129).
Maternal illness and obstetrical characteristics
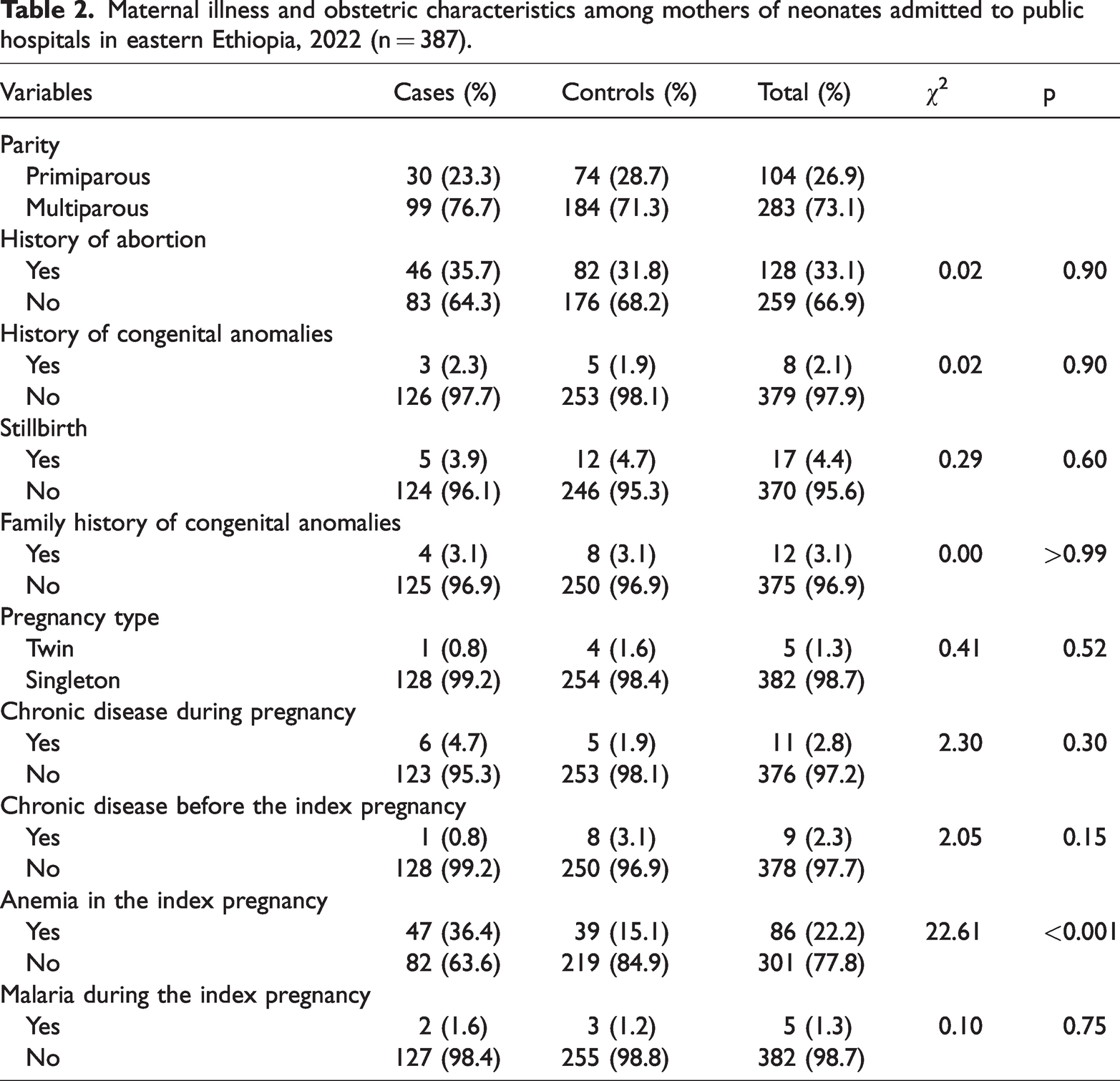
The results showed that 99 (76.7%) cases and 184 (71.3%) controls were multiparous. Forty-seven (36.43%) cases and 39 (15.1%) controls had anemia. Regarding maternal chronic diseases, 6 (4.70%) cases and 5 (1.94%) controls had chronic diseases during pregnancy. A history of abortion was found in 46 (35.7%) cases and 82 (31.8%) controls (Table 2).
Maternal illness and obstetric characteristics among mothers of neonates admitted to public hospitals in eastern Ethiopia, 2022 (n = 387).
Antenatal care and lifestyle characteristics
In this study, 94 (72.9%) cases and 226 (87.6%) controls received ANC. During this pregnancy, 81 (62.8%) cases and 115 (44.6%) controls chewed khat. Regarding alcohol consumption, 24 (18.6%) cases and 16 (6.2%) controls had a history of alcohol consumption during pregnancy. Folic acid was used in 85 (65.9%) cases and 213 (82.6%) controls (Table 3).
Antenatal care and lifestyle characteristics of mothers of neonates admitted to public hospitals in eastern Ethiopia, 2022 (n = 387).

Neonatal-related characteristics
The number of male neonates was 62 (48.1) in the case group and 145 (55.8) in the control group. The birth weight of 43 (33.3%) cases and 66 (25.6%) controls were less than 2500 g. Furthermore, 65 (50.4%) cases and 42 (16.3%) controls were preterm (Table 4).
Neonatal-related characteristics of neonates admitted to public hospitals in eastern Ethiopia, 2022 (n = 387).

Predictors of congenital anomalies
A history of maternal anemia during the index pregnancy, maternal alcohol consumption during the index pregnancy, ANC attendance, maternal khat chewing during the index pregnancy, and residence were all independently associated with congenital anomalies in the multivariable logistic regression analysis. The odds of having an infant with congenital anomalies were four times higher (AOR: 4.37, 95% CI: 2.48–7.69; p < 0.001) in mothers with anemia during the index pregnancy compared with those with no anemia. Compared with their counterparts, neonates from women with a history of alcohol consumption during the index pregnancy were four times more likely (AOR: 4.01; 95% CI: 1.88–8.54; p < 0.001) to develop congenital anomalies. The odds of congenital anomalies in neonates born to women who received ANC were reduced by 57% (AOR: 0.43, 95% CI: 0.22–0.84; p = 0.014) compared with those who did not receive ANC during the index pregnancy. Furthermore, neonates from women who chewed khat during the index pregnancy had a 1.73-fold (AOR: 1.73; 95% CI: 1.04–2.85; p < 0.032) higher risk of congenital anomalies than their counterparts. Furthermore, the odds of congenital anomalies in neonates born to rural women were 1.73 times higher (AOR: 1.73; 95% CI: 1.04–2.97; p < 0.036) than in their urban counterparts (Table 5).
Bivariable and multivariable logistic regression analysis of determinants of congenital anomalies among neonates admitted to public hospitals in eastern Ethiopia (n = 387)

**Significant at p < 0.05. COR, crude odds ratio; AOR, adjusted odds ratio; ANC, antenatal care attendance; CI, confidence interval.
Discussion
Globally, congenital anomalies result in a larger proportion of neonatal deaths, and have substantial socioeconomic effects on individuals, families, society and healthcare systems. 8 Identifying the predictors of congenital anomalies is important to reduce neonatal and child mortality. This study aimed to determine the predictors of congenital anomalies in public hospitals in eastern Ethiopia. The risk of congenital anomalies was higher among mothers with a history of anemia during the index pregnancy, a history of alcohol consumption during the index pregnancy, khat chewing during the index pregnancy, and those who resided in rural areas. However, attending ANC sessions was a protective factor against the development of congenital anomalies.
This study showed that neonates born to anemic mothers during the index pregnancy had a four-fold higher risk of developing congenital anomalies than those born to mothers who were not anemic during the index pregnancy. This finding is consistent with the findings of previous studies conducted in Ethiopia and Saudi Arabia.33–35 It is possible that anemic pregnant women are more likely to also have folic acid deficiencies; insufficient consumption of folic acid and multivitamins may result in the birth of babies with neural tube defects. 36
In this study, maternal alcohol consumption during early pregnancy was associated with a four-fold increased risk of congenital anomalies. This supports findings from studies conducted in California, 37 China38–40 and Ethiopia.8,22 This likely reflects that fact that alcohol has complex effects on developmental processes; alcohol may disrupt fetal development by altering stem cell genomes via acetaldehyde, an endogenous and alcohol-derived source of DNA damage, which promotes cell degeneration. 41
The current findings showed that mothers who chewed khat were twice as likely to have neonates with congenital anomalies than those who did not chew khat. This finding is in line with that of a study conducted in southeast Ethiopia.22,23 In our study setting, khat chewing is a common and popular social practice engaged in by many people, including pregnant women. Khat may affect intrauterine fetal growth by altering the chemical composition of fetal organs and reducing overall fetal weight and fat. These effects may result in depletion of carbohydrate provision to embryonic organs and suppression of DNA and proteins. 42 Khat consumption reduces maternal appetite, resulting in lower food consumption. Furthermore, many women consume large amounts of tea and coffee while chewing khat, which reduces iron absorption. 43
Furthermore, the current study showed that neonates of women who attended at least one ANC session during their index pregnancy were less likely to have congenital anomalies than those of women who had not attended at least one ANC session. This is consistent with previous studies conducted in Iraq 20 and Ethiopia. 30 A possible explanation is that women who do not attend ANC during index pregnancy do not receive iron and folic acid supplements, which has a major effect on neonatal health. 44 However, this assumption is not supported by a study conducted in Bahir Dar, Ethiopia. 19 However, this previous study extracted data from neonatal medical records and so may have not recorded all ANC attendances.
In the current study, neonates born in rural areas had a higher risk of congenital anomalies than those born in urban areas. This finding is comparable to the findings of a study conducted in Bishoftu General Hospital, Oromia, Ethiopia, 26 but inconsistent with findings from the study conducted in Bahir Dar, Ethiopia. 19 This difference between urban and rural neonates may be because mothers in rural areas lack access to a range of media information sources and expert personnel and so are not well-informed about preventable risk factors for congenital anomalies. 45 Poor dietary diversity, particularly a lack of iron-rich foods, has previously been linked to birth defects in rural areas. 46
Limitations
It was not possible in this study to confirm definitive cause-and-effect relationships among the variables. In addition, the data were drawn from interviews and medical record reviews; therefore, recall bias may have occurred. This was an institutional study focusing on newborns admitted to neonatal intensive care units, so may not be generalizable to other populations.
Conclusion
The most common type of congenital anomaly found in this study was nervous system anomalies (65.1%), followed by gastrointestinal system anomalies (15.5%). A history of maternal anemia during the index pregnancy, alcohol consumption during the index pregnancy, ANC attendance, chewing khat during the index pregnancy and living in a rural area were significant predictors of congenital anomalies. To reduce the burden of congenital anomalies, modifiable risk factors such as maternal anemia, alcohol consumption and khat chewing should be targeted, and the use of ANC follow-ups should be encouraged.
Footnotes
Acknowledgements
We would like to thank Haramaya University and Dire Dawa University for their unreserved technical support. We would also like to extend our gratitude to the hospital heads, the study participants, the data collectors, and the supervisor for their support.
Author contributions
NB, AD and KTR made a substantial contribution to the conception, study design, execution, acquisition of data, analysis and interpretation. MK and ML contributed to critically revising the paper, the revision of the data analysis and the editing of the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.