
Abstract
Objectives:
Coronary artery anomalies are uncommon, but important cardiac malformations, representing the second commonest cause of death in young athletes.
Methods:
We utilized computerized tomographic angiography to screen and precisely delineate coronary artery anomalies in patients with minimal cardiac symptoms.
Results:
During 3.5-year period, we performed 2888 computerized tomographic angiographies. A total of 33 (1.1%; 95% confidence interval = 0.7–1.5) cases of coronary artery anomalies were identified (mean age = 44 ± 13.5 (15–70) years). In total, 23 patients (mean age = 43 years) had malignant coronary artery anomalies with an inter-arterial course of the aberrant vessel: of which 3 had left main coronary artery arising from right coronary sinus and 20 right coronary artery from left sinus; 19 patients were of Asian and 14 were of Arab origins. Of interest, 21 out of 33 patients had chest pain, 5 had palpitations, and 2 had breathlessness. There were no examples of sudden cardiac death. All patients received appropriate advice regarding physical exertion and medical management, and remained well for 2–5 years of follow-up. Of 33 patients, 4 had significant symptomatic coronary artery disease requiring intervention: 1 percutaneous coronary intervention and 3 coronary artery bypass graft surgery.
Conclusion:
There is a relatively high incidence of coronary artery anomalies with malignant course in Asians. The vast majority were managed conservatively.
Keywords
Introduction
Coronary artery anomalies (CAA) are relatively uncommon, but important cardiac malformations, representing the second commonest cause of sudden cardiac death in young athletes.1–4 In individuals above the age of 35 years, the prevalence of coronary artery disease increases and becomes an important predisposing factor to sudden cardiac death. 4 Despite the fact that the vast majority of CAA are benign and are of academic interest only in the adult population, certain anatomical variants have been linked to sudden cardiac death associated with exercise.5,6 Such anatomical variants include a major coronary trunk that arises from the opposite sinus of Valsalva and passes in-between the two major arterial trunks (aorta and pulmonary artery) where there is potential for significant compression during strenuous exercise. The significance of this anatomical variant of CAA with the malignant course has been evaluated in an inconsistent manner in the adult population mainly due to lack of studies with large-enough groups of patients.
We report a relatively high incidence of CAA with the so-called malignant course that has been identified using computerized tomographic angiography (CTA) in an Asian population. We discuss the clinical relevance of these lesions in the adult population, with recommendations for management.
Materials and methods
A retrospective analysis of all dual-source CTA studies completed in a tertiary-care cardiac centre between September 2011 and November 2014 was performed. Clinical presentation, electrocardiogram (ECG) at the time of presentation, echocardiographic studies when relevant, data of conventional coronary angiography when applicable, medical or surgical treatment, and subsequent follow-up were examined and evaluated for all patients who had CAA on CTA. The CTA of those patients with CAA were re-examined for this analysis by a radiologist experienced in the field. All cases of normal coronary anatomy were excluded from this study. This study received an automatic exemption from the Ethics Committee as it only involved the review of previously captured images and already existing electronic patient records.
Technique of CTA
All the studies were performed on a newly installed CT machine at the cardiac centre using the same protocol in all patients. We utilized a 128-slice, dual-source scanner (Somatom Definition Flash, Syngo CT 2011 A, Erlangen, Germany). Patients were positioned appropriately in a supine position, ECG leads were attached, and large intravenous access (18 gauge) was established for the injection of the contrast agent at a rate of 6 mL/s. All patients were pre-medicated with a short-acting nitroglycerin sublingual spray and intravenous β-blockade (5–20 mg of intravenous metoprolol) given only for the patient with heart rate higher than 70 beats per minute (bpm). The target heart rate was below 70 bpm.
Data acquisition and three-dimensional (3D) reconstruction enabled us to precisely define the origin of the main coronary arteries, or one of its main branches, the course taken to reach the final destination, and its relationship to important structures within the heart, as well as the presence of stenotic coronary artery disease.
Definition of CAA
For the purpose of this study, we defined CAA as a congenital anomaly of the main coronary artery or one of its major branches that may involve abnormal origin, course, or displacement of the coronary ostium outside of its original sinus of Valsalva. Furthermore, we used the terms malignant and non-malignant CAA, with malignant referring to an anomaly that involves an abnormal origin of a major coronary trunk such as the right coronary artery (RCA) or the left main coronary artery (LCA) with the main trunk taking a course between the pulmonary artery/right ventricular infundibulum and the ascending aorta (inter-arterial course).1–3,7 Therefore, the term malignant or non-malignant refers to the relationship between anomalous major trunk to the major arteries, the aorta, and the pulmonary artery. The relationship between the anomalous right or left main trunk to the major arteries is shown in Figure 1. In this study, it was not possible to define the presence or the nature of an intra-arterial wall course of a major trunk or a structural abnormality of the coronary ostium.

This is a schematic representation of CTA images of normal and malignant RCA and LCA anomalies.
Statistical analysis
Prevalence of coronary anomalies was defined in terms of proportion with 95% confidence interval (CI). Age as a variable was defined in terms of mean and standard deviation (SD) with its range. Variables such as ethnicity and gender are shown in frequency and percentages. SPSS 22.0 statistical package was used to calculate the descriptive statistics.
Results
There were 2888 CTA studies performed between September 2011 and November 2014. We identified 33 patients (1.1% of 2888; 95% CI = 0.7–1.5) with at least one type of coronary artery anomaly. The age range was 15–70 years, with a mean age of 44 ± 13.5 years. There were two 15-year-old patients. The racial breakdown of these patients is as follows: 17 (51.6%) patients were of Asian origin and 14 (42.4%) were of Middle Eastern origin (Table 1). Also, of 33 patients, the incidence of CAA in males was 28 (85%) and in females 5 (15%).
Profile of patients with CAA.
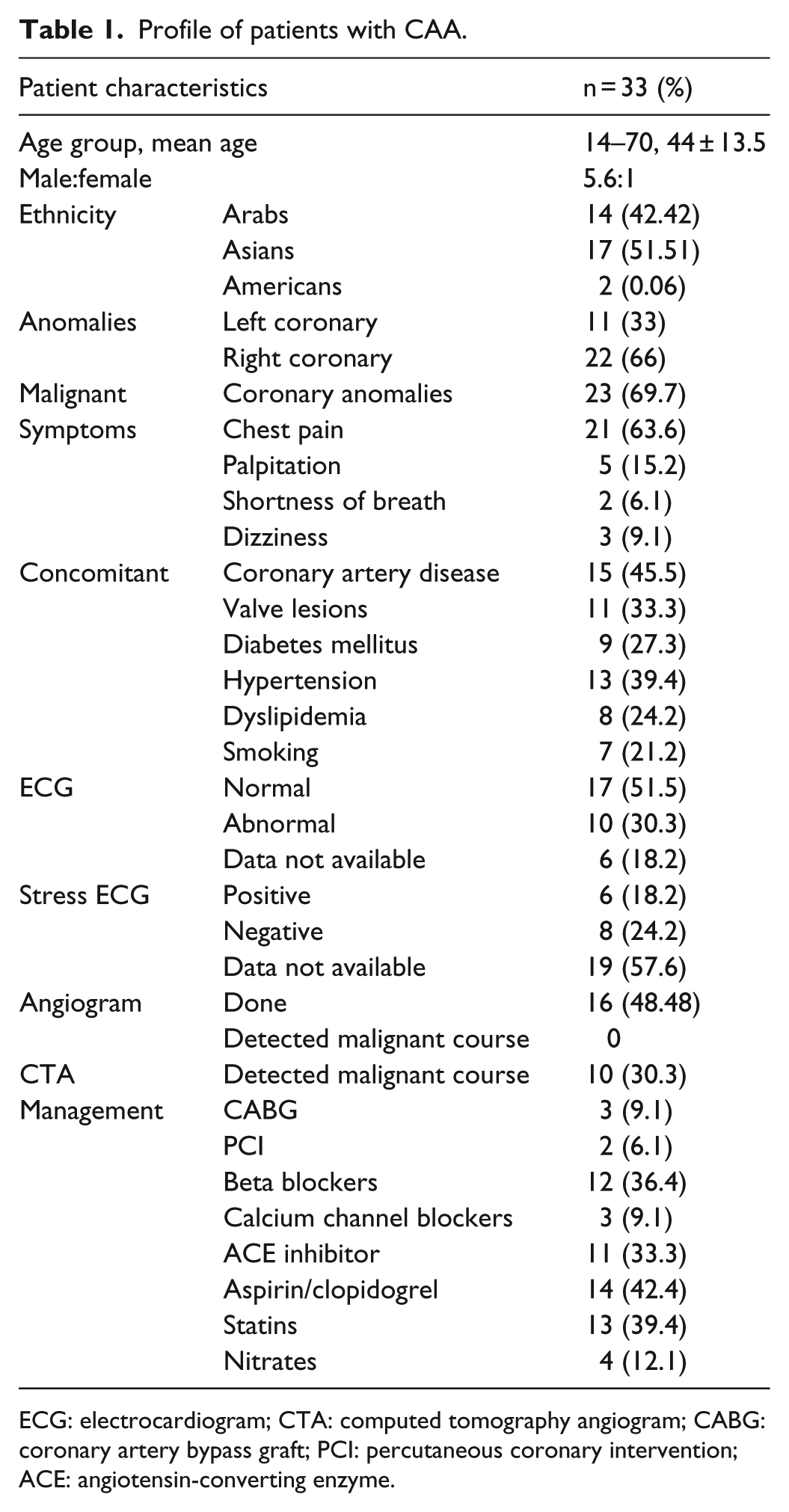
ECG: electrocardiogram; CTA: computed tomography angiogram; CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention; ACE: angiotensin-converting enzyme.
Malignant CAA
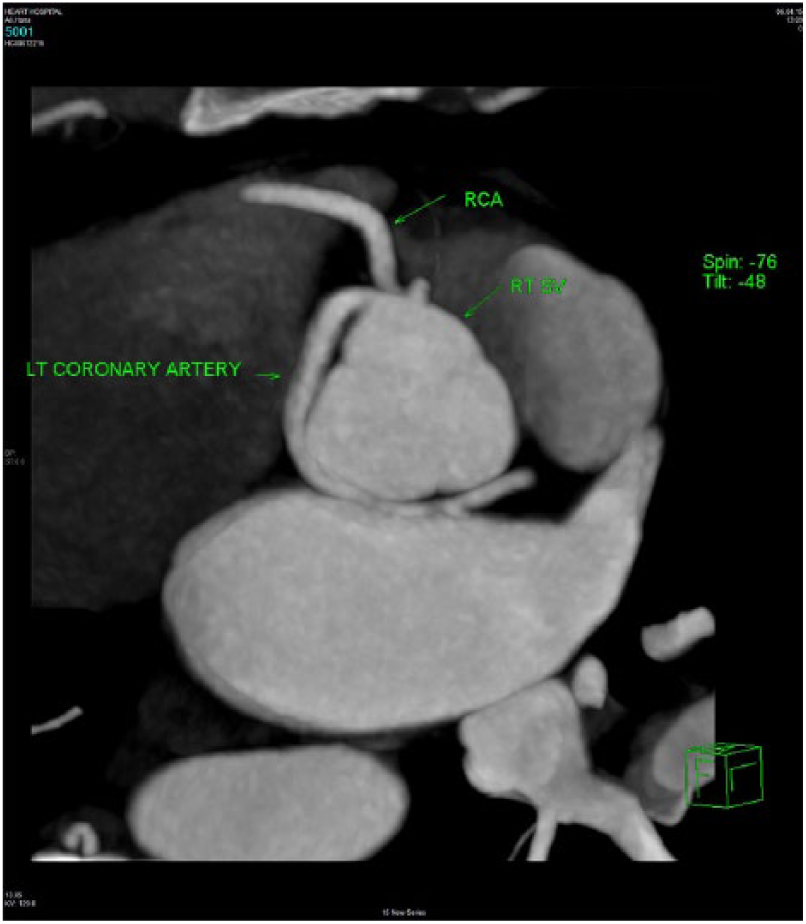
A total of 23 patients (out of 33, 69%) had CAA with a malignant course (Table 2). Of which 3 patients had a left coronary artery arising from the right sinus of Valsalva with an inter-arterial course (Figure 2) and 20 had right coronary arteries arising from the left sinus of Valsalva with an inter-arterial course (Figure 3). Out of the 23 patients with a major trunk passing between the two great vessels, only 1 patient showed narrowing of the trapped segment of coronary artery. This narrowing was not significant and did not require intervention.
All malignant anomalies.
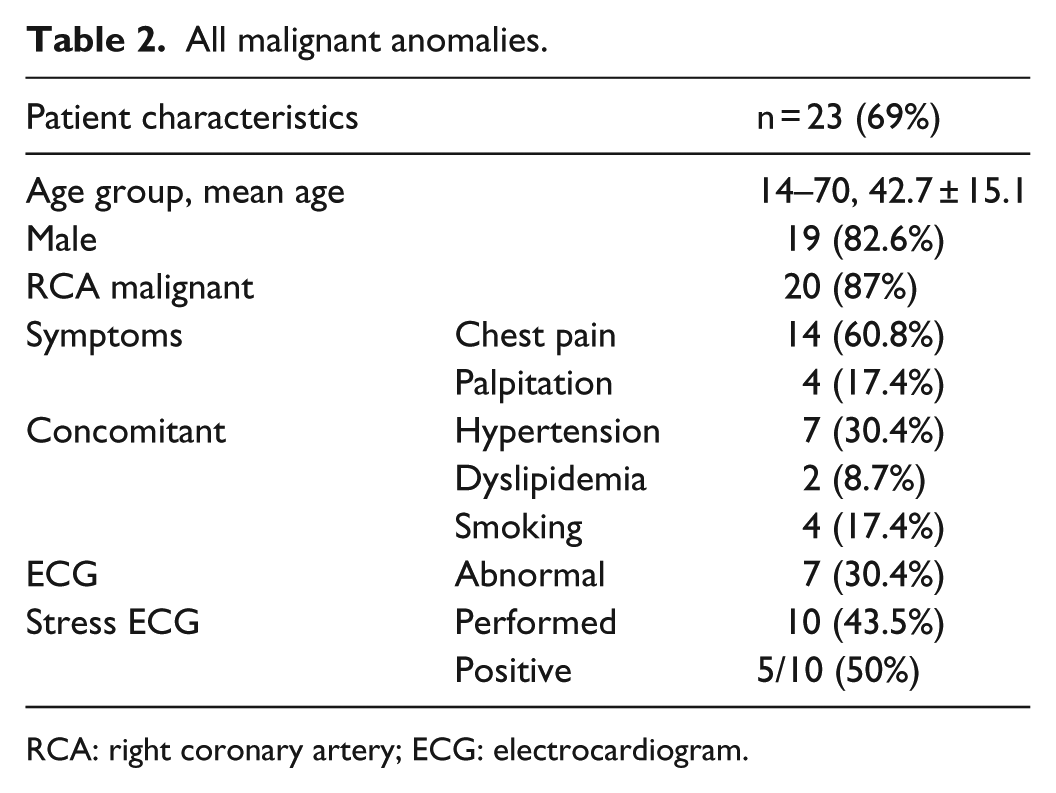
RCA: right coronary artery; ECG: electrocardiogram.
CTA image of a patient with a malignant LCA showing a tortuous course of LCA between the two great vessels.

CTA image of a patient with a malignant RCA anomaly showing the abnormal course of the RCA.
Other CAA
Of the remaining 10 patients (out of 33, 30%), 4 had the circumflex artery (CX) arising from the right coronary sinus and coursing behind the aorta and pulmonary artery to reach its final destination; in one of the patients, the abnormal artery had a common ostium with the RCA, but in the other 3, there were separate ostia. One patient had a normal origin and course of both main coronary trunks, but the left main trunk was exceptionally long with the left anterior descending artery (LAD) branching from a point low down in the interventricular groove. One patient had both coronary artery trunks arising from their normal respective sinuses and followed their normal course; however, an accessory LAD was seen arising from the RCA, passing in front of the pulmonary trunk to reach the LAD territory parallel to the original LAD resulting in two LADs running side by side in the front of the heart. Two patients had the RCA arising from the LAD, with both coursing in front of the heart and pulmonary infundibulum to reach the normal territory of distribution. One patient had the ostium of the RCA displaced into the aortic wall outside and above the boundaries of the right sinus of Valsalva. One patient had the LCA arising from the right coronary sinus but coursed in front of the pulmonary artery and right ventricle infundibulum to reach the front of the heart to divide into LAD and CX arteries. There were no cases of aberrant coronary artery arising from the pulmonary artery in this series.
Clinical presentation
In our institution, CTA is not the first-choice diagnostic modality for the investigation of cardiac symptoms. All the patients in this study were referred for CTA to investigate what could only be described as non-specific symptoms. In all, 21 patients presented with chest pain as the predominant symptom, 5 patients with palpitation, and 3 patients had syncope. One of the patients with LCA arising from the right sinus of Valsalva and inter-arterial course had ST segment depression in leads II, III, and aVF on routine ECG, but a negative exercise ECG on dynamic testing. The patient subsequently underwent conventional angiography which showed mild coronary artery disease. A total of 14 patients underwent stress ECG, of which 6 of them were positive for inducible ischaemic changes. Of those 6 patients, 5 had an RCA arising from the left sinus with an inter-arterial course, and 2 of them underwent coronary artery bypass grafting for demonstrable coronary artery disease following conventional angiography. It is important to note that the coronary artery disease did not involve the segment of the artery passing between the two great vessels (aorta and pulmonary artery).
CAA in athletes
There were two young athletes among this group. One patient was a 15-year-old female track-and-field athlete who complained of shortness of breath, palpitations, and chest discomfort while training. She had been involved in track-and-field training for a number of years before the development of her symptoms which, we believe, were due to RCA arising from the left sinus of Valsalva and passing between the great vessels. She demonstrated a positive-stress ECG for ischaemia. There was no luminal stenosis involving the segment of coronary artery between the two great vessels or elsewhere. The second patient was a 30-year-old footballer who developed chest tightness and breathlessness during competitive matches few months prior to presentation, despite the fact that he was playing consistently for many years with no symptoms. Also, he demonstrated ST segment depression and widened QRS complex on ECG without stress. His CTA showed an LCA arising from the right sinus of Valsalva and passing between the two great arteries. Both of these athletes had to discontinue their respective sporting activity. The young female athlete requested bypass surgery in order to allow her to continue her career in athleticism, but we felt that that would not be justifiable due to her young age.
CAA with significant coronary artery disease
Four patients were diagnosed with significant coronary artery disease. Three patients underwent successful coronary artery bypass grafting for multi-vessel coronary artery disease. One patient had LAD disease for which he underwent percutaneous coronary intervention and stent placement.
Management and follow-up
Medical management consisted of specific advice relating to avoidance of extreme exertion and physical activities, a combination of beta-blockers or calcium antagonists when appropriate, and risk factor therapy and prevention. Sixteen patients underwent conventional angiography to further investigate their symptoms. Ten patients had a diagnosis of malignant CAA; even though conventional angiography demonstrated the abnormal origin, they failed to identify the precise course of the anomalous artery. Thirty one patients were followed up for 2–5 years, while two patients were lost to follow-up, with none suffering sudden cardiac death or angina. Despite the high incidence of malignant anomalies, none of our patients underwent bypass surgery for the specific purpose of addressing the presence of the CAA.
Discussion
This study demonstrates two important findings in this group of patients with congenital CAA. We have identified, in this predominant Asian and Middle Eastern population, a relatively high incidence of the so-called malignant CAA. Of all CAA, 23 were of this malignant type with a high incidence of abnormal RCA origin from the sinus of Valsalva. Eckart et al. 5 reported on the possibility of a malignant RCA anomaly causing sudden cardiac death in military recruits. Similarly, high incidence of malignant RCA anomalies has been identified in a Chinese population by Zhang et al., 8 using dual-source CT angiography. The rest of the coronary anomalies in our group of patients were of essentially academic interest only.
The second important finding of this adult population of patients is the relatively low incidence of significant morbidity and no mortality associated with the malignant CAA. Only the two individuals who participated in extreme sports did experience significant symptoms, one of whom had a malignant LC anomaly. This anomaly is the most frequently associated with sudden cardiac death in young athletes.1–3,6,9 The reminder of our patients (mean age = 44 years) had little if any health problems. We believe that when patients are offered appropriate medical management and advice on life style modifications, then there will be no need for surgical intervention, with favourable long-term outcome. This advice is in agreement with previously reported data based on an adult population.9,10 Furthermore, we discouraged surgical intervention in the two young athletes once the diagnosis of CAA of the malignant nature has been made, and instead recommended a significant change in life style. Coronary artery bypass surgery at an early age will almost certainly lead to further interventions in the future. Avoidance of extreme exertion may represent the most important step in preventing sudden cardiac death in the young.
CAA are rare congenital malformations, occurring in about 1%–2% of patients investigated for cardiac symptoms. In this regard, Yamanaka and Hobbs 10 reported the occurrence of CAA in 1686 (1.3%) patients out of 126,595 conventional coronary angiograms performed over 28-year period. Zhang et al. 8 using dual-source CTA reported an incidence of 1.3% of CAA in a population of 1879 Chinese individuals.
Dual-source CTA is possibly the most reliable investigation in diagnosing and defining the course of the coronary arteries when compared to conventional angiography. In this study, 16 patients underwent conventional angiography to further define the significance of coronary artery disease shown on CTA. Of which 10 patients had a malignant CAA course which was not identified by conventional angiography. Although this comparison is based on a small number, it is possible that conventional angiography performed in a busy catheterization laboratory may miss an anatomical variant of CAA. This may not be the case when using CTA which enables 3D reconstruction with visualization of the anomalous artery from differing spatial angles.8,11,12
Conclusion
In this predominant Asian and Middle Eastern population, there is a relatively higher incidence of malignant CAA, with passage of the major aberrant trunk between the two great vessels.
The vast majority of the patients may be managed with life style modification, appropriate risk factor management, and avoidance of surgical intervention.
Footnotes
Acknowledgements
The authors are grateful to M Abdulsamad for the expert help in creating the images. This is not a controlled randomized trial. This research was presented at the following: (1) Poster presentation: 20th Asian Pacific Society of Cardiology Congress Abu Dhabi and XX World Congress of Echocardiography and Allied Techniques 2015 and the 6th Annual Emirates Cardiac Society Congress 2015, Abu Dhabi, United Arab Emirates. (2) Poster presentation: ASCVTS – 23rd Annual Meeting of the Asian Society for Cardiovascular and Thoracic Surgery, 11–14 May, 2015, Hong Kong.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this study because this study was based on electronic data that have already been stored in our servers. They include clinical data and radiological images, and at no time the identities of the patients were exposed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for this study because this study was based on data that already exist in our system.