
Abstract
Background
Transcatheter aortic valve replacement (TAVR) has revolutionized the treatment of aortic stenosis, yet the majority of TAVR devices are optimized for Caucasian and Latin American aortic root anatomies. Unfortunately, data specific to the South Asian (SA) population is limited.
Objectives
This study sought to evaluate and compare aortic root dimensions in Pakistani patients undergoing TAVR with those of other racial groups.
Methods
This study included consecutive patients undergoing TAVR workup at 2 tertiary care centers in Karachi, Pakistan. A comprehensive assessment of aortic root anatomy and dimensions was performed via cardiac computed tomography angiography. Data for 90 patients from a Japanese cohort and 181 patients from a European cohort were obtained from the published literature.
Results
In a sample of 494 patients, 58.1% (287) were male, and the mean age was 71.2 ± 9.7 years. The mean annular area was 427.33 ± 122.49 mm2, and the mean perimeter was 73.96 ± 10.17 mm. In comparison, the sinus of Valsalva (SOV) was <28 mm in 22.8% (113) versus 66.7% (60) versus 14% (17); left main height was <10.7 mm in 18.7% (90) versus 13.3% (12) versus 3.9% (7); and right coronary artery height was <12.7 mm in 14% (69) versus 7.8% (7) versus 2.2% (4) among the Pakistani, Japanese, and European cohorts, respectively.
Conclusions
The Pakistani population exhibited a higher incidence of smaller SOV dimensions compared to the European cohort and a higher incidence of shorter coronary artery heights. These findings highlight the need for tailored TAVR device designs and procedural strategies to accommodate the unique anatomical characteristics of the SA population, ensuring optimal outcomes in this demographic.
This is a visual representation of the abstract.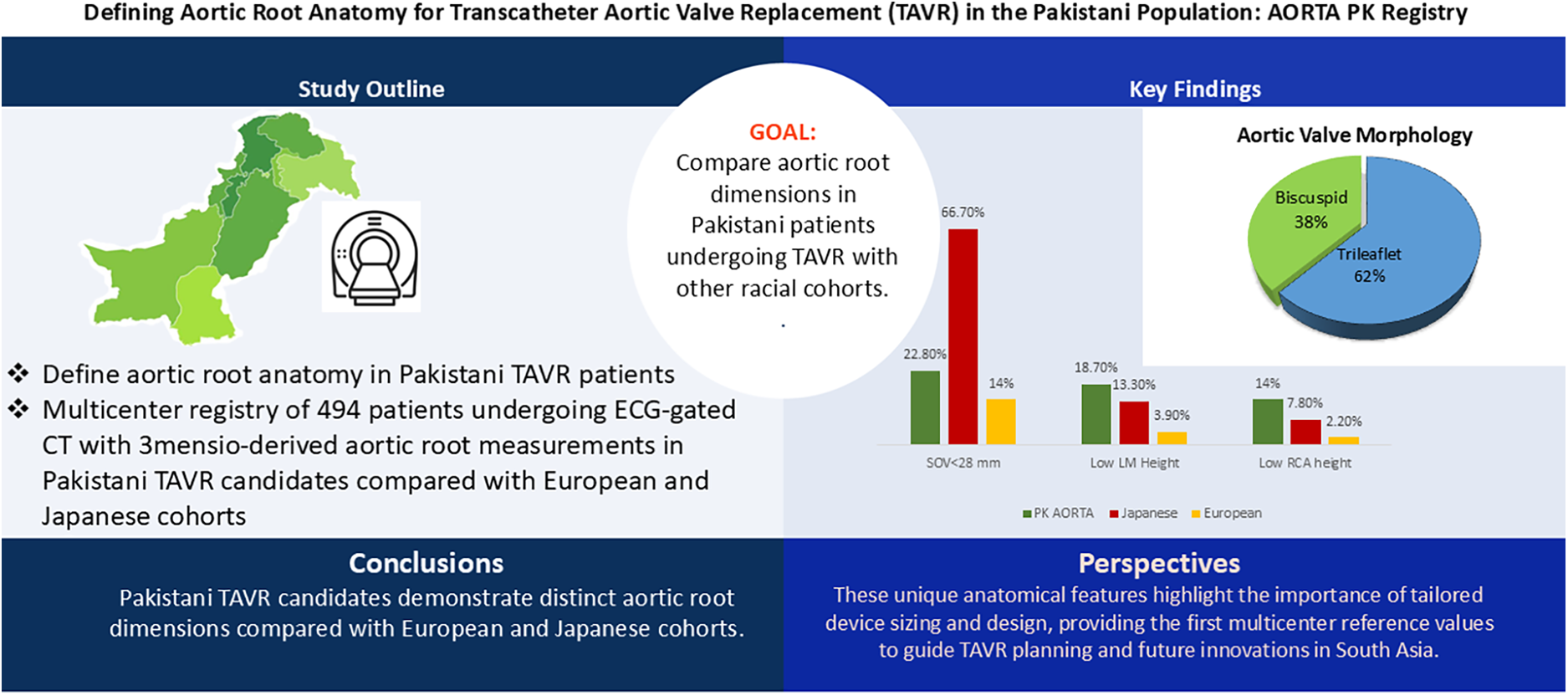
Key Points
The AORTA-PK registry provides the first multicenter computed tomography (CT)-based characterization of aortic root anatomy in Pakistani patients (South Asians) undergoing TAVR.
Pakistani patients demonstrated smaller annular and aortic root dimensions compared to European cohorts, aligning more closely with Japanese data.
Bicuspid aortic valves (BAVs) were highly prevalent (38%), with the majority being Sievers type I morphology.
These anatomical distinctions emphasize the need for tailored device designs and procedural approaches for South Asian populations.
Our findings highlight the importance of regional registries to bridge knowledge gaps and optimize TAVR outcomes globally.
Introduction
Aortic stenosis (AS) is a frequent and disabling valvular heart disease affecting mostly the elderly. Historically, surgical aortic valve replacement was the standard of care for the treatment of severe AS; however, the advent of transcatheter aortic valve replacement (TAVR) has dramatically shifted the treatment paradigm. 1 Offering a less invasive approach with fewer perioperative risks, TAVR has become a preferred option for patients at intermediate or high surgical risk, and is increasingly being used even in low-risk populations. 2 Despite its growing use worldwide, the design and optimization of TAVR devices have largely been based on data derived from Caucasian and Latin American populations.3,4 This raises concerns about the applicability of current TAVR devices in other racial groups, particularly in regions where unique anatomical variations may pose challenges to procedural success.5,6
South Asia, home to nearly a quarter of the world's population, remains underrepresented in cardiovascular research, despite the region bearing a disproportionately high burden of cardiovascular disease. 5 However, limited research has been conducted to characterize the specific anatomical features of the South Asian population, including the Pakistani population, particularly in relation to aortic root dimensions and valve morphology. This is a critical gap, as racial differences in cardiovascular anatomy, including variations in aortic root size, sinus of Valsalva (SOV) dimensions, and coronary artery height, have been demonstrated in other studies comparing East Asian and Caucasian populations. 7 These differences can significantly impact the choice of valve size, positioning, and procedural approach in TAVR, potentially influencing clinical outcomes.
Recent studies have also underscored the high prevalence of bBAVs in South Asian populations, with some reports suggesting that up to 50% of patients with AS in this region have this congenital anomaly. 8 Bicuspid valves present unique challenges in TAVR sizing, positioning, and adequate expansion due to their eccentric calcium distribution, tapered configuration of the aortovalvular complex, elliptical shape, and variable raphe morphology.9,10 This high prevalence of bicuspid valves, combined with the distinct anatomical features of South Asians (small SOV and low coronary height), highlights the urgent need for population-specific data to guide TAVR interventions in this demographic.
In light of these considerations, this study aims to comprehensively evaluate the aortic root anatomy of Pakistani patients undergoing TAVR using advanced cardiac CT imaging. By comparing aortic root dimensions between Pakistani patients and data from Japanese and European cohorts, 11 this study seeks to identify key anatomical differences that may necessitate tailored device designs and procedural techniques.
Furthermore, this research will contribute critical insights into the unique cardiovascular characteristics of the South Asian population, providing a foundational reference for future studies and clinical decision-making. By establishing a detailed anatomical profile of the Pakistani population, this study will pave the way for more informed TAVR interventions, with the ultimate goal of improving patient outcomes and advancing precision medicine in this underserved population.
Methods
This was an observational, multicenter study aimed at evaluating aortic root anatomy in Pakistani patients undergoing TAVR evaluation using cardiac CT angiography (CTA). Collaborations were established with tertiary care centers across the 2 largest TAVR centers in Pakistan, including the National Institute of Cardiovascular Diseases, Karachi, and the Aga Khan University Hospital, Karachi, to obtain CT data for patients who underwent the TAVR protocol. The study adhered to the ethical principles outlined by the Declaration of Helsinki and local institutional review boards. As the study involved retrospective analysis of anonymized CT data without direct patient contact or follow-up, informed consent was waived. Institutional review board approval was obtained. All patient data were anonymized, ensuring patient confidentiality and data privacy throughout the research process.
Patient Population
The study included consecutive patients referred for TAVR who had undergone comprehensive cardiac CTA for preprocedural evaluation. All patients underwent the standard TAVR protocol-based imaging at the collaborating centers within the 1-year study period. Patients with incomplete CT imaging, prior valve surgery, or congenital heart disease other than BAVs were excluded.
CT Data Collection and Imaging Protocols
Multidetector CTA was performed at 2 centers using contemporary high-resolution scanners. At NICVD, a Siemens SOMATOM Edge with syngo CT VB20 (128-slice) was utilized, while at AKUH, imaging was performed with a Toshiba Aquilion ONE (640-slice). Acquisition protocols were standardized across sites, with electrocardiogram (ECG)-gating and thin-slice reconstruction to optimize spatial resolution for aortic root measurements. Contrast-enhanced images were acquired following a standardized TAVR imaging protocol to ensure detailed assessment of aortic root dimensions and coronary anatomy. All imaging data were analyzed centrally using 3mensio Structural Heart software (Pie Medical Imaging, Maastricht, The Netherlands).
Because all patients were undergoing evaluation for TAVR, the CT reports generated by the Medtronic Core Lab using 3mensio served as the source for all aortic root measurements in this study. These reports were used to derive the values analyzed, ensuring a consistent methodology and minimizing variability among readers. Measurements included annular area and perimeter, SOV dimensions, sinotubular junction, left ventricular outflow tract dimensions, and coronary artery heights, all obtained in midsystole (30%–40% of the R–R interval).
Comparative data for the Japanese and European cohorts were derived from previously published studies. These studies also employed ECG-gated CTA with multiplanar reconstruction, although scanner models and postprocessing software differed and were not always explicitly specified. Direct cross-cohort comparisons should therefore be interpreted with caution, as variations in acquisition and measurement protocols may influence absolute dimensional values.
Data Collection and Analysis
Quantitative measurements included aortic annulus diameter, annular perimeter and area, SOV diameter, coronary ostium height, and the distribution of calcification. Special attention was given to the prevalence and characteristics of BAVs due to their known anatomical challenges in TAVR procedures. Data from 494 Pakistani patients were compared with data from Japanese (n = 90) and European (n = 181) cohorts, previously reported in the literature. 11
Statistical Analysis
A descriptive analysis was performed for baseline characteristics. Normality of all continuous variables was tested using the Shapiro–Wilk test and verified by visual inspection of histograms and Q–Q plots. Because most variables deviated from normality (Shapiro–Wilk p < 0.05), they are reported as median [interquartile range (IQR)] and compared using nonparametric tests (Mann–Whitney U or Kruskal–Wallis, as appropriate). In Table 3, values are presented as mean ± standard deviation (SD) for consistency with previously published European and Asian cohorts, although data were nonnormally distributed (Shapiro–Wilk p < 0.05 for most variables). Variables meeting normality assumptions are presented as mean ± SD and compared using Student's t-test/analysis of variance. Categorical variables are summarized as frequencies (%) and compared using the chi-square or Fisher's exact test. Two-tailed p < 0.05 was considered statistically significant. Shapiro–Wilk p-values for all continuous variables are provided in the Supplemental Table. To identify independent predictors of small SOV dimensions (SOV < 28 mm), we conducted a multivariable logistic regression analysis. Candidate variables were selected a priori based on clinical plausibility and included sex, body surface area (BSA), height, BAV morphology, and an elliptical index (EI) threshold of ≤0.25. A stepwise approach was avoided to minimize model overfitting; all covariates were entered simultaneously. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was defined as a two-tailed p-value <0.05. All analyses were performed using SPSS software (version 27.0).
Results
A total of 494 patients were included in the study, comprising 207 females and 287 males. Consistent with Shapiro–Wilk testing, most continuous variables were nonnormally distributed and are presented as medians [IQR] with nonparametric comparisons. The median age of the cohort was 71 years (IQR: 66–77), with no significant difference between females (71 years, IQR: 66–78) and males (72 years, IQR: 66–77; p = 0.96). Males exhibited significantly greater weight (71 kg, IQR: 60–80 vs 65 kg, IQR: 55–72; p < 0.001), height (1.68 m, IQR: 1.60–1.73 vs 1.55 m, IQR: 1.50–1.58; p < 0.001), and BSA (1.8 m², IQR: 1.6–1.94 vs 1.62 m², IQR: 1.4–1.7; p < 0.001) compared to females. In contrast, females had a higher median body mass index (BMI) (26.6, IQR: 23.4–31.0 vs 25.0, IQR: 22.0–29.0; p = 0.0025) (Table 1)
Baseline Characteristics and Root Anatomy in Patients Referred for TAVR.
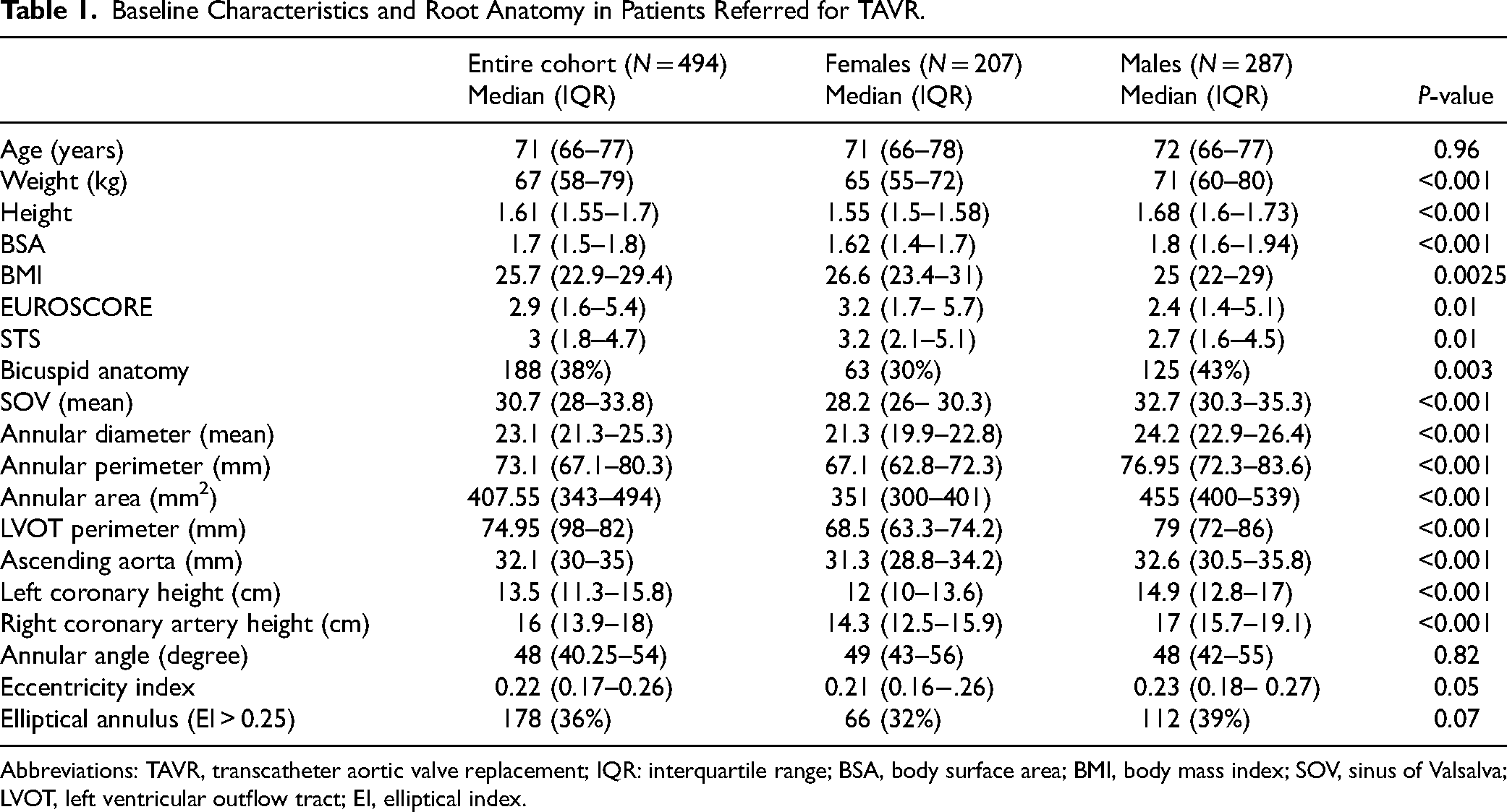
Abbreviations: TAVR, transcatheter aortic valve replacement; IQR: interquartile range; BSA, body surface area; BMI, body mass index; SOV, sinus of Valsalva; LVOT, left ventricular outflow tract; EI, elliptical index.
Risk assessment scores indicated that females had significantly higher EUROSCORE (3.2, IQR: 1.7–5.7 vs 2.4, IQR: 1.4–5.1; p = 0.01) and STS scores (3.2, IQR: 2.1–5.1 vs 2.7, IQR: 1.6–4.5; p = 0.01), reflecting a higher procedural risk profile (Table 1). Based on the heart team assessment, 65% were deemed high or prohibitive surgical risk (Figure 1).
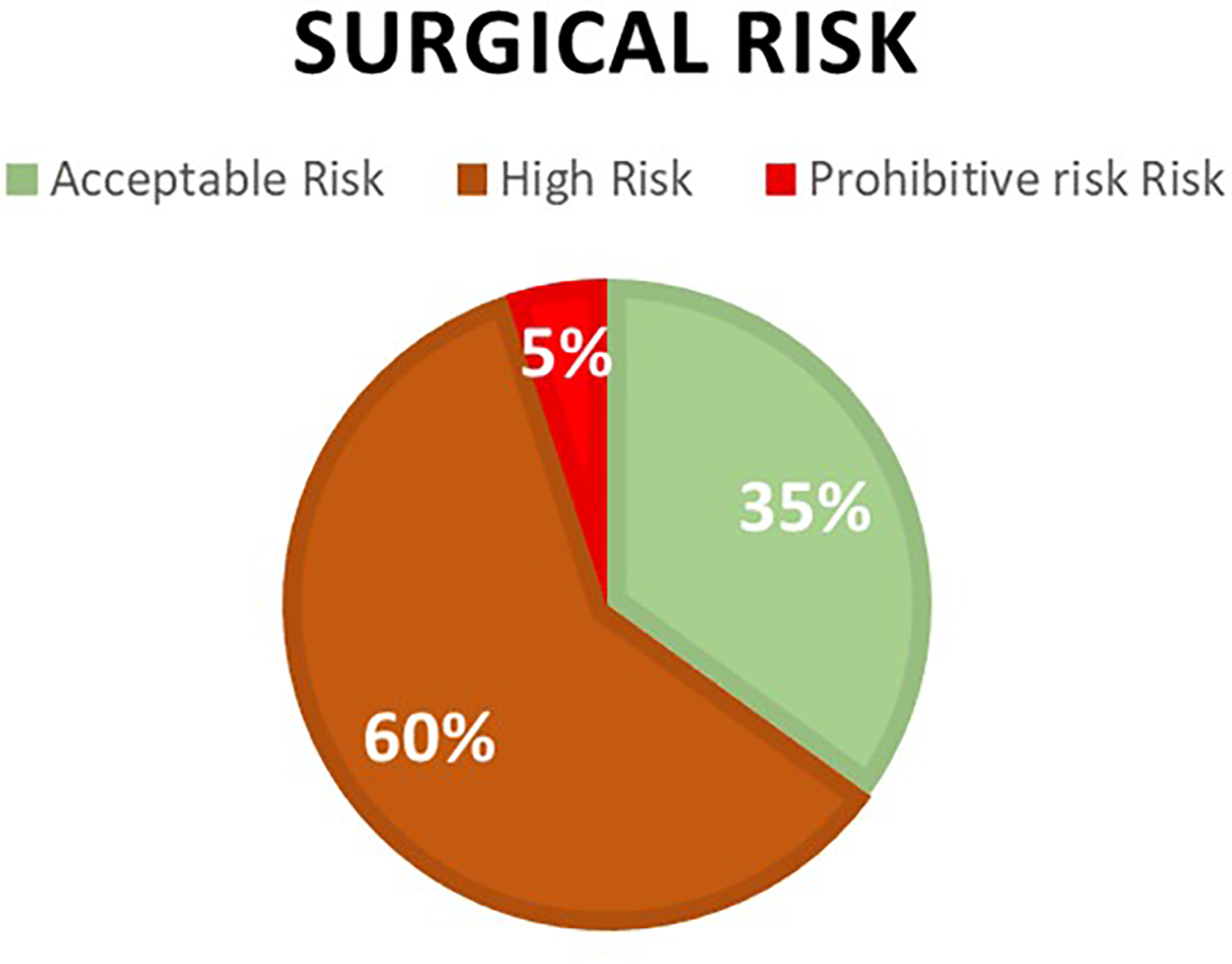
Surgical risk as assessed by the heart team.
Aortic Root Anatomy
Table 1 shows the mean aortic root dimensions stratified based on gender. Anatomical measurements revealed significant sex-based differences. Males had larger SOV diameters (32.7 mm, IQR: 30.3–35.3 vs 28.2 mm, IQR: 26.0–30.3; p < 0.001), annular diameters (24.2 mm, IQR: 22.9–26.4 vs 21.3 mm, IQR: 19.9–22.8; p < 0.001), annular perimeters (76.95 mm, IQR: 72.3–83.6 vs 67.1 mm, IQR: 62.8–72.3; p < 0.001), and annular areas (455 mm², IQR: 400–539 vs 351 mm², IQR: 300–401; p < 0.001). Similarly, left coronary height (14.9 mm, IQR: 12.8–17.0 vs 12.0 mm, IQR: 10.0–13.6; p < 0.001) and right coronary height (17.0 mm, IQR: 15.7–19.1 vs 14.3 mm, IQR: 12.5–15.9; p < 0.001) were greater in males. Ascending aorta diameters were also larger in males (32.6 mm, IQR: 30.5–35.8 vs 31.3 mm, IQR: 28.8–34.2; p < 0.001) (Figure 2).
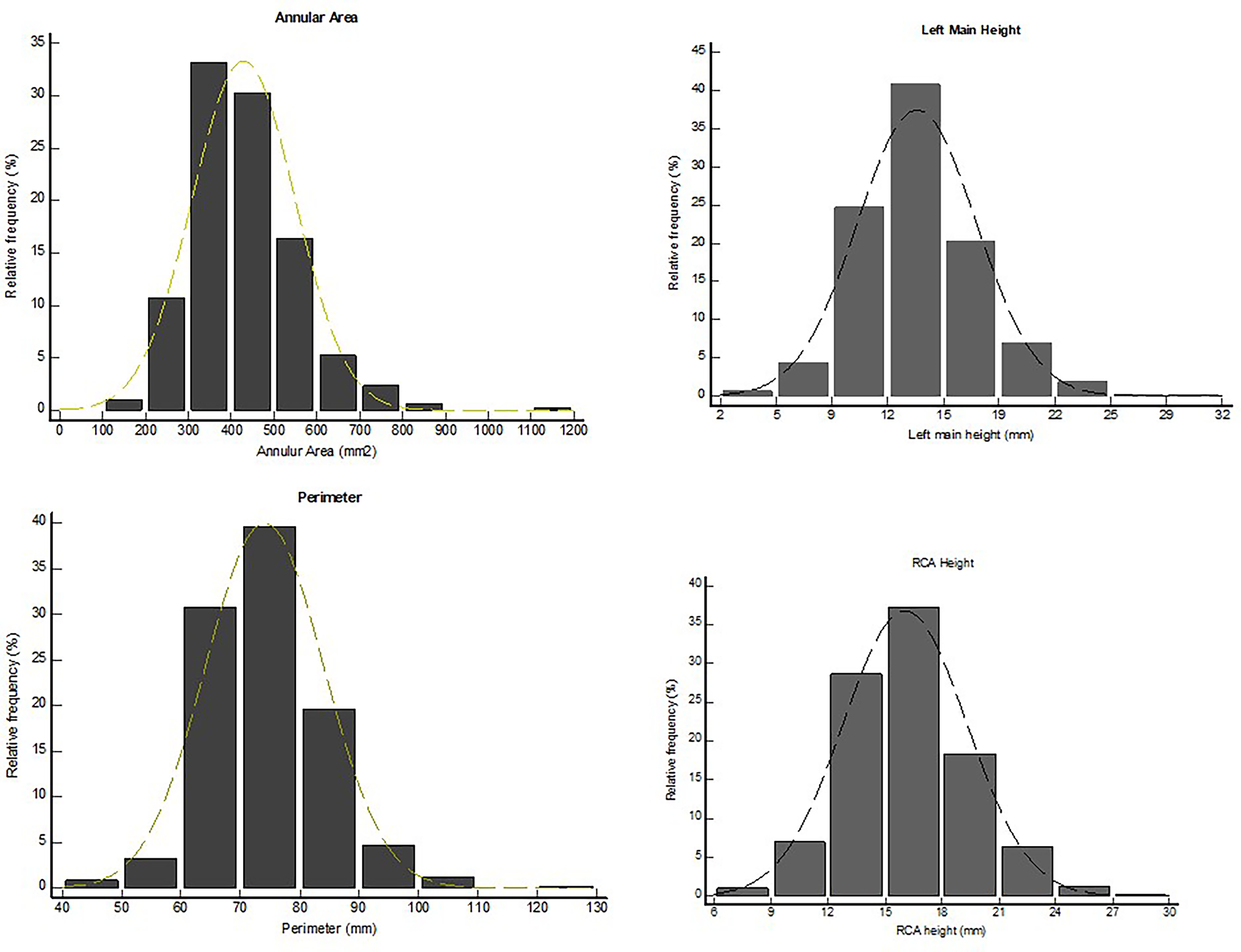
Distribution of annular perimeter, area, and coronary heights.
Bicuspid anatomy was more frequently observed in males (43% vs 30%; p = 0.003). The eccentricity index (1 – short annulus diameter/long annulus diameter) × 100, according to the method previously described by Blanke et al 12 was slightly higher in males (0.23, IQR: 0.18–0.27 vs 0.21, IQR: 0.16–0.26; p = 0.05). Although a higher proportion of males had elliptical annuli (EI > 0.25: 39% vs 32%), this difference did not reach statistical significance (p = 0.07).
On multivariable logistic regression analysis, female sex was the strongest independent predictor of a small SOV (OR 6.01, 95% CI 3.74–9.66, p < 0.0001). In contrast, bicuspid valve morphology was associated with significantly lower odds of a small SOV (OR 0.40, 95% CI 0.23–0.69, p = 0.0011). An EI >0.25 was also independently predictive of small SOV (OR 1.82, 95% CI 1.12–2.95, p = 0.015). Neither BSA nor height was significantly associated with SOV size in the adjusted model (p > 0.70 for both).
Bicuspid Anatomy
Figure 3 shows the distribution of bicuspid valves, with 39% patients having bicuspid morphology. In total, 141 patients (75%) had Sievers type I, 36 (19%) patients had type 0, and 8 patients (6%) had type II bicuspid valves. Patients with BAVs were younger (70 vs 74 years, p < 0.0001) and exhibited larger annular dimensions, including diameter (24.2 vs 22.7 mm, p < 0.001), area (451 vs 388 mm², p < 0.0001), and perimeter (77 vs 71.2 mm, p < 0.0001), as well as larger SOV diameters (32 vs 30 mm, p < 0.0001). While BMI was lower (24 vs 26, p = 0.02), BSA was marginally higher (1.75 vs 1.70 m², p = 0.05). These findings underscore key anatomical and demographic differences between valve phenotypes (Table 2).
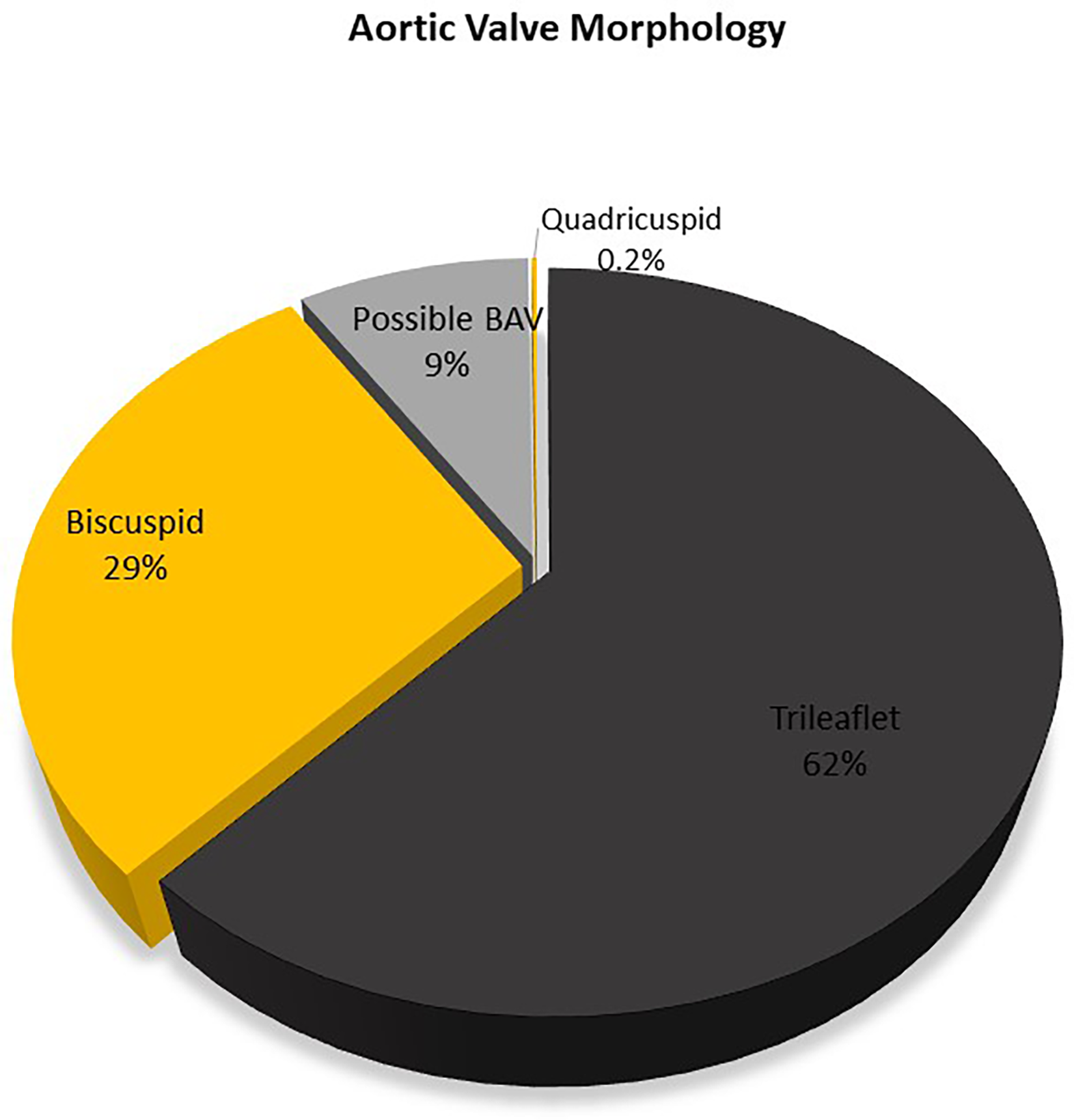
Distribution of valve phenotypes.
Differences Between Bicuspid and Tricuspid Aortic Valves.
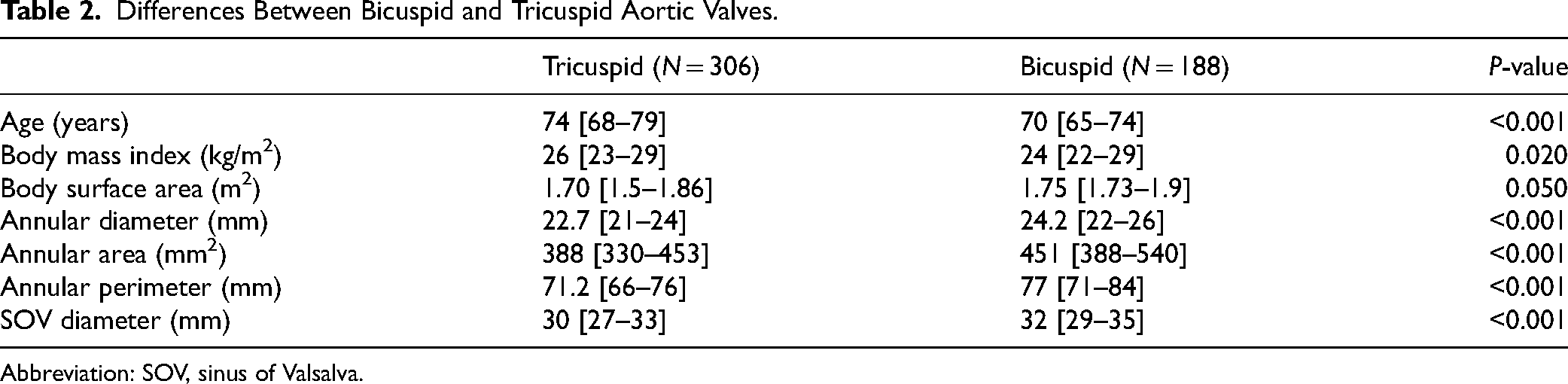
Abbreviation: SOV, sinus of Valsalva.
Comparative Anatomy to European and Japanese Cohorts
The Pakistani cohort demonstrated distinct anatomical features compared to Japanese and European cohorts. A smaller SOV (SOV < 28 mm) was more prevalent in Japanese patients (66.7%) than in Pakistanis (22.8%) or Europeans (14.0%). Similarly, a lower SOV-to-calculated average annulus diameter (CAAD) ratio (<1.26) was most common in Japanese patients (47.8%), followed by Europeans (33.6%) and Pakistanis (25.5%). The prevalence of lower left main coronary arteries (left main height [LM] < 10.7 mm) was highest in Pakistanis (18.7%) compared to Japanese (13.3%) and Europeans (3.9%). Additionally, lower right coronary artery height (RCA < 12.7 mm) was more frequent in the Pakistani cohort (14.0%) than in Japanese (7.8%) or European cohorts (2.2%) (Table 3).
Comparison with Japanese and European Cohorts. 11
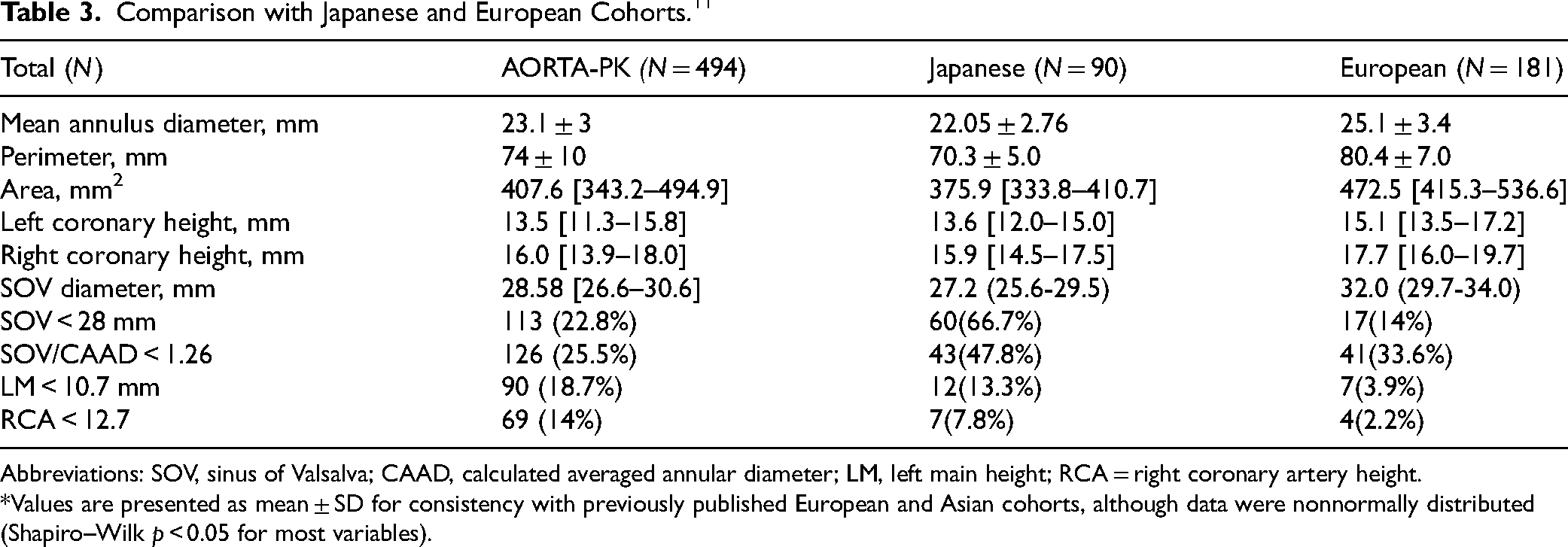
Abbreviations: SOV, sinus of Valsalva; CAAD, calculated averaged annular diameter; LM, left main height; RCA = right coronary artery height.
*Values are presented as mean ± SD for consistency with previously published European and Asian cohorts, although data were nonnormally distributed (Shapiro–Wilk p < 0.05 for most variables).
Discussion
This study provides a comprehensive analysis of the aortic root anatomy of the Pakistani population undergoing TAVR, addressing a critical gap in cardiovascular research within this demographic. By systematically comparing aortic root dimensions between Pakistani, Japanese, and European cohorts, the study highlights key anatomical differences underscoring the need for tailored approaches in TAVR to accommodate population-specific anatomical variations (central illustration).
A significant proportion of the Pakistani cohort demonstrated smaller SOV dimensions compared to the European population, with 22.8% of Pakistani patients exhibiting SOV <28 mm versus 14% in the European cohort. These findings align with prior studies highlighting racial variations in cardiovascular anatomy, where East Asian populations similarly present with smaller SOV dimensions. 5 Smaller SOV dimensions pose challenges during valve deployment, including an increased risk of coronary obstruction, paravalvular leak (PVL), and annular disruption. 13 Furthermore, smaller dimensions limit future valve-in-valve procedures, which is relevant in the lifetime management of younger patients with AS. 14
The Pakistani cohort exhibited lower coronary artery heights compared to both Japanese and European cohorts. Specifically, a left main coronary artery height <10.7 mm was observed in 18.7% of Pakistani patients, compared to 13.3% in the Japanese cohort and 3.9% in the European cohort. Similarly, the prevalence of RCA <12.7 mm was higher in the Pakistani cohort (14%) than in the Japanese (7.8%) and European cohorts (2.2%). 15 Lower coronary heights, particularly in combination with smaller SOV, significantly increase the risk of coronary obstruction during TAVR, necessitating meticulous preprocedural planning. Detailed and meticulous analysis of CTA plays a pivotal role in identifying at-risk patients and guiding procedural modifications such as transcatheter aortic valve implantation (TAVI) prosthesis sizing, depth of deployment, coronary protection with stents, or intentional leaflet laceration using the BASILICA procedure, which is very challenging in high-risk native valve procedures. 16
Several types of TAVR valves are available in Asia. The balloon-expandable Edwards Sapien (Edwards Lifesciences) family of valves is among the first valves introduced and widely used in the region. Other commonly used valves include the Medtronic self-expanding prostheses (CoreValve and Evolut series). Their usage varies across different countries in Asia. 5 Until recently, the Asian market predominantly utilized self-expanding valves for TAVR, whose supra-annular design complicated coronary access in patients with low coronary ostia. In China, three locally manufactured TAVR devices are available and approved: the Venus-A valve (Venus MedTech), J-Valve (Jie Cheng Medical Technologies), and MicroPort VitaFlow valve (MicroPort Medical). 16 In India, 2 types of valves are currently manufactured: MyVal (a balloon-expandable system from Meril Life Sciences Pvt Ltd) and Hydra (a self-expanding system from Vascular Innovations Co Ltd). Their use is approved; however, data to validate their success needs to be strengthened. 17
The rates of complications, such as PVL, permanent pacemaker implantation, major vascular complications, and the need for open-heart surgery, in Asian registries (OCEAN-TAVI registry and Asia-TAVI registry) were similar to those reported in Western registries. However, there is a plausible difference in the TAVR recipient population between the 2, which may be attributed to the high dropout rate from TAVR in Asian countries due to complex anatomical features, high costs, and low reimbursement rates.7,18–20
BAV morphology was significantly more prevalent in the Pakistani cohort (38%) compared to global registries such as the OCEAN-TAVI (2.7%), Asian-TAVR (5.8%), and TVT (3%–3.5%) registries. 21 Prior studies have shown that BAV is particularly common in East Asian populations, with prevalence rates approaching 50% in Chinese patients undergoing TAVR for severe AS. 22 The prevalence observed in our study aligns with these findings, reinforcing the unique anatomical challenges posed by BAV in non-Caucasian populations.
Bicuspid valves present unique challenges in TAVR sizing, positioning, and adequate expansion due to their eccentric calcium distribution, tapered configuration of the aortovalvular complex, elliptical shape, and variable raphe morphology. These factors contribute to a higher risk of PVL, prosthesis under expansion, and second valve implantation.9,10 Tailored procedural strategies and device designs are critical to addressing these challenges, particularly in populations with a high prevalence of BAV, such as the Pakistani cohort.
The anatomical variations identified in this study have critical implications for the safe and effective implementation of TAVR in the Pakistani population. Smaller SOV dimensions and lower coronary artery heights necessitate meticulous preprocedural planning, enhanced imaging techniques, and potentially novel device designs. The introduction of MyVal provides a promising alternative for patients with challenging anatomy, while procedural adaptations to reduce coronary obstruction can mitigate the dreaded complication of left coronary obstruction in high-risk cases. 15
The high prevalence of BAV in the Pakistani population underscores the importance of population-specific data to optimize device selection and procedural techniques. Device manufacturers must consider these anatomical differences to improve outcomes and minimize complications in this underrepresented demographic. 23
Study Limitations
This study is limited by its observational design and the reliance on published literature for Japanese and European cohort data, which may introduce selection bias. Additionally, the single-region Pakistani sample may not fully represent the broader South Asian population. Future multicenter studies with larger sample sizes are needed to validate these findings and investigate the impact of anatomical differences on clinical outcomes. 7 Additionally, cross-cohort comparisons should be interpreted with caution, as the Japanese and European data were derived from published studies that used in-house core lab analyses using 3mensio, whereas our Pakistani cohort relied on CT reports generated by the Medtronic Core Lab using 3mensio to ensure measurement consistency.
This study provides critical insights into the unique anatomical characteristics of the Pakistani population undergoing TAVR, highlighting significant differences compared to Japanese and European cohorts. These findings underscore the necessity for population-specific considerations in TAVR planning and device design to optimize patient outcomes. Future research should focus on developing tailored strategies to accommodate these anatomical variations and improve the safety and efficacy of TAVR in diverse populations.
Conclusion
Aortic root dimensions in Pakistani patients undergoing TAVR were systematically evaluated, revealing distinct anatomical differences compared to Japanese and European cohorts. Notably, the Pakistani population exhibited a higher incidence of smaller SOV dimensions compared to the European cohort, and a higher incidence of shorter coronary artery heights. These findings highlight the need for tailored TAVR device designs and procedural strategies to accommodate the unique anatomical characteristics of the South Asian population, ensuring optimal outcomes in this demographic.
Clinical Perspectives
Anatomic variations in the Pakistani population, including smaller annulus sizes, low coronary heights, and a high prevalence of BAV, highlight the need for tailored TAVR strategies.
Supplemental Material
sj-docx-1-hvs-10.1177_30494826251386377 - Supplemental material for Defining Aortic Root Anatomy for Transcatheter Aortic Valve Replacement (TAVR) in the Pakistani Population: Insights From Multicenter Computed Tomography (CT) Evaluation Aortic Root Assessment and Oriented Reference for TAVR in Pakistan (AORTA-PK Registry)
Supplemental material, sj-docx-1-hvs-10.1177_30494826251386377 for Defining Aortic Root Anatomy for Transcatheter Aortic Valve Replacement (TAVR) in the Pakistani Population: Insights From Multicenter Computed Tomography (CT) Evaluation Aortic Root Assessment and Oriented Reference for TAVR in Pakistan (AORTA-PK Registry) by Abdul Hakeem, Osman Faheem, Farhan Memon, Jehangir Ali Shah, Ahsan Ali Lakho, Asim Ali, Navaira Azeem, Manjeet Singh, Bashir Hanif, Asad Pathan, Sabha Bhatti and Tahir Saghir in Journal of the Heart Valve Society
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.