
Abstract
We report an exceptionally rare case of “Coconut Left Atrium” (LA) presenting with severe mitral stenosis and tricuspid regurgitation. The patient developed acute, refractory symptoms necessitating urgent surgical intervention with mitral valve replacement and tricuspid repair. During the initial surgery, no cleavage plane could be identified in the interatrial septum (IAS), prompting a plan for balloon mitral valvotomy via a surgically created septal access. However, this plan was abandoned upon discovery of a newly formed soft thrombus during reoperation. With limited options remaining, a complete endoatriectomy of the heavily calcified left atrium and IAS was successfully accomplished.
Introduction
Coconut Left Atrium is a rare complication even in long-standing rheumatic valve disease.1–3 Coconut shell is described as complete calcification of the left atrial wall and the interatrial septum.2–5 The term “Porcelain LA” refers to extensive calcification of the left atrial appendage, free wall, and mitral apparatus, typically sparing IAS. 2 Most reports use Coconut LA interchangeably with Porcelain LA, but fewer than ten cases show true Coconut LA with septal involvement. Although left atrial endoatriectomy is commonly performed to peel off the calcium from the left atrial wall, it is generally done in cases with adequate sparing of the interatrial septum. In coconut LA where IAS is densely calcified, surgical intervention is undesirable due to ensuing complications. 1 3–5 This distinguished case report describes a rare presentation of Coconut LA, complicated by soft thrombus, that was managed surgically by complete left endoatriectomy of the LA wall and the IAS followed by mitral valve replacement and tricuspid repair.
Clinical Summary
A 48-year-old female with critical mitral stenosis in New York Heart Association class four was referred to us for mitral valve replacement (MVR). Her Transthoracic echocardiography (TTE) revealed critical calcific mitral stenosis and severe tricuspid regurgitation with pulmonary arterial hypertension. The mitral valve area was 0.4 cm2 with a peak transvalvular gradient of 27 mm Hg. A peculiar finding of dense calcification was captured by TTE. The calcific deposits surrounded the entire left atrium including the IAS that appeared as a coconut shell. The x-ray and computed tomography of the chest supported the TTE findings (Figure 1, Supplementary figure 1). Since the patient had refractory congestive heart failure, we scheduled her for MVR and tricuspid valve repair.
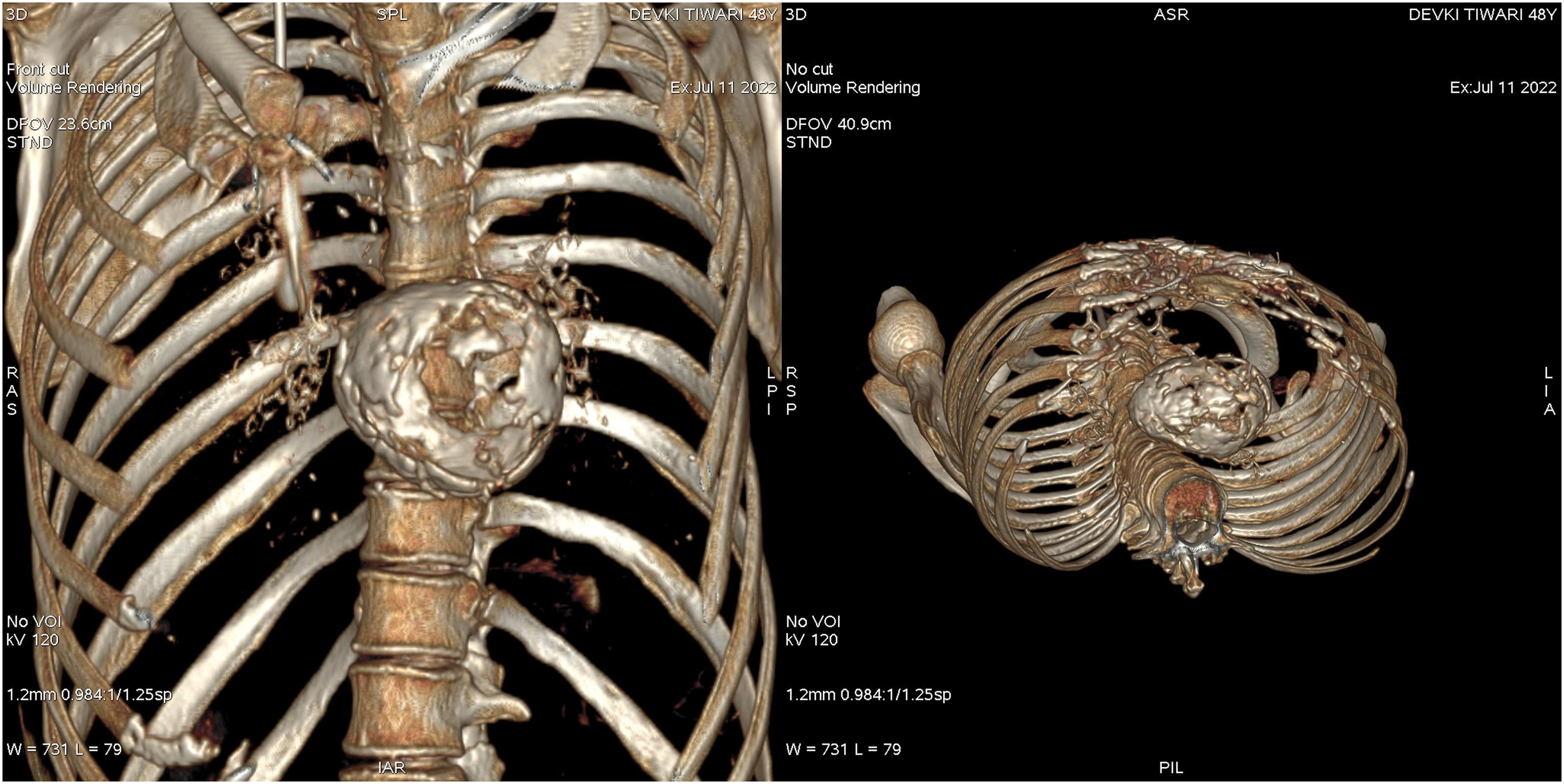
V Preoperative volume-rendered computed tomography (CT) demonstrates dense, circumferential calcification of the left atrial wall and interatrial septum, consistent with a coconut LA. The imaging depicts transmural involvement, explaining the technical challenge encountered during the initial operation.
In the operating room (first sternotomy), the entire LA was calcified, and palpated as a hard, rock-like structure. Similarly, the IAS was hard and rigid when manipulated through the right atrial wall (Supplementary figure 2). Although the finding was anticipated, the interatrial septum proved far more densely calcified than expected. With no discernible or safe plane for entry, the procedure had to be abandoned.
Following multidisciplinary discussion, two alternative strategies were outlined. The first involved balloon mitral valvotomy through a surgically created septal window to be closed later with an atrial septal defect device, combined with tricuspid valve repair. The second involved a retrograde balloon mitral valvotomy via the aortic root, followed by tricuspid repair.
Four days later, the patient was taken into the operating room to execute the planned approach. Surprisingly, the intraoperative echocardiogram unveiled a large amount of soft thrombus within the left atrium which was absent during the first sternotomy (Figure 2). The only option left was to forcefully enter the LA through IAS by breaking the calcium, evacuate the soft thrombus, replace the mitral valve, and probably close the defect with an ASD device. So, we dissected the IAS by utilizing number 11 knife, rongeur, bone nibbler and blunt and sharp dissecting instruments. After entering the LA, the mitral valve was not appreciable due to complete obstruction of the view from the heap of calcified thrombus. Therefore, we proceeded with endoatriectomy of the LA to remove the calcium in piece meal (Figure 2). As we progressed, the soft thrombus was evacuated, and we were able to achieve complete decalcification from both IAS and LA wall. Mitral valve replacement was done with a bioprosthetic valve. Subsequently, it was easy to reconstruct the septum with an autologous pericardial patch and the surgery was completed with tricuspid valve repair. The patient was weaned off bypass and had a smooth postoperative course. Her repeat echocardiogram showed normally functioning mitral prosthesis, no tricuspid regurgitation and decalcified left atrium (Figure 3). At 10-month follow up, the echo demonstrated no mitral regurgitation and no tricuspid regurgitation (Supplementary figure 3).
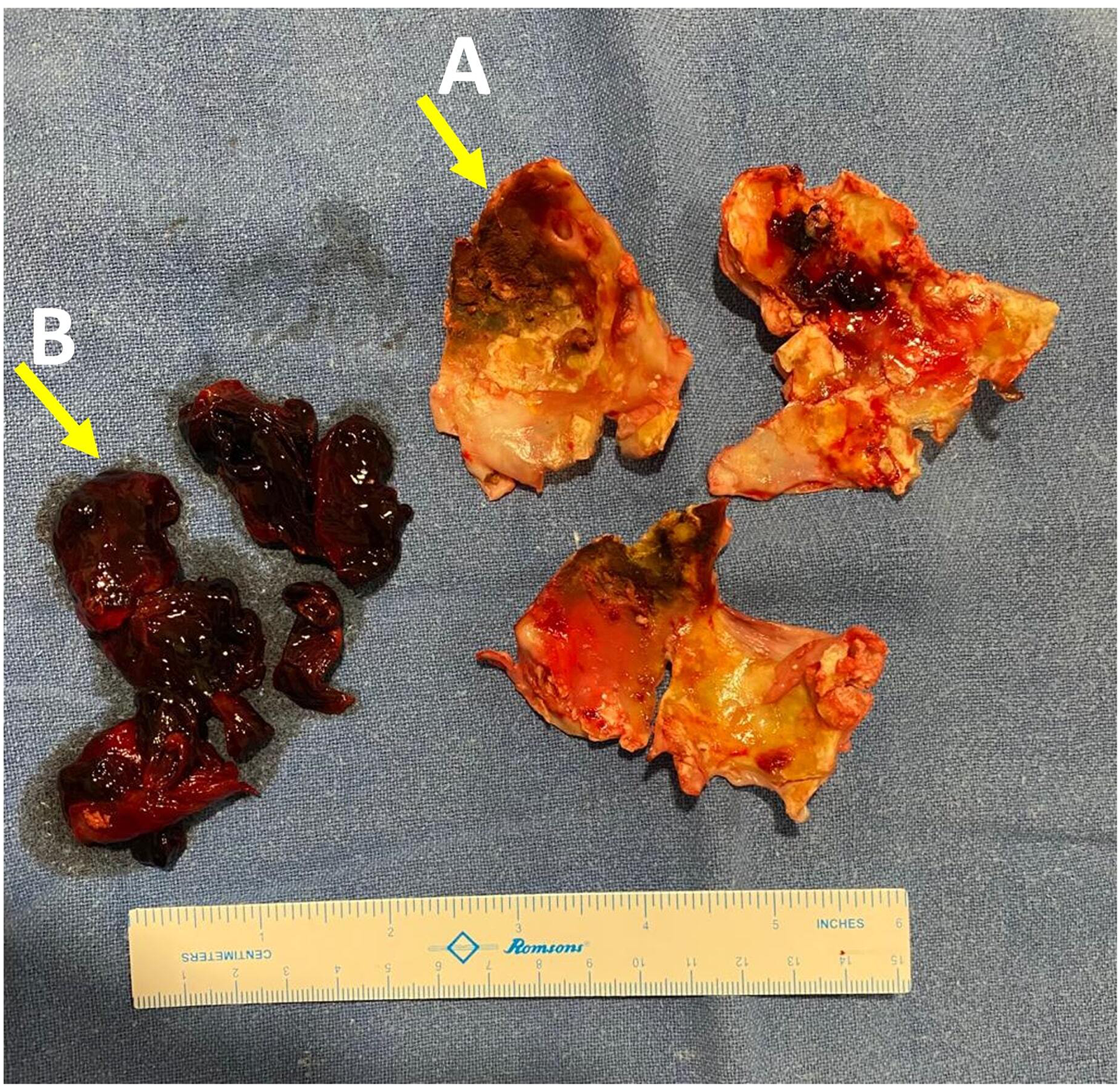
A: Calcium shell cored out from LA wall and IAS in piece meal during endoatriectomy B: Soft thrombus evacuated from LA after entry through the calcified septum.
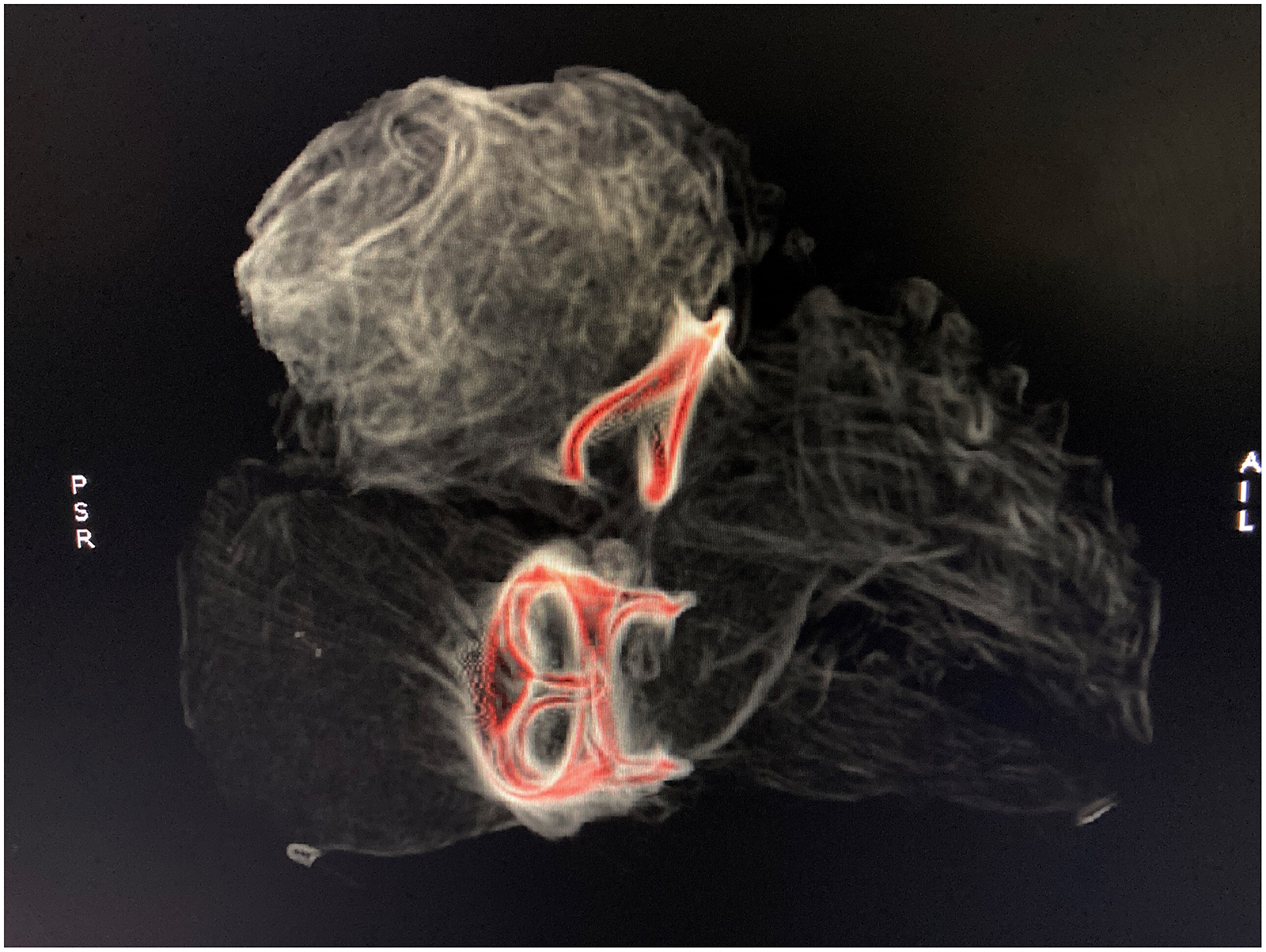
Postoperative computed tomography scan demonstrating complete removal of calcium shell, presence of mitral valve bioprosthesis, and tricuspid ring. The scan confirms successful restoration of atrial cavity morphology and absence of residual calcification or thrombus.
To summarize, the surgical course involved an initial sternotomy that was abandoned due to extensive septal calcification, followed by formulation of alternative strategies and a subsequent reoperation prompted by newly detected atrial thrombus.
Comments
The term “Coconut LA” is used for patients who present with complete transmural calcification of LA along with interatrial septal calcification. “Porcelain LA” describes extensive calcification of the entire LA appendage, free wall, and mitral valve apparatus that spares the IAS.2,4,5 Despite calcification of LA being common with rheumatic disease, it is still rare for a patient to present with a completely calcified LA and interatrial septal wall.1,4 It is important to note that LA endoatriectomy is generally indicated when IAS is spared. Current literature suggests choosing endoatriectomy for porcelain LA that spares the IAS.1,3,4 For transmural calcification that involves the IAS, surgical approach has been avoided and recommended against due to poor success rates.1,4,5 In addition to the challenge of finding a cleavage plane,1,4 there is also an increased risk of embolization and hemorrhage during the procedure. 4 In our case, the patient had critical mitral stenosis, which favored us by limiting the propagation of soft clot and calcium during endoatriectomy.
Upon reviewing literature, we identified one successful surgery on coconut LA. Tsumaru et al, attempted endoatriectomy by accessing the IAS which resulted in an uneventful postoperative course and good outcome. 6 Our case was distinctive due to associated severe tricuspid regurgitation and it was further complicated by the development of soft thrombus which became apparent on echocardiogram during reoperation.
The most likely explanation for the development of soft thrombus was due to stopping Acenocomarol before surgery. We did not restart anticoagulant after the first sternotomy since we were planning to reoperate emergently due to unstable hemodynamics of the patient. In patients with severely calcified and low compliance left atria, even short periods without anticoagulation can promote blood stasis and thrombus formation. This highlights the importance of carefully managing anticoagulation bridging and timing of surgery in high-risk rheumatic etiology to prevent new thrombus development during the perioperative window. Nonetheless, we managed to remove calcium in its entirety, successfully replace the mitral valve and repair the tricuspid valve. The patient fared well after surgery and was discharged on the fourteenth postoperative day.
Our ability to successfully operate and make quick decisions can be credited to multiple factors. Firstly, our department frequently witnesses patients with rheumatic heart disease with a wide spectrum of presentations. Institutional expertise in handling complicated mitral valves with rheumatic etiology is essential. Secondly, collaborative planning and discussions with the team could achieve better outcomes. Finally, we believe that the surgeon's experience, skill, and adeptness remain imperative while addressing such complications. We recommend optimization of medical therapy in patients with coconut LA if they respond well. Due to the risks involved, we do not advocate surgical intervention unless the patient presents acutely, and there is availability of skilled team that is seasoned in managing complex rheumatic valve cases. To our knowledge this is the first report of successful MVR and tricuspid repair in a patient of coconut LA with dense calcification of the entire LA and IAS that was complicated by a soft thrombus.
Supplemental Material
sj-jpg-1-hvs-10.1177_30494826261425223 - Supplemental material for Complete Endoatriectomy of Coconut Left Atrium with Mitral Valve Replacement and Tricuspid Repair
Supplemental material, sj-jpg-1-hvs-10.1177_30494826261425223 for Complete Endoatriectomy of Coconut Left Atrium with Mitral Valve Replacement and Tricuspid Repair by Shashwat Shrivastava, Sandeep Shrivastava, A.B. Gopalamurugan, Shipra Shrivastava and Shitij Shrivastava in Journal of the Heart Valve Society
Supplemental Material
sj-jpg-2-hvs-10.1177_30494826261425223 - Supplemental material for Complete Endoatriectomy of Coconut Left Atrium with Mitral Valve Replacement and Tricuspid Repair
Supplemental material, sj-jpg-2-hvs-10.1177_30494826261425223 for Complete Endoatriectomy of Coconut Left Atrium with Mitral Valve Replacement and Tricuspid Repair by Shashwat Shrivastava, Sandeep Shrivastava, A.B. Gopalamurugan, Shipra Shrivastava and Shitij Shrivastava in Journal of the Heart Valve Society
Supplemental Material
sj-jpg-3-hvs-10.1177_30494826261425223 - Supplemental material for Complete Endoatriectomy of Coconut Left Atrium with Mitral Valve Replacement and Tricuspid Repair
Supplemental material, sj-jpg-3-hvs-10.1177_30494826261425223 for Complete Endoatriectomy of Coconut Left Atrium with Mitral Valve Replacement and Tricuspid Repair by Shashwat Shrivastava, Sandeep Shrivastava, A.B. Gopalamurugan, Shipra Shrivastava and Shitij Shrivastava in Journal of the Heart Valve Society
Footnotes
Informed Consent
Informed consent has been obtained for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB
IRB exemption was obtained for this case report.
Supplemental Material
Supplemental material for this article is available online.