
Abstract
Introduction
In recent years, major findings on concomitant procedures and anticoagulation management have occurred in Mitral Valve (MV) surgery. Therefore, we sought to evaluate the current practices in MV interventions across Europe.
Methods
In October 2021, all national cardio-thoracic societies in the European region were identified following an electronic search and sent an online survey of 14 questions to distribute among their member consultant/attending cardiac surgeons.
Results
The survey was completed by 91 consultant/attending cardiac surgeons across 12 European countries, with 78% indicating MV repair as their specialty area. 57.1% performed >150 operations/year and 71.4% had 10+ years of experience.
Concomitant tricuspid valve repair is performed for moderate tricuspid regurgitation (TR) by 69% of surgeons and for mild TR by 26.3%, both with annular diameter >40 mm. 50.6% indicated ischaemic MV surgery in patients undergoing CABG if moderate mitral regurgitation with ERO >20 mm2 and regurgitant volume >30 mL, and 45.1% perform it if severe MR with ERO >40 mm2 and regurgitant volume >60 mL. For these patients the preferred management was: MVR if predictors of repair failure identified (47.2%) and downsizing annuloplasty ring only (34.1%).
For atrial fibrillation (AF) in cardiac surgery, 34.1% perform ablation with biatrial lesion and 20% with left sided only. 62.6% perform concomitant Left Atrial Appendage (LAA) Occlusion irrespective of AF ablation with a left atrial clip. A wide variability in anticoagulation strategies for MV repair and bioprosthetic MV valve was reported both for patients in sinus rhythm and AF.
Conclusion
These results demonstrate a variable practice for MV surgery, and a degree of lack of compliance with surgical intervention guidelines and anticoagulation strategy.
Introduction
Recent advances in mitral valve (MV) intervention have improved patients’ outcomes through multiple technological innovations. The impact of peri and post-operative management and comorbidities has been influential for long-term durability and improved quality of life.
Tricuspid valve (TV) regurgitation is a common finding among patients with moderate-severe mitral valve regurgitation (MR), with its incidence in this cohort being around 30%. 1 Wide variation in the practice of concomitant TV surgery at the time of MV.surgery has been reported, ranging anywhere from 5% to 75%. The recent randomized controlled trial by Gammie and colleagues. 2 illustrated the advantage of concomitant TV annuloplasty in patients undergoing MV surgery, demonstrating improvement on a 2-years follow-up of a composite of death, reoperation for TV regurgitation and its progression. Similarly, coronary artery disease (CAD) is present in a significant proportion of patients with MV disease, with around 40% of ischaemic MR and approximately 15% to 20% of non-ischaemic MR patients undergoing concomitant coronary artery bypass grafting (CABG).3,4 In patients with moderate ischemic MR, the Randomized Ischemic Mitral Evaluation (RIME) Trial reported that adding CABG to MV annuloplasty leads to improved outcomes when compared to CABG alone. 5 Atrial fibrillation (AF) is present in 30%–50% of patients undergoing mitral valve surgery and is associated with long-term mortality and morbidity. 6 Surgical ablation for AF during MV surgery has been demonstrated to be an effective method of lowering the incidence of AF (6). The recent Left Atrial Appendage Occlusion Study (LAAOS III) has shown a significant advantage in reducing the rate of postoperative stroke of LAA occlusion during MV surgery. 7 Finally, anticoagulation therapy remains crucial for the effective postoperative management of patients undergoing both MV repair and replacement with bioprosthetic valve.
Despite trials widening our understanding and guidelines undergoing regular updates, the reality of their application in the operating theatre on a routine basis is to be explored. Our survey reviewed these concomitant interventions and explored them in view of recent trials.
Evidence in the form of guidelines and clinical trials give us a path which we want to establish as practice. However, the adherence to such guidelines is to be explored. The often-reduced formal national educational curriculum on the mitral valve and the dynamic status of this valve, decision-making in its interventions and management remain in the hands of expert centres.
Therefore, the status of mitral valve intervention in the United Kingdom and Europe has not been fully explored. In light of the complexity surrounding mitral valve interventions, and the variation across centres in Europe, we undertook a survey to understand the spectrum of practice variability.
Methods
A nucleus group of experts and interested individuals (V.N., A. AR., J.C, G.L, J.A., P.P.P.) formulated a survey of questions which was distributed to the relevant national cardiothoracic organisations in Europe. In October 2021, all national cardio-thoracic societies in the European region were identified following an electronic search and sent an online survey of 14 questions (Supplementary File 1) to distribute among their member consultant/attending cardiac surgeons.
The questions encompassed 4 main areas of focus in the realm of mitral valve (MV) surgery: anticoagulation plan following mitral valve repair and replacement with bioprosthetic valve; indications for performing concomitant tricuspid valve repair; indications and management of intervention on the ischaemic mitral valve in patients undergoing coronary artery revascularisation surgery; concomitant atrial fibrillation (AF) ablation and concomitant Left Atrial Appendage Occlusion irrespective of AF ablation in patients with AF. Data was also collected regarding the surgeon’s country of practice, gender, years of practice as an attending cardiac surgeon, cardiac operative volume per year and area of subspecialty within cardiac surgery. All data were recorded on a central database and analysed.
Data analysis
Results are reported as percentages or mean and standard deviation values. Differences between groups for categorical variables were analysed by using a Chi-squared test while for continuous variables t test or Fisher’s exact test were used as appropriate. All statistical analyses were performed by using IBM SPSS version 27 (IBM Corp., Chicago, IL, USA). A p-value of less than 0.05 was considered to indicate statistical significance.
Results
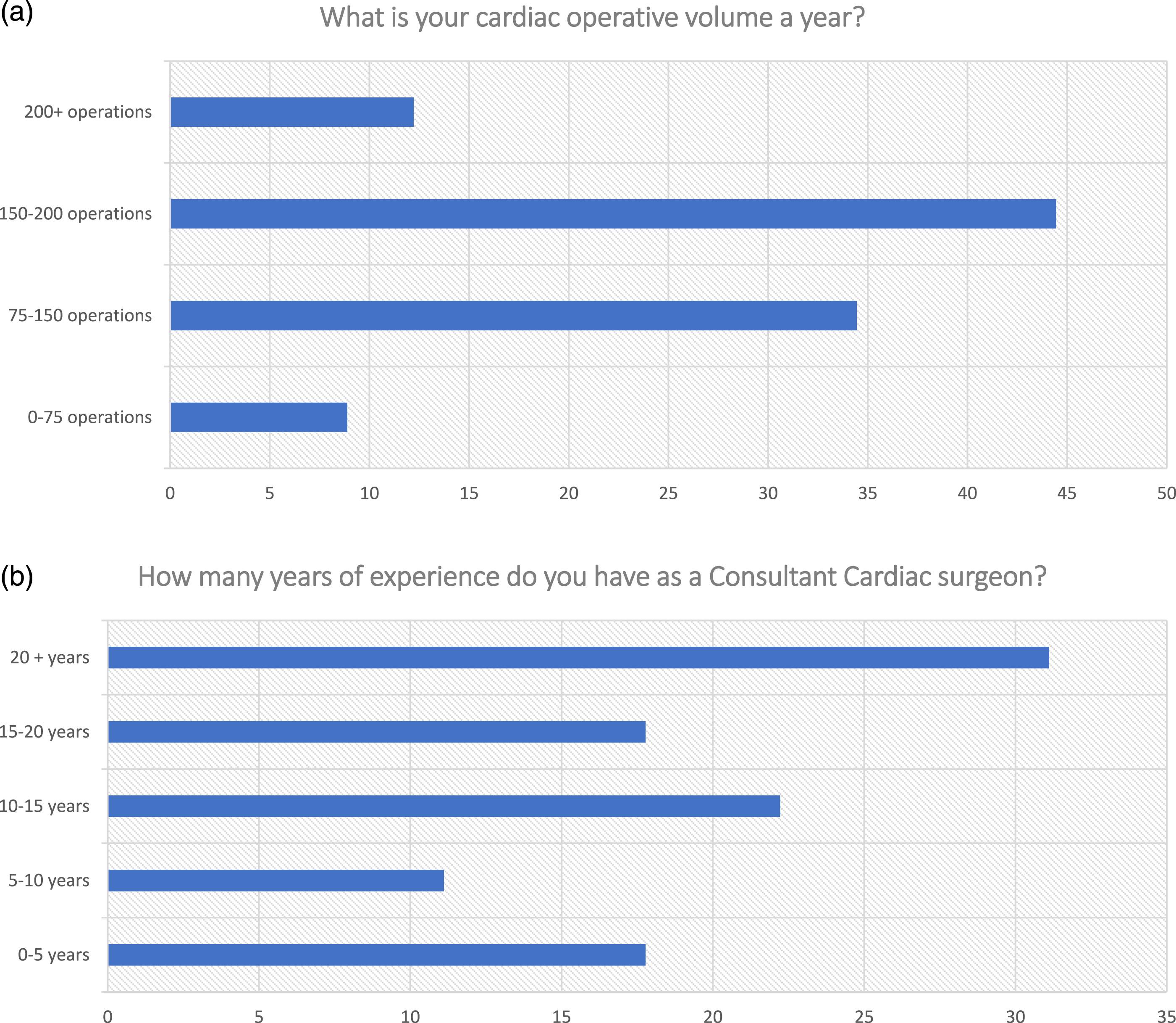
A positive response was received by 91 attending/consultant cardiac surgeon in 12 European countries, including: Belgium, Finland, France, Germany, Ireland, Portugal, Moldova, Italy, Russia, Switzerland, Turkey and the United Kingdom (Figure 1). Mitral valve surgery was indicated as an area of expertise by 78% of surgeons (71/91). Out of the whole cohort, 71.4% of surgeons (65/91) reported 10+ years of experience as consultant cardiac surgeons, and 57.1% (52/91) performed >150 operations/year (Figure 2). 54.9% of the consultants worked in the UK, potentially representing national practices. Map of respondent countries. Characteristics of respondents.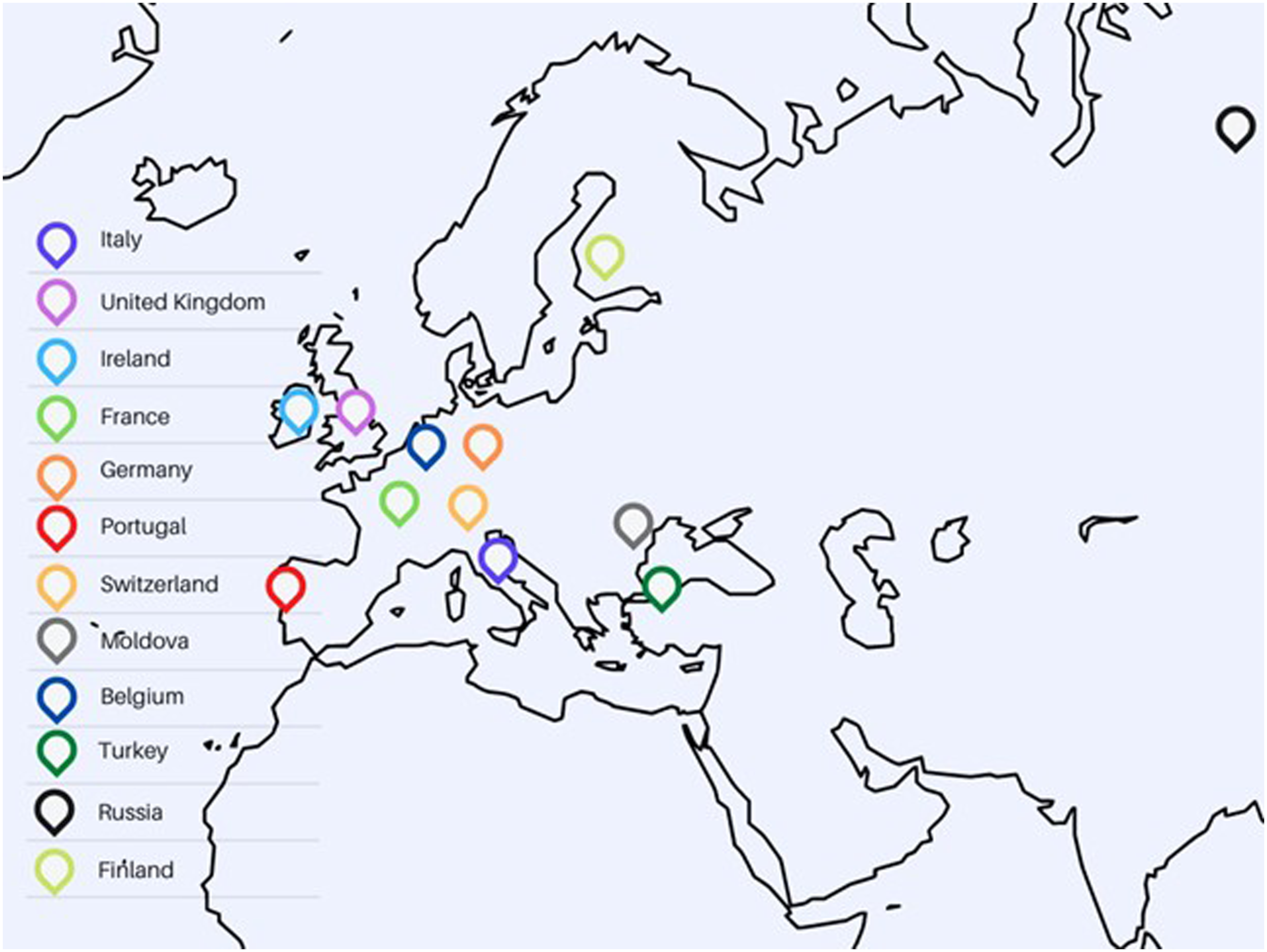
Concomitant tricuspid valve surgery
Concomitant tricuspid valve repair in patients undergoing mitral valve intervention is performed for moderate tricuspid regurgitation (TR) by 69% of surgeons and for mild TR by 26.3%, both with an annular diameter >40 mm. Severe TR only was an indication for tricuspid valve repair by 4.4% of the surgeons (Figure 3). Swiss and UK surgeons constituted the only groups which indicated severe TR only as indication (50% of responses per group). TV repair during MV surgery.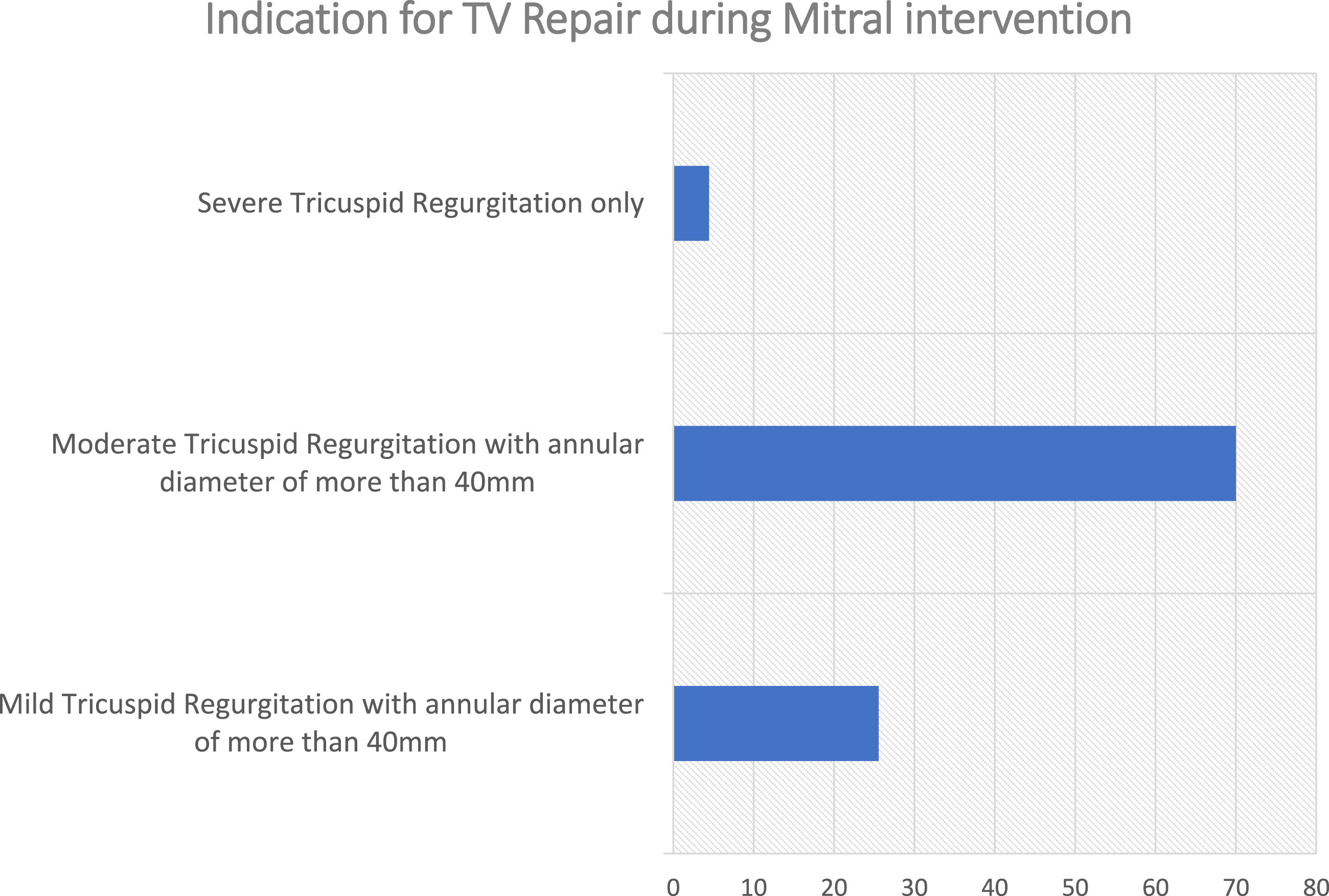
Concomitant atrial fibrillation ablation during mitral valve surgery
Most surgeons routinely perform concomitant Atrial Fibrillation Ablation in patients undergoing cardiac surgery with AF with 34.06% performing ablation with biatrial lesions, 23.08% with left-sided only, 20% perform pulmonary vein isolation only, however 23.1% do not perform any ablation but only left atrial appendage occlusion (Figure 4(b)). Interestingly, of the surgeons performing over 150 operations per year, only 18.5% (10/54) do not perform ablation, while in those performing <150 operations per year 30.8% (12/39) do not perform ablation (p = .145). Among respondents from Portugal 80% indicated not performing ablation, only LAA closure, while in the UK this was 18% of respondents. AF ablation and LAAO during cardiac surgery.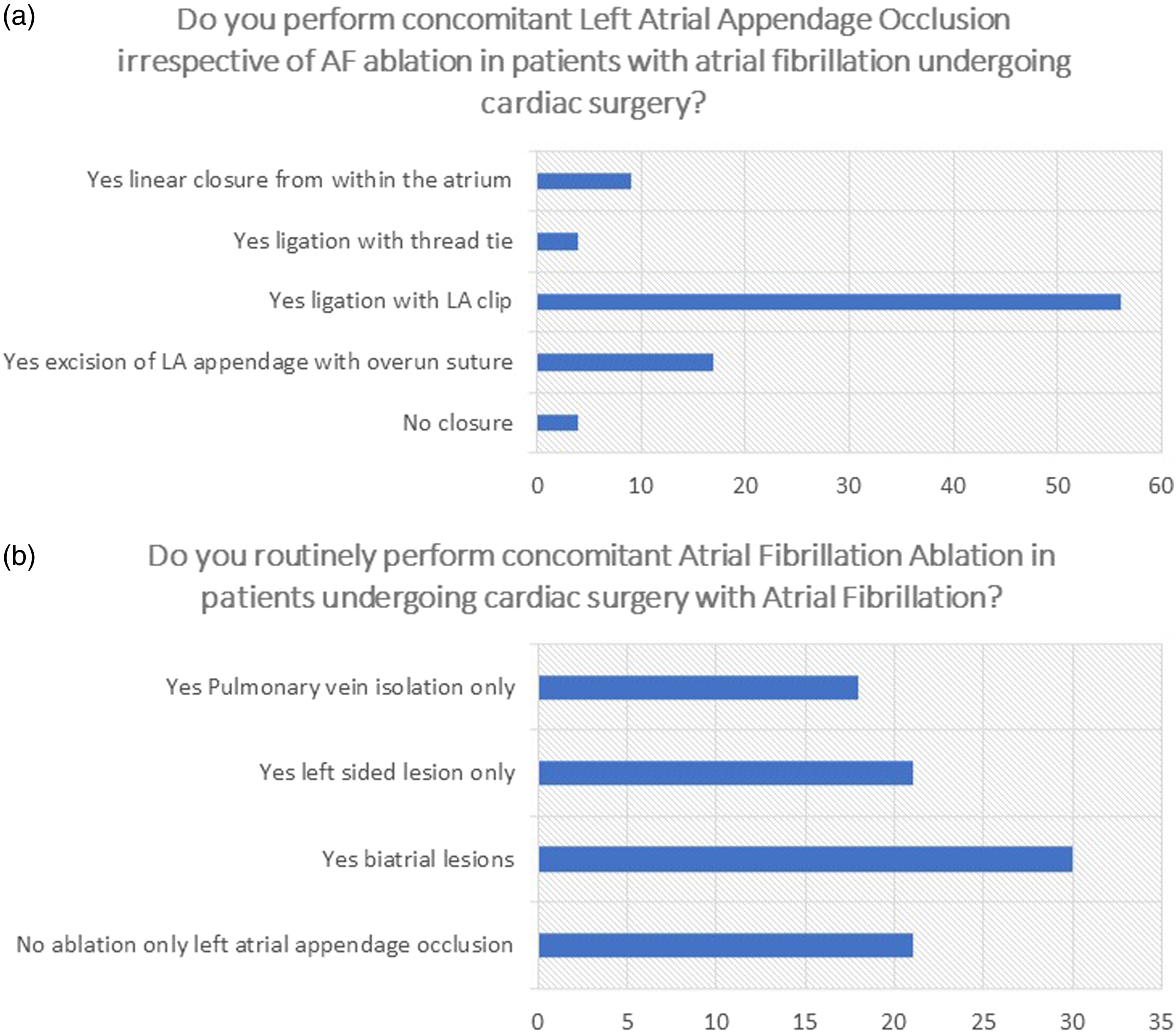
Concomitant left atrial appendage occlusion during mitral valve surgery
Concomitant Left Atrial Appendage Occlusion irrespective of AF ablation in patients with atrial fibrillation undergoing cardiac surgery is performed by 62.6% with a left atrial clip, 18.7% perform excision of LAA with overrun suture, 9.9% perform linear closure from within the atrium, 4.4% perform ligation with a thread tie, and 4.4% do not perform closure (Figure 4(a)). Of interest, 58.3% of Belgian surgeons reported using excision of LAA with overrun suture versus 6% of UK surgeons. In fact, 86% of UK surgeons and 64% of Swiss surgeons reported using the LAA clip. Overall, across Europe (excluding the UK), LA clip is chosen by 34% of surgeons.
Concomitant coronary artery surgical revascularisation for the ischaemic mitral valve
50.6% of the surgeons reported the indication for intervention on the ischaemic mitral valve in patients undergoing coronary artery revascularization to be moderate mitral regurgitation with ERO >20 mm2 and regurgitant volume >30 mL. 45.05% perform it in the presence of severe MR with ERO >40 mm2 and regurgitant volume >60 mL, while the remaining 4.4% of surgeons perform concomitant CABG in the presence of evidence of worsening severity of ischaemic MR on stress dobutamine/exercise echocardiogram (Figure 5(a)). Ischaemic MV surgery during CABG.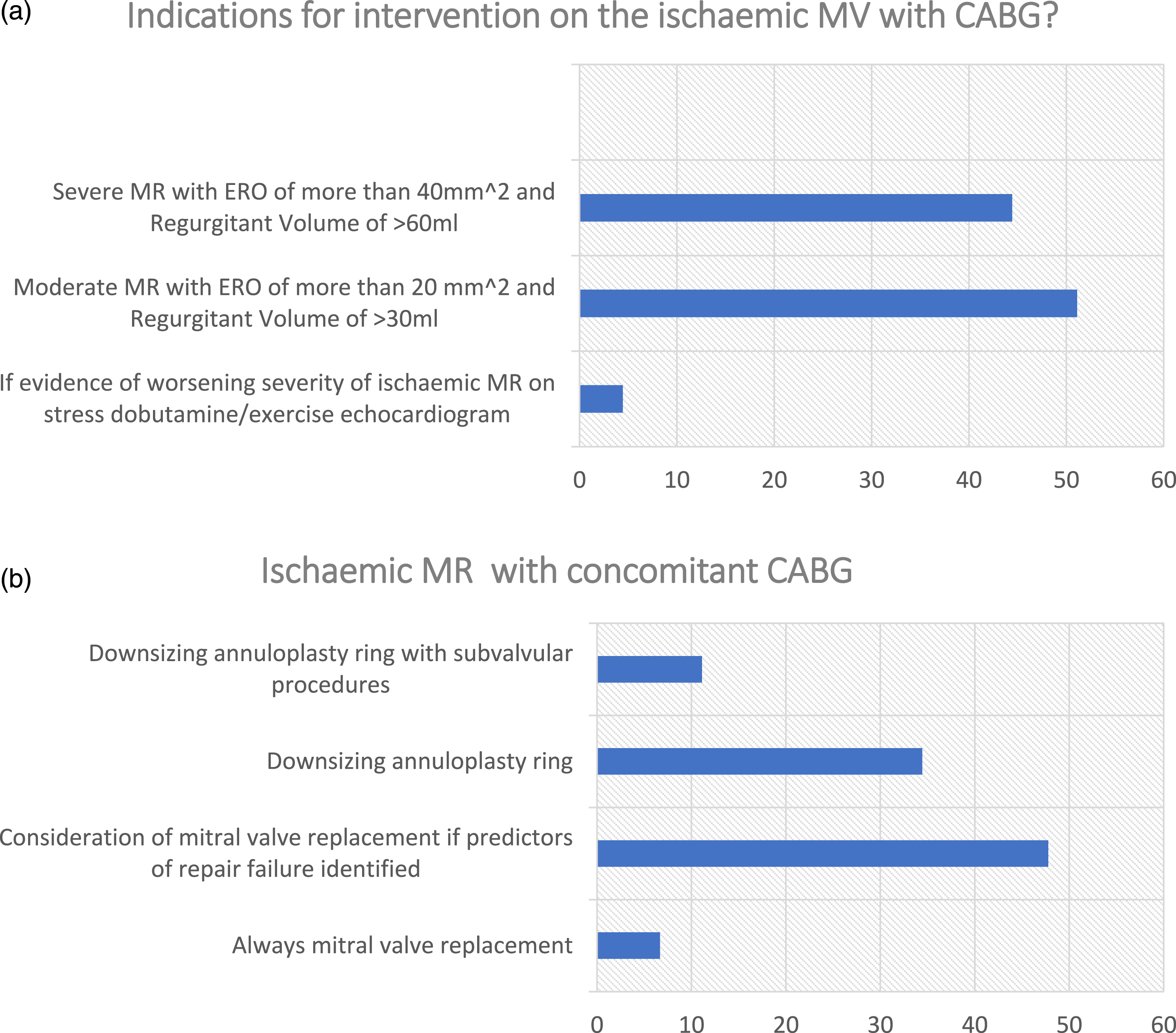
The preferred method of management for ischaemic MR concomitantly in patients undergoing CABG was mitral valve replacement if predictors of repair failure were identified (47.2%), downsizing annuloplasty ring (34.1%) with additional subvalvular procedures (12.1%). 6.59% of the surgeons reported always performing mitral valve replacement in these patients (Figure 5(b)). Interestingly, 34.6% of surgeons with 0–10 years’ experience prefer downsizing annuloplasty ring ± subvalvular procedure, against 50.7% of those with 10+ years’ experience, although the difference was not statistically significant (p = .183). In the UK 52% of surgeons preferred MV replacement if predictors of repair failure identified, versus 41.5% in the rest of Europe. 40% of UK surgeons versus 53.7% in the rest of Europe reported choosing downsizing MV annuloplasty ± subvalvular procedures.
Post-operative anticoagulation in mitral valve surgery
Mitral valve repair
For patients with sinus rhythm undergoing mitral valve repair, the respondents reported a 24.1% use of Aspirin while 47.3% used Vitamin K antagonist (VKA), both alone for 3 months only. The remaining respondent described using only lifelong aspirin (7.6%), DOAC in the initial 3 months only (4.4%), VKA plus aspirin for 3 months only (5.5%), vitamin K antagonist for 3 months and then lifelong aspirin (3.3%), no anticoagulation (4.4%). VKA alone for 3 months only was the preferred option by 80.5% of the surgeons in Europe versus 20 % in the UK. Conversely, 40% of UK surgeons preferred Aspirin only for 3 months, versus 4.9% in the rest of Europe.
In patients with atrial fibrillation (AF) undergoing repair the surgeons reported a 29.7% use of DOAC for life and 20.8% of VKA for life, and 35.1% use VKA for 3 months followed by DOAC for life, 6.6% Vitamin Antagonist plus Aspirin for 3 months followed by Direct Oral Anticoagulants for life, 3.3% VKA and aspirin for 3 months and then VKA for life (Figure 2). The remaining respondents were miscellaneous of those options. 44% of the surgeons in the UK indicated the use of DOAC for life versus 12.2% of surgeons in Europe, where 48.8% reported VKA for 3 months followed by DOAC for life as preferred option.
Mitral Valve replacement with bioprosthetic valve
For patients with sinus rhythm undergoing mitral valve replacement with a bioprosthetic valve, the respondents reported a 46.2% use of VKA and 15.4% use of Aspirin, both alone for 3 months only. The remaining respondent described using DOAC in the initial 3 months only (3.3%), VKA plus aspirin for 3 months only (7.7%), lifelong aspirin only (7.6%), DOAC in the initial 3 months and then long term (3.3%), no anticoagulation (4.3%) (Figure 6). The remaining respondents were miscellaneous of those options. Interestingly, 24% of UK surgeons versus 4.9% in the rest of Europe reported using Aspirin alone for 3 months only. 70% of surgeons in Europe indicated VKA for 3 months only as their choice, versus 26% in the UK where the rest of responses were heterogeneous. Anticoagulation during Mitral valve Surgery.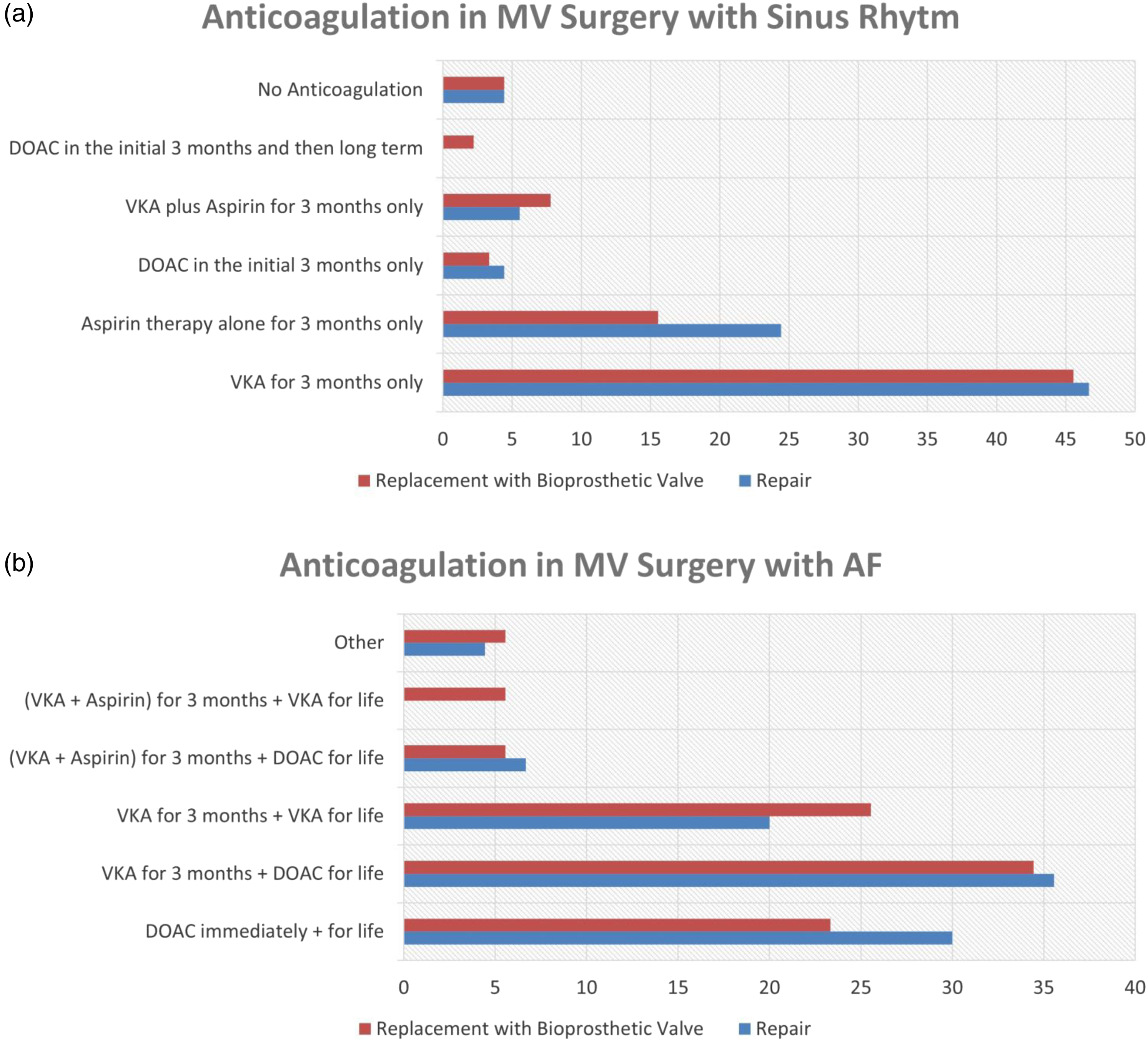
In patients with atrial fibrillation, the surgeons reported a 23.08% use DOAC for life, 26.4% use VKA for life, and 34.07% use VKA for 3 months followed by DOAC for life, VKA and aspirin for 3 months and then VKA for life (5.49%), VKA and aspirin for 3 months and then DOAC for life (5.49%) (Figure 6).
For both mitral valve repair and replacement with a bioprosthetic valve in patients with sinus rhythm, a high proportion of surgeons selected the option “other”, 14.2% for repair and 20.8% for replacement. All of these respondents reported using for both procedures either Aspirin lifelong or VKA for 3 months followed by Aspirin for 3 months. 38% of UK surgeons use DOAC for life versus 4.9% in the rest of Europe, where 34.1% use VKA for life (vs 20% in the UK).
Discussion
Concomitant tricuspid valve surgery
The management of concomitant procedures during mitral valve surgery remains a multifaceted topic with controversial study findings and great variability in practice, as also outlined by our findings. Firstly, patients affected by mitral valve pathology often present with a diseased tricuspid valve as well,8,9 bringing onto the discussion table the need for concomitant tricuspid surgery at the time of MV repair. While most of the current evidence with regards to concomitant TV surgery remains based on data from observational studies, a broad consensus has been reached on the need for surgery in the setting of severe TV regurgitation (grade III-IV) at the time of MV surgery.10–12 The recent ESC/EACTS guidelines of 2021 classify the latter as a class I recommendation with level of evidence C (13). However, the debate mainly remains open with regards to mild-moderate and moderate TV regurgitation, with the guidelines and observational data suggesting that TV surgery should be considered with mild or moderate TV regurgitation with a dilated annulus (annular diameter >40 mm).10–13 Only 4.3% of the respondents indicated Severe TR only to be an indication for concomitant TV surgery, while 70% indicated moderate TR with dilated annulus as an indication. Although improved outcomes and lower disease progression have been reported with TV repair for moderate or less than moderate concomitant surgery, concerns remain. These concerns mainly regard the need for permanent pacemaker implantation, longer cardiopulmonary bypass times and the possible need to replace in case of TV repair failure.14–16 A recent randomized controlled trial by Gammie et al. of 401 patients has, however, demonstrated that concomitant TV repair for moderate/less than moderate TR at the time of MV repair could lead to lower 2-year mortality and TR progression. 2
Concomitant atrial fibrillation ablation during mitral valve surgery
Surgical patients undergoing mitral valve surgery may be adequate candidates for surgical AF ablation, with the main intent of lowering the long-term risks of stroke. Up to date, surgical ablation for AF during MV surgery has been demonstrated to be an effective method of lowering the incidence of AF in these patients.6,17,18 However, no short-term survival benefit has been yet demonstrated, with an increased reported risk of permanent pacemaker implantation.6,17–19 In our study 23.1% of respondents do not perform any ablation but only left atrial appendage occlusion. The second level of uncertainty is added by the choice of lesion set ablation. Pulmonary vein isolation represents the simplest technique and is performed by 19.7% of surgeons in our study. Biatrial lesions ablation which is performed by 34.1% of surgeons in our study, usually takes a longer CBP time and requires right and left atriotomies. The randomized study by Gillinov et al. reported no significant difference between the two techniques in terms of freedom from AF (6).
Concomitant left atrial appendage occlusion during mitral valve surgery
The recent Left Atrial Appendage Occlusion Study (LAAOS III) recently investigated the benefit of left atrial appendage (LAA) occlusion during cardiac surgery and demonstrated a lower risk of ischemic stroke and systematic thromboembolism in the group receiving LAAO (7). Our results demonstrated that the preferred methods of LAAO are in 62% a left atrial clip, and in 18.5% excision of LAA with overrun suture. It is of concern that following the recent findings, 4.3% of the surgeons reported not closing the LAA during cardiac surgery, which could potentially expose the patients to an unnecessarily increased risk of debilitating complications. The current ESC/EACTS guidelines do indeed recommend LAAO in cardiac surgical patients with a level of recommendation IIa and evidence level B (13). It is of interest to also note that our results show over 62.6% of the respondents using a left atrial clip which contrasts with the LAOOS III Trials use of 15.1%, in which the majority (55.7%) used the cut and sew technique. 7 This could be explained through the relatively easier application of the clip and its possible increased used following the release of the above mentioned trial.
Concomitant coronary artery surgical revascularisation for the ischaemic mitral valve
The surgical intervention on the ischemic mitral valve remains another area of open debate with contradicting evidence published in the literature. Ischemic MR results from the reverse remodelling of the left ventricle as a consequence of myocardial infarction, most often distinguished from primary functional MR by the presence of an infarcted myocardium but normal leaflets. Generally, the appropriateness of the surgical approach has to be patient-centred, and the decision is to be taken by a dedicated Heart Team. Severe MR in patients undergoing CABG has been recommended for MV surgery. 13 MV repair through the use of a rigid ring has been shown to result in symptomatic improvement and LV reverse remodelling. 20 Careful attention should be paid to the increased risk of ring dehiscence posed by complete rigid annuloplasty rings in the setting of ischemic MR. 21 On the other hand, a randomized controlled trial published by the Cardiothoracic Surgical Trials Network, found no additional survival and outcome benefit at 2 years for the surgical repair of moderate MR in patients undergoing CABG (22). Similar results in terms of mortality at 30 days and 1 year was reported by the Randomized Ischemic Mitral Evaluation (RIME) Trial group, 5 who demonstrated no difference upon the addition of MV repair to CABG in moderate ischemic MR patients. Nevertheless, the study did report that the addition of MV annuloplasty to CABG might improve left ventricular reverse remodelling, MR severity, and functional capacity when compared to CABG alone. 5 The current evidence clearly contrasts our data which demonstrated 50.4% of the surgeons reporting the indication for intervention on the ischaemic MV in patients CABG to be moderate mitral regurgitation with ERO >20 mm^2 and regurgitant volume >30 mL. 22
In cases where MV surgery was decided to be carried out concomitantly to CABG, surgeons preferred mitral valve replacement if predictors of repair failure were identified (47.2%) and downsizing annuloplasty ring (46.1%), demonstrating a variability in practice. The preferred intervention on the mitral valve in ischemic MR remains a matter of controversy up to date, which is also indicated by the results of the data collected in our study. Acker and colleagues 23 randomly assigned 251 patients to either MV replacement or MV repair in order to compare the efficacy and safety of both treatments. No significant difference in left ventricular reverse remodelling and survival were found at 1 year between patients undergoing MV repair or MV replacement, with MV repair having higher rates of moderate-severe MR reoccurrence. Their results came at great contrast to the available results from observational studies, which at the time had shown improved outcomes with MV repair, probably due to sicker patients undergoing MV replacement. 23 In particular more surgeons with more than 10 years of experience preferred to use downsized annuloplasty ring ± subvalvular procedure (51.5%) compared to those with less experience (34.6%), however not reaching statistical significance. These techniques are challenging to perform and as our survey demonstrated mostly experienced surgeons perform them. Harmel et al. 24 Conducted a meta-analysis to address that MV annuloplasty alone might not address the underlying LV remodelling in ischaemic MR and suggested that additional subvalvular repair techniques might improve restoring LV geometry. Their results demonstrated that MV annuloplasty ring with additional subvalvular techniques (regardless of technique) was associated with four times significantly lower reoccurrence rate of mitral regurgitation with grade of ≥2 as compared with annuloplasty alone.
Post-operative anticoagulation in mitral valve surgery
Anticoagulation following MV intervention has the main objective of reducing clot formation and a prothrombotic state until the newly implanted prosthetic material is endothelialised, usually 3 months following the operation. 25 Indeed, multiple studies have already demonstrated that both mitral valve repair and replacement with a bioprosthetic valve are associated with an increased risk of thromboembolic events in the short term, 4.6% ± 1.5% for replacement and 1.5% ± 0.4% for MV repair. 25 Furthermore, MV surgery has been associated with an elevated risk of AF development, with around one-third of the patients developing this debilitating condition. 26
With regards to anticoagulation therapies for mitral valve interventions, the results of our study have demonstrated a broad variation in practice across surgeons. Firstly, when mitral valve repair in patients with sinus rhythm is considered, 24.1% of the respondents reported using Aspirin while 46.7% used Vitamin K antagonist (VKA), both alone for 3 months only. Interestingly, 4.4% reported not using any form of anticoagulation, 7.6% used lifelong aspirin, 4.4% used DOAC in the initial 3 months, while 5.4% combined both VKA and Aspirin for 3 months, thus clearly showing the broad variation in practice. The most recent ESC/EACTS 2021 guidelines for the management of valvular heart disease recommend using both an oral anticoagulant for the first 3 months, with a level of recommendation IIa and level of evidence C. 13 It must be noted that at present it has been shown that both ASA and VKA present similar incidence of thromboembolic events in the first 3 months after surgery, however, no randomized control trial has been carried out to date.
For patients with AF undergoing mitral valve repair, 30% of surgeons reported using DOAC and 20.8% VKA, both alone for life, while the majority of 34.8% use VKA for 3 months followed by DOAC for life. In patients with AF the current guidelines suggest using long term oral anticoagulation therapy irrespective of other interventions to treat AF.13,27 Data regarding anticoagulation therapy in this population remains inconclusive. The ENAVLE trial enrolling 220 patients undergoing MV repair or replacement with a bioprosthetic valve demonstrated Edoxaban to be non-inferior to VKA for thromboembolism and major bleeding. 28 Sub-group analysis of multiple other trials exploring AF anticoagulation with MV repair all demonstrated non-inferiority or equivalence of DOACs in this population.
For patients with sinus rhythm undergoing MV replacement with a bioprosthetic valve, 45.6% of respondents reported use of VKA and 15.2% use Aspirin, both alone for 3 onths only. As per the ESC/EACTS 2021 guidelines, in these patients, VKA is the preferred method of anticoagulation for the first 3 months following surgery with a recommendation level IIa and level of evidence B (13,31), thus illustrating that 54.4% of our respondents were not compliant with the most recent guidelines including 4.3% not giving any anticoagulation. In particular in our survey it was noted that only 26% of UK surgeons used VKA for 3 months compared to 70% of the European surgeons. Although the evidence within this area remains scarce, real-world data and experience of multiple centres support the guideline recommendation.
In patients with atrial fibrillation undergoing bioprosthetic mitral valve replacement, 23.07% of surgeons reported using DOAC for life, 26.4% using VKA for life, and 34% use VKA for 3 months followed by DOAC for life. Even in this scenario, a high degree of variability in practice and non-compliance to guidelines exists despite the serious long-term implications of AF. Indeed, guidelines recommend a DOAC over VKA after the first 3 months following surgery,13,28 which 37% of surgeons in our survey did not follow. In addition, 38% of UK surgeons used DOAC for life alone compared to only 4.9% in Europe where 34.1% of surgeons used only VKA for life. Patients with a concurrent indication for anticoagulation such as AF, a DOAC is generally preferred for these patients as described by the RIVER trial where patients with AF and undergoing bioprosthetic mitral valve, the incidence of stroke was lower in the rivaroxaban group but mortality from cardiovascular or thromboembolic events and major bleeding were similar to the VKA group. 29
Limitations
The national practices of the individual countries do not represent the responses of individuals in this survey. Although, all respondents of this survey were consultant/attending cardiac surgeons, the number of respondents is limited by the relatively low size, thus limiting our findings, and requiring caution interpretation of the study’s findings. Furthermore, a response was not able to be obtained from all countries in the European region due to a lack of response, therefore, limiting the generalizability of our data to the whole European region.
Conclusion
The following survey evaluated the current practices in the dynamic field of mitral valve interventions across the European region focussing on both the surgical techniques and the perioperative/postoperative management of these patients. Our findings highlighted a wide variability in current practice as well as a degree of non-compliance to current ESC/EACTS guidelines by cardiac surgeons in Europe. Thus, mitral valve surgery risks remaining in the hands of the “experienced” surgeons. Although experience is considered a valuable asset, there remains a great need for more standardization of practices in order to provide patients undergoing mitral valve surgery with the best possible outcomes.
Supplemental Material
Supplemental Material - Concomitant interventions in mitral valve surgery – A European perspective
Supplemental Material for Concomitant interventions in mitral valve surgery – A European perspective by Vinci Naruka, Arian Arjomandi Rad, Jacob Chacko, Guiqing Liu, Jonathan Afoke and Prakash P Punjabi in Perfusion
Footnotes
Acknowledgments
We would like to express our gratitude to all the European Cardio-thoracic Surgery National Societies for the support in disseminating our survey. Special thanks to the Society for Cardiothoracic Surgery in the UK and Ireland (SCTS) and the Swiss Society of Cardiac and Thoracic Vascular Surgery.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.