
Abstract
Valvular heart diseases (VHDs) pose significant challenges to cardiovascular health globally, contributing substantially to morbidity and mortality. Despite advancements in therapeutic strategies, women frequently face delayed diagnoses, surgical referrals, and encounter poorer postoperative results compared to men. This inequity stems from historical biases where women were underrepresented in pivotal studies shaping current medical guidelines. However, emergent research focuses more frequently on women, highlighting remarkably sex-differences in VHD etiology, diagnosis, and treatment. Acknowledging and addressing these differences is required for fair healthcare and optimized clinical outcomes for both sexes in the current era. Hence, this review proposes to highlight the implications of sex-differences concerning diagnosis, treatment modalities, and outcomes among patients affected by VHDs.
This is a visual representation of the abstract.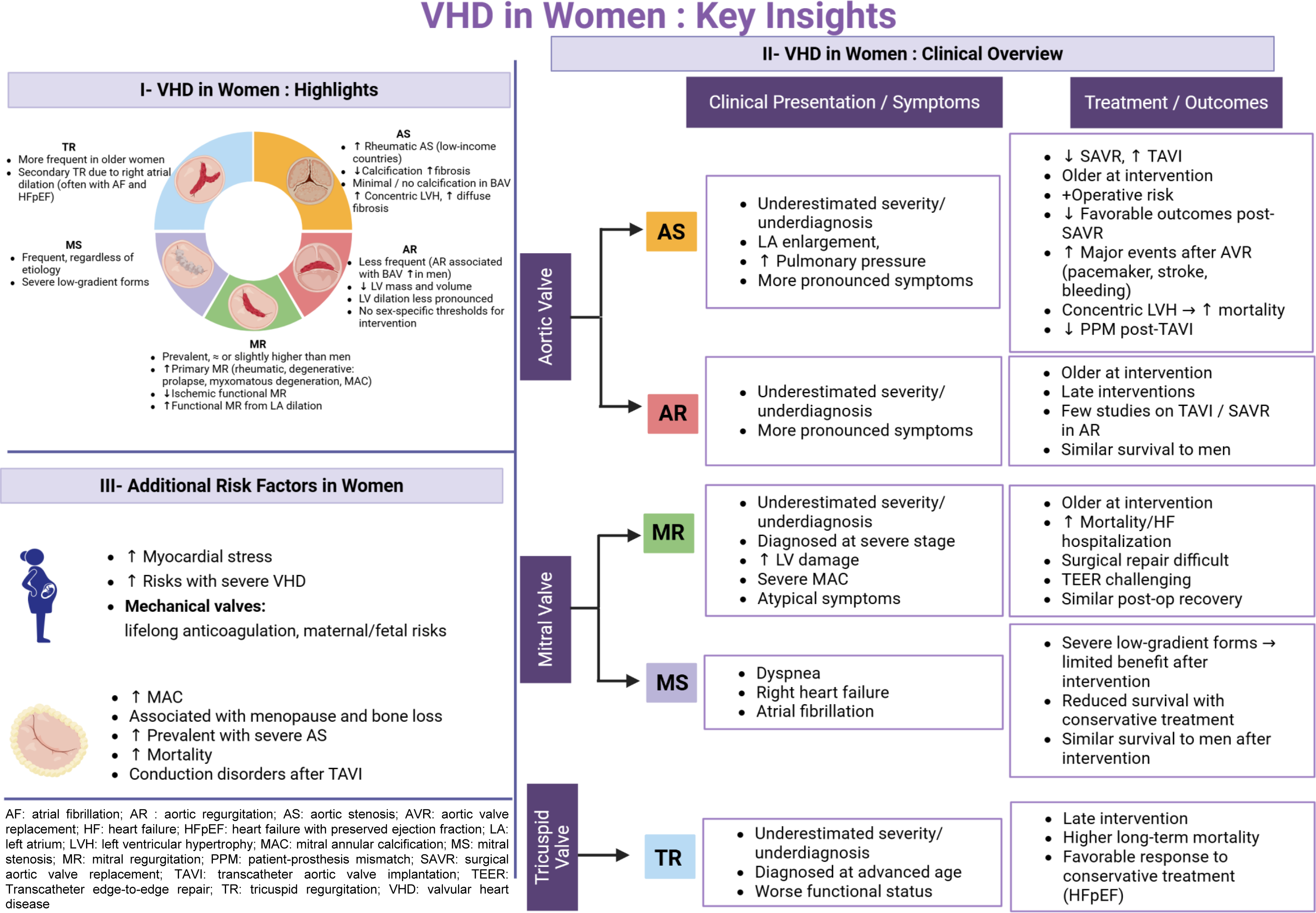
Key Points
Women with valvular heart disease present with distinct etiologies, anatomical features, and remodeling patterns that shape diagnosis, treatment, and outcomes.
Underrecognition of disease severity and reliance on non–sex-specific thresholds may contribute to delayed referrals in women.
Sex-specific left-ventricular remodeling influences intervention strategy and long-term prognosis.
Adequate female representation in clinical trials is critical to develop evidence-based, sex-tailored management.
Introduction
Valvular heart diseases (VHDs) represent a significant burden on global cardiovascular health, leading worldwide to morbidity and mortality. 1 While rheumatic valve diseases remain prevalent in low-income regions, degenerative and functional diseases represent the cornerstone of VHDs etiology in high-income countries. 2
Current therapeutic strategies, which have seen significant advancements, primarily rely on surgical or transcatheter interventions for the severe VHDs forms, given the lack of pharmacologic treatments demonstrating efficacy in arresting valvular disease progression in different clinical scenarios. 3
The majority (70%) of VHDs diagnoses in high-income countries occur in individual aged 65 years or older, excluding pulmonary valve disease. Overall, 47% of VHDs are diagnosed in women, however the prevalence of tricuspid regurgitation (TR) and mitral stenosis (MS) is reported higher in women than in men, suggesting interesting specific sex-differences in the VHDs epidemiology.4–6 Moving from epidemiological scenarios, an underrepresentation of women is present in many trials which constitute the landmark of the current guidelines, potentially neglecting sex-specific features in VHDs management. 7
An emergent growing body of research underscores notable sex-differences in VHDs not only in epidemiology, but also in pathophysiology, presentation, intervention referral practices, treatment modalities, and clinical outcomes. 8
In this review, we sought to spotlight the current knowledge linked to sex-differences in the clinical presentation, management strategies, and therapeutic responses concerning the prevalent degenerative or functional VHDs among adults, encompassing aortic stenosis (AS), chronic aortic regurgitation (AR), mitral regurgitation (MR) and TR.
Aortic stenosis
Epidemiology
AS is the most prevalent VHD with clinical significance and the third most prevalent heart disease after coronary artery disease (CAD) and systemic arterial hypertension. The prevalence of AS increases with age, as it is present in 5% of the population aged ≥ 65 years old and in up to 12.4% of adults aged ≥ 75 years old. 9
In younger adults, calcific AS is mostly present in patients with bicuspid aortic valves (BAV), which affects 0.5% to 2% of the population in a 1:3 male to female ratio (Figure 1).10,11 Hence, AS is most prevalent in men than in women in younger patients (ie, below 60 years of age), but this tendency shifts in elderly populations with similar prevalence between men and women. 6
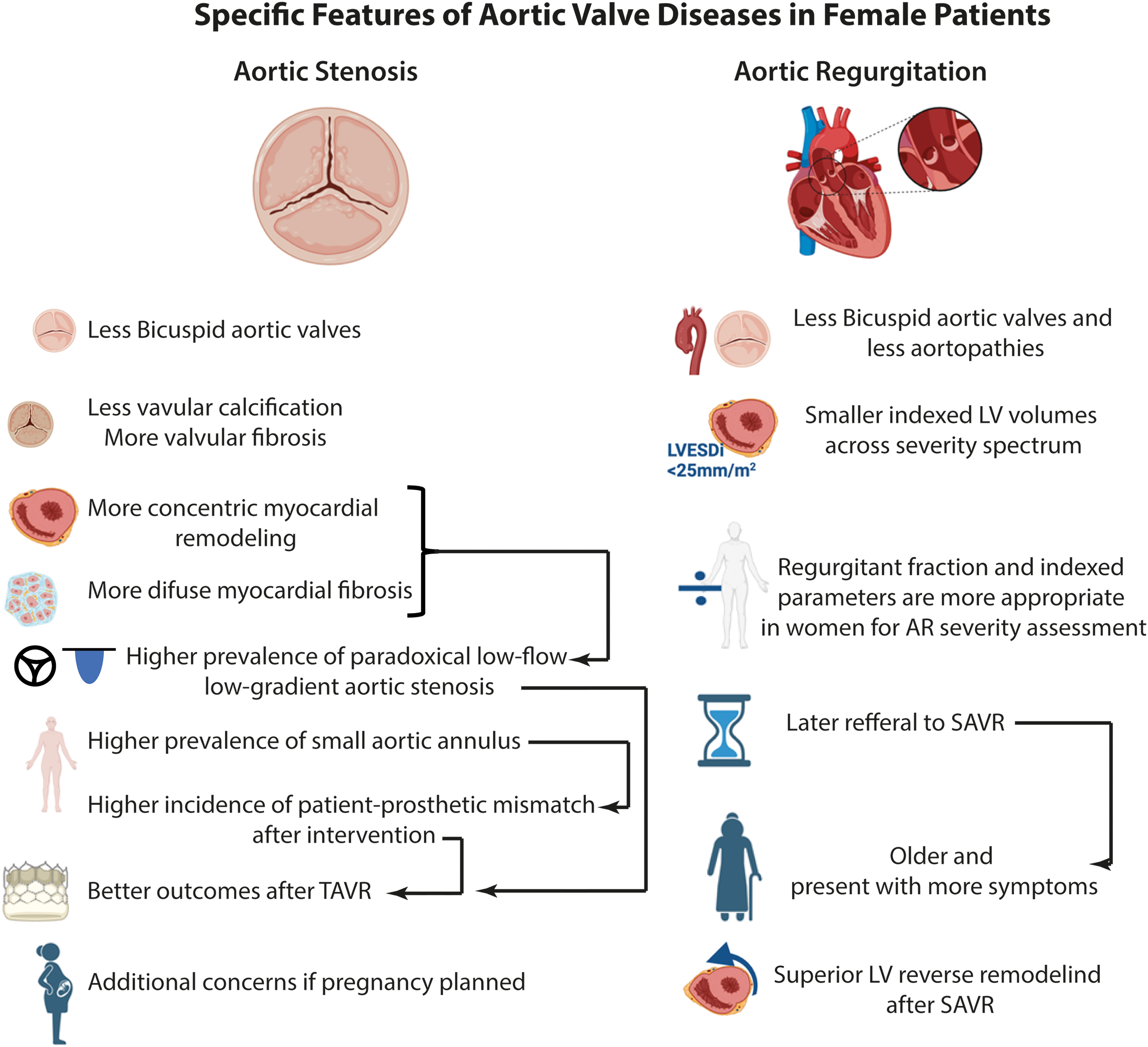
Specific Features in Aortic Valve Diseases in Female Patients.
Mechanisms and Etiologies
Rheumatic AS remains prevalent in low-income countries, and rheumatic AS is more prevalent in women, such as all rheumatic valve diseases. In high-income countries, the vast majority of encountered AS is associated to “degenerative” processes. However, the term degenerative is misleading given the very active nature of the disease. Indeed, the pathophysiology of calcific AS is characterized by lipid deposition, chronic oxidation and inflammation as well as the transition of the valvular interstitial cells to an osteoblastic phenotype, which induce fibrosis and calcium deposition and thus leaflet thickening. 12 The resulting fibrocalcific remodeling leads to stiffening of the valve leaflets and narrowing of the valve opening, and subsequent cardiac outflow obstruction. It is well documented that for a given hemodynamic severity, women consistently present with less valvular calcification than men, but with higher levels of fibrotic and dense connective tissue within valve leaflets (Figure 1).13,14
Compensatory responses to the chronic pressure overload imposed on the left ventricle (LV) also differ between sexes. Indeed, women most frequently display concentric hypertrophy or normal LV geometry, while eccentric and concentric hypertrophy are the most prevalent remodeling patterns in men. 15 As the LV hypertrophies, myocyte apoptosis occurs as a result of the mismatch between myocardial oxygen supply and demands. Degree of nonischemic replacement myocardial fibrosis assessed with late gadolinium enhancement on cardiac magnetic resonance (CMR) is similar in men and women, but women exhibit a significantly larger extent of diffuse myocardial fibrosis regardless of AS severity (Figure 1). 16 The use of CMR in selected asymptomatic patients with severe AS may still hold great promise for optimizing the timing of aortic valve replacement (AVR) through the early detection of myocardial fibrosis and subtle ventricular decompensation.16,17 Although the EVOLVED trial did not demonstrate a benefit of early AVR guided by CMR findings in a broad population, 18 future studies may better define specific subgroups—such as younger patients, those with rapid disease progression, or those with extensive mid-wall fibrosis—who could benefit from a CMR-guided strategy.
Diagnosis
Gold-standard for assessing AS severity is transthoracic echocardiography (TTE). Values of aortic valve area (AVA) < 1.0 cm2, mean gradient >>40 mm Hg and peak aortic jet velocity >>4 m/s are diagnostic for severe AS. When echocardiographic parameters are discordant (ie, low gradient/velocity and tight AVA), which occurs in up to 40% of AS patients, dobutamine stress echocardiography can be performed to increase flow rate, and distinguish true severe from pseudo severe AS-especially in patients with low LV ejection fraction (LVEF)-, but a large proportion of patients exhibit lack of contractile reserve leading to inconclusive results.19–21 In that case, the measurement of aortic valve calcification by computed tomography (CT) imaging is useful as it is a powerful predictor of clinical outcomes.22,23
Findings in AS are not solely restrained to the valve itself. The chronic hemodynamic burden eventually leads to myocardial adaptations, mainly LV hypertrophy to compensate for the increased wall stress and maintain LV function. In women, concentric hypertrophy is the most frequent remodeling pattern, which explains why they more often exhibit paradoxical low-flow low-gradient (LFLG) patterns (ie, low flow despite a preserved LVEF) (Figure 1). This particularity certainly accounts for the underdiagnosis of severe AS in women and their lower rates of AVR referral as their LVEF remains higher than the guideline-Class I ESC/AHA 50% threshold. 24 There is consequently systematic overestimation of their LV systolic function despite significantly decreased stroke volume index. Notably, a Class IIa indication for AVR in asymptomatic patients with severe AS and LVEF below 55% is currently reported in ESC guidelines, since those values are associated with higher mortality in both men and women. 25 The measurement of global longitudinal strain (GLS) could also be of incremental value in this subset of patients for assessing LV systolic function as it is more sensitive and reproducible than LVEF.26,27,28
In patients with LFLG AS with discordant echocardiographic parameters and either preserved or reduced LVEF, aortic valve calcium (AVC) scoring by CT imaging can be very useful to assess true severity of the disease. Sex-specific thresholds of 1200 or 1300 AU in women and 2000 AU in men indicating severe AS are well established and account for the higher calcific burden in men for a given hemodynamic severity regardless of age or valve phenotype.14,23,29,30 AVC density thresholds (AVC indexed to the cross-sectional area of the aortic annulus) have also been validated and can be used for enhanced accuracy in patients presenting annulus sizes which diverge from the sex-specific average. Rounded threshold values of 300 AU/cm2 in women and 500 AU/cm2 indicate severe disease but are not currently included in current American or European guidelines.23,31
However, caution is required when interpreting AVC scores as women may present with mostly fibrotic remodeling and low calcific burden, especially in young female patients, bicuspid patients and patients with cardiac amyloidosis, who can sometimes even exhibit no calcification at all but severe hemodynamic parameters. A novel method not yet established in routine clinical setting allows for the assessment of valvular noncalcified tissue in the valvular leaflets. Assessment of aortic valve noncalcified over calcified tissue ratio measured by contrast-enhanced CT may be preferable to noncontrast CT when noncalcific tissue accounts for most of the burden causing outflow obstruction (ie, fibrosis, cardiac amyloidosis). Indeed, noncalcified/calcified tissue ratio demonstrates a better correlation with peak aortic jet velocity, especially in female patients and can improve identification of severe AS, but future studies are warranted to establish severity thresholds.32,33
The prevalent pattern of LFLG AS in women combined with preserved LVEF and lower calcific burden might explain the association of female sex and lower rates of diagnostic testing and specialist visits compared to men. 34 Greater clinical recognition of paradoxical LFLG AS is warranted to avoid underdiagnosing and undertreating women. Hence, thresholds of reduced LVEF should be increased and the echocardiographic assessment should focus additionally on myocardial deformation parameters, such as GLS 35 and peak atrial longitudinal strain 36 recently identified as promising tools potentially aiming to guide optimal AVR timing. However, despite a complete myocardial deformation assessment has been recently introduced in a staging system framework in AS, 37 sex-specific data are currently lacking.
Treatment
The natural history of AS can be divided into 2 phases; the first one being the clinically silent progression of the valve disease over many years, during which myocardial adaptations occur as a result of the chronic afterload enforced on the left ventricle. The second phase is characterized by the onset of symptoms, classically dyspnea, angina, and syncope. Once these symptoms occur, the prognosis is poor, with an expected survival of 2 to 3 years if no intervention is performed. 38 Treatment options consist of AVR either surgically (SAVR) of by percutaneous access (TAVR), as no pharmacological treatment has been proven to be effective in treating or halting progression of AS. Formal indications of intervention include severe symptomatic disease or asymptomatic severe disease with LVEF below 50% or if another cardiac surgery is planned (Class I).24,25
At time of AVR referral, female patients are consistently older, exhibit higher left atrial volumes and pulmonary pressures than men, and present with more symptoms. However, for the same AS severity, AVR is less likely to be performed on women compared to men, even after age matching. 39 This may be partially explained by men being more likely to require concomitant cardiac surgery (ie, coronary artery bypass graft [CABG], aorta repair, or replacement). Prior to intervention, men have more cardiovascular comorbidities than women, with higher prevalence of diabetes, previous myocardial infarction and percutaneous coronary intervention, CABG surgery, peripheral artery disease and low LVEF. 39
The literature is clear on the fact that male patients have a better prognosis after SAVR than their female counterparts.40,41 Indeed, men often exhibit AS characteristics more favorable for SAVR, such as bicuspid aortic valves, lower prevalence of small aortic annuli (SAA) and higher levels of valvular calcific tissue (Figure 1). While this greater calcium burden may contribute to better outcomes after SAVR by facilitating complete excision of the diseased valve, it is also a strong predictor of significant paravalvular leak after TAVR with both self-expandable and balloon-expandable valves. 42
On the other hand, women frequently exhibit AS patterns associated with worse outcomes after SAVR, such as LFLG AS with preserved LVEF. 43 The less invasive nature of TAVR can therefore benefit female patients given their worse preoperative profile and older age, in addition to their often-impaired diastolic function and reduced stroke volume index, which puts them at an increased operative risk.44–48,49–52 Conversely, mortality as well as rates of permanent pacemaker implantation, stroke and bleeding are higher in female patients undergoing SAVR compared with their male counterparts, especially in the early postoperative period. 53 Nevertheless, there remains inconsistencies in the literature as several studies comparing SAVR outcomes in women and men report similar baseline-matched long-term survival.54–56
Interestingly, it has been shown that concentric hypertrophy is associated with a high risk (60%) of all-cause mortality or cardiovascular mortality in women both before and after AVR, independent of intervention strategy, while this association is not found in male patients. 57 Consistent with these results, residual LV hypertrophy post-AVR has been associated with significantly worse outcomes in women compared to men. 58
Many female patients, especially elder women exhibit SAA, which presents an additional challenge in the treatment of AS and is associated with worse postoperative outcomes. According to recent studies, TAVR seems to associate with superior hemodynamic results and lower rates of prosthesis patient mismatch (PPM) in these patients. 59 PPM is a major operative concern in patients with SAA as it is linked to lower LV mass regression, compromised normalization of coronary flow reserve, suboptimal LV function after AVR, and is a powerful predictor of long-term mortality as well as structural valve deterioration.60,61 Results from the PARTNER trial also exhibit lower 2-year mortality in SAA patients who underwent TAVR versus SAVR. 62 However, the VIVA trial revealed conflicting results with previous studies. Indeed, in this cohort of patients with SAA, which included more than 90% of women, TAVR was not superior to SAVR regarding hemodynamic or clinical outcomes, and there were no significant differences in severe PPM rates between the 2 treatments. 63 Hence, further studies, with larger cohorts are warranted to either corroborate or invalidate these novel findings.
A particular concern must be addressed in women of childbearing age who require AVR (Figure 1). Usually, mechanical prosthesis is preferred in young patients given the increased durability of the device compared to biological prostheses, which have a life expectancy of about 10 to 15 years. However, the choice of a mechanical valve requires long-term anticoagulation, which is possible in pregnancy by opting for a low molecular weight heparin, but not ideal. Indeed, it is less effective than warfarin in preventing thrombotic events, but the latter is associated with high pregnancy loss and fetal complications. 64 Hence, no anticoagulation strategy is truly safe for both mother and fetus, which is why mechanical valves should be avoided in women who are planning pregnancy. An especially attractive option in this subset of patients is the Ross procedure, which consists of replacing the diseased aortic valve with the patient's own pulmonary valve followed by the placement of a homograft in the pulmonary position. 65 Freedom of reoperation for aortic valve at 15 years is also much higher (90.0% vs 57.1%) with the Ross procedure than with a bioprosthesis. 66 At 25 years the freedom from reintervention remains high with 70.5% for the autograft and 74.3% for the right ventricular outflow tract. 67 However, this procedure is technically challenging, and its outcomes are highly contingent upon hospital surgical volumes and cardiac surgeon expertise. 68 Lastly, the nature of the procedure involves the inherent risk of converting a single-valve disease into a double-valve disease.
Considering the interaction of multiple individual baseline characteristics in female patients presenting with severe AS, it should be highlighted that decisions regarding intervention type for treating AS require careful discussion by a specialized heart team, as there is no “one treatment fits all.” Surely, high-risk elder women and female patients with paradoxical LFLG benefit the most from TAVR, but the option of SAVR must not be denied to female patients in low/moderate-risk patients presenting with favorable anatomic and hemodynamic characteristics for surgical approach solely based on sex.
Aortic Regurgitation
Chronic AR has a prevalence of 4.9%, and more than mild AR is found in 0.5% of the population. 69 Rheumatic disease remains the main etiology of AR in low-income countries, but the vast majority of AR in high-income countries is due to either congenital or degenerative diseases. Hence, prevalence of the disease increases with older age and other comorbidities as well as cardiac diseases are frequently encountered. AR is a frequent finding in patients with aortopathies, endocarditis and in patients with BAV as they often display larger diameters of aortic root and ascending aorta compared to their tricuspid counterparts. These characteristics, more prevalent in men than in women explain the predominance of AR in men across the age spectrum (Figure 1). 7 It should be noted that among BAV patients, men are more likely to develop complications such as moderate to severe AR and aortopathies, while women more frequently develop moderate to severe AS. 70
AR is characterized by reflux of blood from the aorta into the LV during diastole resulting in decreased effective stroke volume. The evolution of the disease is usually slowly progressive due to chronic LV volume overload, which leads to subsequent myocardial dilatation and eccentric hypertrophy, showing concomitant diastolic dysfunction in later phases of the disease. Women tend to display lower LV volumes and mass across AR severity, even when accounting for body surface area (BSA). However, this difference lessens in BAV patients with at least moderate AR with similar end-systolic diameters indexed to BSA between men and women. 71 Interestingly, women also frequently exhibit normal LV size despite severe AR, which may contribute to severity underestimation given the absence of LV dilatation. 72 Furthermore, studies show that TTE underestimates LV dilatation particularly in women and that CMR could be adopted for LV myocardial characterization in this context to avoid delaying surgical referral. 73
Assessment of AR severity is performed by TTE, during which LV size and systolic function are also measured. Doppler jet width ≥65% of LV outflow tract, vena contracta superior to 0.6 cm, regurgitant volume ≥60 mL/beat, regurgitant fraction ≥50% and effective regurgitant orifice area ≥0.3 cm2 indicate severe disease.24,25 Evidence of LV dilatation is also required in diagnosing AR, which is considered mild to moderate when LV end systolic volume is <50 mm and severe when LV end systolic volume is >>50 or if its indexed value to BSA is of >>25 mm/m2.24,25 This latter indexed value is particularly useful in female patients given they rarely meet the absolute threshold of 50 mm. However, other parameters of severity such as vena contracta and regurgitant volumes may underestimate AR severity in female patients because of their consistently smaller LV. Regurgitant fraction and indexed parameters can thus be more diagnostically accurate in women. However, the 25 mm/m2 threshold might be too high as several studies have shown a threshold closer to 20 mm/m2 might be more appropriate (Figure 1).74–77
Women are less likely than men to undergo aortic valve surgery and at time of surgery, women are older and present with more advanced symptoms (Figure 1). 78 Nonetheless, long-term survival after aortic valve surgery is similar between sexes and female patients exhibit even superior LV reverse remodeling than men. Hence, the survival disadvantage of women with AR is a result of late diagnosis and referral rather than female sex per se.
Class I indications of aortic valve surgery include severe symptomatic AR without regard to LV function, asymptomatic severe AR and LV systolic dysfunction/dilatation (LVEF 55% or lower), and severe AR in patients already undergoing cardiac surgery for other indications. 24
Although current guidelines for AR recommend uniform LV dimension thresholds for intervention irrespective of sex, recent data demonstrate important sex-specific differences. In a cohort of 525 patients with severe AR, women consistently exhibited smaller LV volumes than men, both at baseline and during follow-up, yet experienced adverse events at substantially lower LV end-systolic volume indexed to BSA (LVESVi) thresholds (27 mL/m² in women vs 50 mL/m² in men). 79 These findings indicate that guideline-based cutoffs may underestimate risk in women, supporting the need for sex-specific considerations in AR management.
In patients at prohibitive surgical risk with severe AR and symptoms and/or LV systolic dysfunction, medical therapy with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers are recommended. 24 In contrast with AS management where patients receiving TAVR have exceeded the number of patients undergoing SAVR in recent years, aortic valve surgery remains the mainstay of treatment for chronic severe AR. 80 Recently, TAVR has been demonstrated effective and safe in a prospective multicentric study involving patients with severe AR at 1-year follow-up. This pivotal finding highlights the need for randomized controlled trials to explore the role of TAVR in severe AR. 81 Currently, TAVR is considered off-label only in patients with severe pure AR in carefully selected scenarios and prohibitive surgical risk, since AR most frequently presents with anatomical features not suited for TAVR, including aortic annulus and aortic root dilatation. 82
Mitral Valve Disease
Mitral valve disease (MVD) is one of the most common forms of VHD associated with significant cardiovascular morbidity and mortality, and its incidence increases with age.1,83–85
Nonrheumatic degenerative mitral valve heart diseases showed a prevalence of approximately 16,000,000 in 2022, accounting for roughly 38,000 deaths worldwide. 86
Rheumatic MVD remains a major global health burden, with over 40 million cases likely in 2021, based on rheumatic heart disease estimates. It disproportionately affects younger populations in low-sociodemographic index regions, especially sub-Saharan Africa, with age-standardized prevalence over 1100 per 100,000. 87 While disability-adjusted life years have declined since 1990, the rising prevalence underscores ongoing disparities in prevention and care. 87
MVD encompasses MR and MS, including also overlapping between MR and MS. 88 Furthermore, the presence of mitral annular calcification (MAC) is of utmost importance, since distinct sex-specific feature are observed in this condition.
Mitral Regurgitation
Epidemiology and physiopathology
MR is the second most common VHD after AS in high-income countries (31.5 vs 43.1%) 84 and is defined as retrograde flow from the LV to the left atrium during systole 89 : this occurs when there is inadequate coaptation of the mitral valve leaflets during systole and a change in the pressure gradient between the atrium and ventricle. 90 Trivial MR is common in the general population, with a prevalence of 40%. However, significant MR is associated with increased mortality, regardless of LV function and associated comorbidities, impacting over 24 million people worldwide and resulting in over 34,000 deaths in 2019. Moderate or severe MR increases with age and affects 9.3% of the population over 75 years of age. In the United States, there were more than 2 to 2.5 million affected patients in 2000, with the prevalence of MR increasing at a rate of 0.7% in patients aged 18 to 44 years and 13.3% in patients over 75 years. This burden is expected to grow in the next years due to the progressive ageing of the population.83,86,88,91,92–95 It is either equally common in both men and women, or slightly more common in women. Regarding pathophysiology, MR is classified in 2 categories24,25,90,96 with different underlying mechanisms: primary and secondary MR.
Primary MR, also referred to as organic or degenerative MR, occurs when there is a structural abnormality of the mitral leaflets or subvalvular apparatus, ie, chordae tendineae or papillary muscles. This phenotype is the most common form of MR in the United States. 97 It encompasses a series of alterations: acquired or congenital tissue changes, infiltrative or dysplastic, leading to elongation or rupture of the cords resulting in leaflet prolapse or flail, as well as mitral annular dilatation. 98 Approximately 2% of the general population is affected, with 5% to 6% of prevalence in women. Although more common in women, evidence of severe regurgitation associated with organic MR is more frequent in men.99–101
While the prevalence of rheumatic diseases has declined in high-income countries, they remain a common cause of MR—especially in women—characterized by calcific deposits, fibrous thickening of the leaflets, fibrosis of the papillary muscles, and asymmetric annular dilatation.85,98,102,103 Furthermore, MAC is another organic mechanism involved in MR, prevalent among individuals over the age of 60 (Figure 2). The pathogenesis is not well understood but may be attributed to mechanical stress on the annulus. In this situation, concomitant calcific AS may be present. MAC can cause leaflet deformation and chordal elongation, leading to regurgitation as a result of leaflet displacement or immobilization, which hinders correct valvular coaptation.104–106
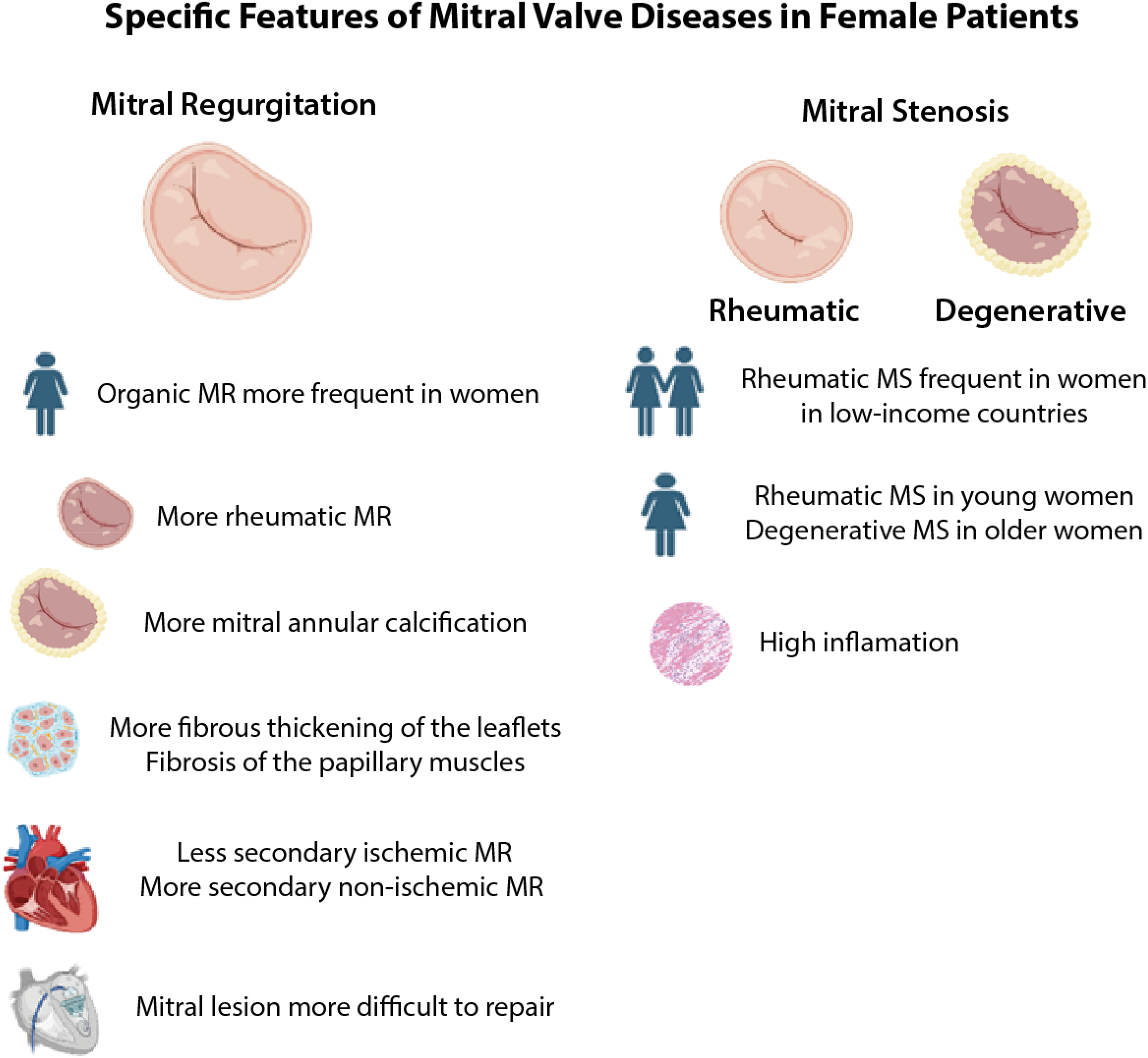
Specific Features in Mitral Valve Disease in Females Patients.
In general, women with organic MR tend to have a higher prevalence of rheumatic MR, more severe MAC, fewer leaflet flails, and an increased frequency of bileaflet or anterior prolapse as well as generalized myxomatous degeneration (Figure 2).100,101,107–110
Secondary MR, also called functional MR, it is primarily the result of primary LV pathology which induces remodeling and dysfunction in an anatomically normal valve, more specifically, an altered geometry of the LV causing dilatation of the mitral valve annulus resulting in incomplete systolic leaflet coaptation, or left atrial anomaly89,93,110,111
The most common cause of functional MR is ischemic dilatation of the LV and/or ischemic fibrosis of the papillary muscle. 112 Ischemic lesions induce negative and progressive LV remodeling. Initially, the MR associated with this etiology is frequently moderate, 113 and it occurs in 20% to 50% of patients early after acute myocardial infarction. Moderate ischemic MR may progress to severe MR over time and after 30-days from acute myocardial infarction 12% of patients exhibit more than moderate MR. The prevalence rises up to 20% in patients with concomitant heart failure and previous myocardial infarction.113–115 Other studies have estimated that up to 40% of patients with heart failure due to dilated cardiomyopathy develop functional MR.89,116
LV remodeling due to acute coronary syndromes and ischemic heart disease, leading functional MR, is more common in men than in women (Figure 2). In contrast, functional MR due to left atrial dilatation is more frequent in women.117,118
Secondary MR may occur in a nonischemic context when dilation and LV remodeling are not associated with CAD but linked to other abnormalities such as dilated cardiomyopathies. In this scenario, potential mechanisms involved in the development of MR include a decrease in transmural pressure gradient, geometric changes in the mitral annulus, papillary muscles, and mitral valve, and dyssynchronous LV contractions.89,116
Clinical profile and diagnosis
In primary MR, the course of the disease can extend over several years, and many patients remain asymptomatic even with severe MR due to compensatory pathophysiological mechanisms. Indeed, to normalize wall stress, the myocardium may undergo hypertrophy, dilation and increased end-diastolic volume, leading to a reduction in left ventricular contractility and ejection fraction. This dysfunction may be irreversible. Progressive dilation of the left atrium may also occur to maintain normal atrial pressure, followed by an increase in atrial and LV diastolic pressures, as well as pulmonary vascular resistance, leading to clinical decompensation and symptoms of heart failure.119–122 Symptoms of heart failure may also manifest in patients with preserved LV function who exhibit elevated pulmonary venous pressure or develop atrial fibrillation122,123
Women are less frequently diagnosed with severe MR and a dilated LV regardless of their symptomatic status, and they are often referred for cardiac surgery later, probably due to underestimation of MR severity.101,124,125 In addition, the thresholds proposed to assess MR severity are not indexed to body surface area, nor sex-specific.24,25 Males are more likely to be referred for surgery at the appropriate time due to the presence of more typical cardiac symptoms, with more LV dysfunction.110,126,127 Although women referred for surgery tend to present higher age, a poor preoperative profile, and severe MAC, they derive the same benefit in terms of cardiac remodeling as men after intervention.101,124
Interestingly, in a study of primary MR excluding functional causes, women had similar indexed left atrial (LA) size but lower reservoir strain and higher stiffness, with a 4-fold higher risk of elevated stiffness. Findings highlight sex-specific LA remodeling and support using LA strain and stiffness, beyond size alone, when assessing MR in both sexes. 128
Treatment and outcomes
Surgical repair is preferred whenever possible in cases of severe organic MR, while surgical replacement is performed in cases where repair is not feasible. Percutaneous procedures are also offered to patients at high surgical risk. Women have lesions that are more difficult to repair, such as rheumatic MR, anterior prolapse and biliary leaflets, consequently women have a lower surgical repair rate (Figure 2). However, when analyzed by etiology, both the mitral valve repair rate and the recurrence rate of MR after repair are similar between men and women.100,101,108,129 Female sex is associated with adverse outcomes, including operative mortality, long-term mortality, and hospitalization for heart failure.100,101,110,125
Transcatheter edge-to-edge repair (TEER) is an effective, less invasive treatment for both primary and secondary MR in patients at high surgical risk. 130 In functional MR, TEER is associated with favorable outcomes. However, TEER cannot be performed in the presence of increased MAC or small LV dimensions, which are very common in women. 131 Before TEER, women are generally older than men but have fewer comorbidities, and postprocedural outcomes are similar between the sexes. Left atrial hypertrophy, which is more frequent in men, is an independent predictor of adverse long-term outcomes after transcatheter mitral valve repair132,133
Results from the randomized EVEREST II trial comparing surgery with MitraClip showed that percutaneous intervention was less effective in reducing regurgitation at 1 year but improved left ventricular dimensions and NYHA class. At 4-year follow-up, there were no significant differences in surgical reintervention or the prevalence of moderate-to-severe MR between treatment groups.134,135
Mitral Stenosis
MS could be caused by rheumatic heart disease and characterized by commissural fusion that directly causes stenosis, 136 or by exuberant MAC and valvular calcification, 137 both being more prevalent in women (Figure 2). Narrowing of the valve orifice can result in increased left atrial pressure, increased pulmonary venous pressure, exertional dyspnea, right heart failure, and the onset of atrial fibrillation.88,138 The majority of patients with rheumatic MS are young and predominantly female, with an increased inflammatory process,139–141 while patients with degenerative MS are older but still predominantly female 137 (Figure 2).
MS severity is graded by integrating mitral valve area (MVA) and transmitral mean pressure gradient (MPG) with clinical context.25,142 Direct planimetry is the reference, with MVA ≤1.5 cm² indicating clinically relevant MS. Pressure half-time (PHT)-derived MVA ≤1.5 cm² supports clinically relevant stenosis but may be inaccurate in altered compliance or postvalvotomy states. Severe MS typically presents with MPG ≥10 mm Hg at normal heart rates, though gradient is influenced by flow conditions. 142 Stress echocardiography can uncover exercise-induced MPG ≥15 mm Hg or pulmonary artery systolic pressure >>60 mm Hg, refining severity assessment and timing of intervention. 142
Previous research has specifically examined low-gradient severe rheumatic MS, characterized by discordant echocardiographic markers of severity. 143 This phenotype, more commonly observed in women, is associated with limited clinical benefit from mitral valvuloplasty. Contributing factors include intrinsic MS combined with ventricular–vascular uncoupling, reduced left ventricular compliance, and a high prevalence of atrial fibrillation. 143
Treatment of MS includes procedures such as balloon valvuloplasty, commissurotomy, or valve replacement if the patient's clinical condition worsens and symptoms develop. 88
Mitral Annular Calcification
MAC is more common and often more severe in women, as shown across multiple studies and ethnic groups.137,144 Women exhibit greater calcium burden and calcification activity, potentially driven by mechanisms beyond atherosclerosis, such as inflammation, biomechanical stress, and altered calcium handling. 144 Postmenopausal bone loss and reduced bone mineral density, especially prevalent in women, have been linked to MAC development. Hemodynamic factors like increased afterload and smaller left ventricles may further predispose women. Female patients show more frequent MR, higher transmitral gradients, and greater concentric remodeling. 145 Risk profiles also differ by sex; hypertension and hypertrophic cardiomyopathy are independent predictors of severe MAC only in women. 146
In a retrospective study of 287 patients with severe calcific MS due to MAC, women represented the majority (66%) and had worse survival than men when managed conservatively. However, among those undergoing mitral valve intervention, outcomes were comparable between sexes. These findings, confirmed by propensity score matching, highlight the prognostic impact of sex in treatment strategies for calcific MS. 147
However, some longitudinal data suggest female sex alone does not predict MAC progression leaving this field not fully clarified. 148
In the setting of multiple VHDs, recent studies have highlighted the frequent coexistence of MAC and AS, with MAC present in up to 50% of patients with severe AS. This “duo” is associated with poorer long-term outcomes. 149 In such cases, SAVR has been shown to confer better survival than TAVR, even after specific adjustment for confounding factors. 149
TR in Women
Epidemiology, Classification and Pathophysiology
TR represents a VHD recently gaining interest as a burdensome health problem independently linked to morbidity and mortality. 150 Significantly sex-differences in TR epidemiology have been highlighted, with an overall prevalence of moderate-to-severe forms around 4% in patients aged 75 years of older (0.55% overall), mostly encountered in women (approximately 60% of cases).92,151,152 Sex specific differences have been previously demonstrated at the time of diagnosis, suggesting that women are diagnosed with severe TR at later age, compared to men. 94
The most recent TR classification accounts on its etiology and mechanism, proposing 3 different groups: (1) primary TR, a rare entity determined by a primitive lesion of the tricuspid valve (congenital—ie, Ebstein`s anomaly, tricuspid dysplasia, or acquired—ie, myxomatous degeneration, carcinoid syndrome); (2) secondary TR, the most common form with normal valve apparatus but inadequate coaptation between the tricuspid leaflet, driven and sustained by secondary causes involving the right or left heart morphology and/or function; and (3) Cardiac Implantable Electronic Device Lead-Induced TR, due to leads interference with the tricuspid valvular-apparatus. 153 Although the atrial (A-STR) and ventricular (V-STR) forms of secondary TR are distinctively described and account for approximately 80% of cases, there must be recognized some overlap. Notably, the long-standing presence of significant isolated A-STR could lead to a right-sided volume overload which may induce right ventricular dilation and dysfunction, making not always clear the real distinction between A-STR and V-STR. 153 Whether it is well established that V-STR carries worse prognosis than A-STR, the recent focus of research shifted towards the pathophysiology and progression of A-STR which seemed to be linked to important sex-differences.154,155 A-STR is diagnosed commonly in elderly women, with long-standing atrial fibrillation or coexisting heart failure with preserved ejection fraction (HFpEF)155,156 (Figure 3). The underlying pathophysiological mechanism is related to the dilation of the tricuspid anulus imposed by the right atrial enlargement, accompanied by a lack of adaptative growth of tricuspid valve leaflets. 155 Separately from an etiological classification, some studies proposed a stratification of TR guided by the clinical context.151,152 TR is rarely isolated and often is diagnosed with associated left-sided VHDs or LV disfunction, presenting frequently concomitant sign of pulmonary hypertension. 151 The clinical-context presents important sex-differences in presentation, revealing how the combination of TR and concomitant LV dysfunction is a peculiar scenario where women are interestingly less involved. 157
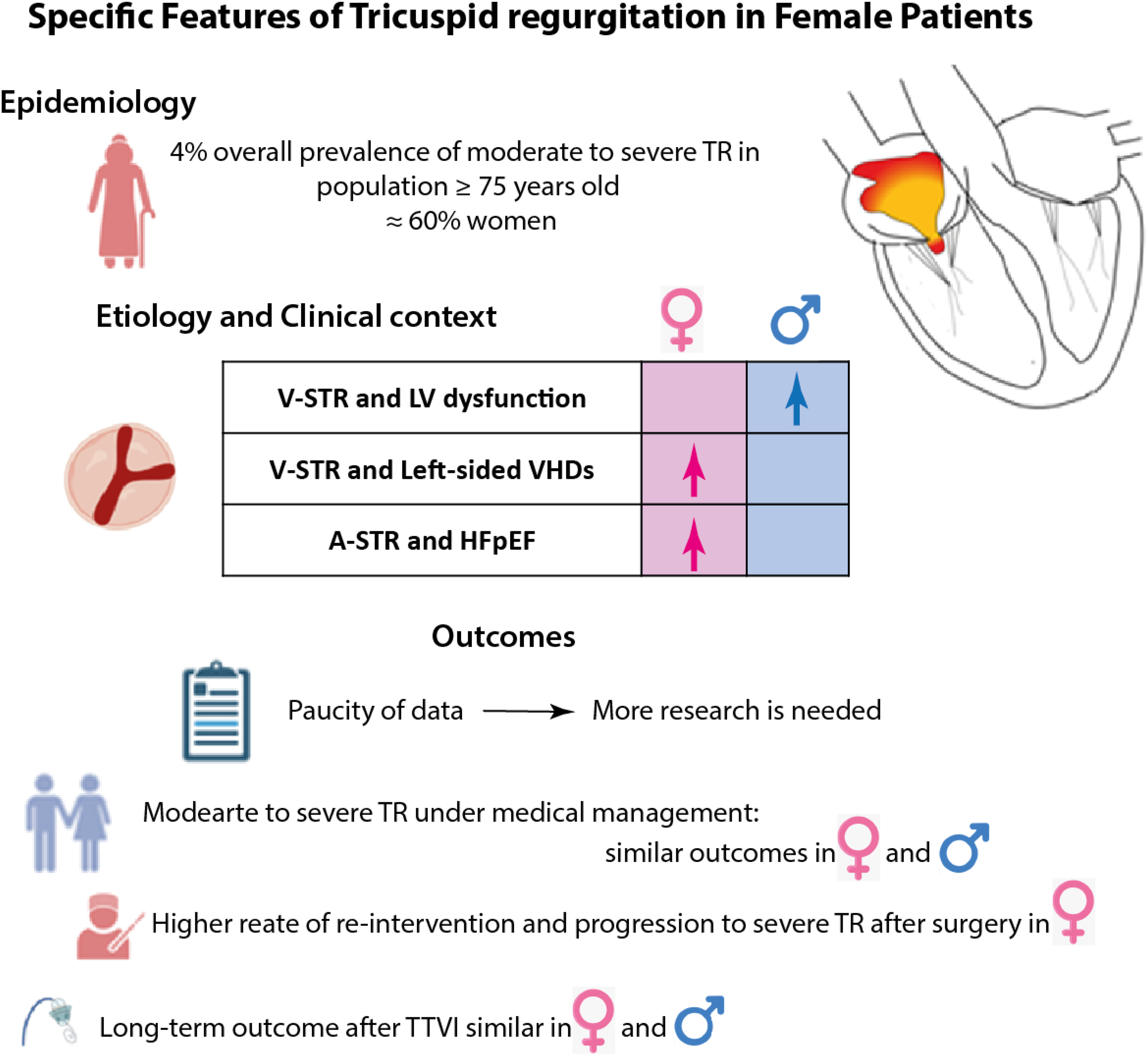
Specific Features in Tricuspid Regurgitation in Females Patients.
The impact of sex in the prognosis of TR still represents a novel field of research, with available paucity of evidence. A study by Dietz et al 158 in a large cohort of 1569 patients with significant TR (only 5% primary TR) found that sex did not present independent association on long-term mortality, after covariate-balance with propensity score matching (Figure 3). This study cohort was represented mostly by patients with significant TR followed under medical management (only 13% underwent tricuspid valve surgery during the follow-up).
Tricuspid Valve Intervention Strategies
Medical therapy represents the pivotal cornerstone in the context of TR, leading to the optimization of the volemic state (diuretics) and to manage the underlying conditions responsible of TR worsening (ie, antiremodeling therapy in the presence of heart failure, antiarrhythmic drugs for rhythm control). 24 Interesting sex-differences were found in the medical treatment response in patients with HFpEF potentially influencing A-STR management: women may respond more favorably to mineralocorticoid receptor antagonists and receptor-neprilisyn inhibitors.159–161
The current 2020 AHA/ESC guidelines report one unique Class I indication for tricuspid valve surgery established severe TR in the context of concomitant left-sided valve surgery. 24 Notably, the presence of signs or symptoms of heart failure in conjunction with severe TR, as well as progressive right ventricular dysfunction in asymptomatic severe primitive TR, are classified as Class II indications for isolated tricuspid valve surgery (IIa and IIb respectively). 24 Consequently, numerous patients with severe TR are treated at advanced stages of the disease, prompting intensified research into early intervention strategies. 162 In the current landscape, notable technological advancement in transcatheter-tricuspid valve intervention (TTVI) has positioned TTVI as a viable option for severe symptomatic TR, but the optimal timing for early-treatment remains unexplored.163,164 Significant sex-disparities are reported in literature in the outcome of patients undergoing mitral valve surgery and concomitant TR. Previous studies reported that women tend to develop severe TR with higher reoperation rates than men after mitral valve surgery.165–167,168
Furthermore, significant racial/ethnic and sex disparities exist in tricuspid valve surgery utilization in the United States, with lower rates among Black, Hispanic, and female patients. Women had lower odds of acute kidney injury but higher odds of blood transfusion. In-hospital mortality and major complications were similar across all groups. Further research is needed to address these disparities. 169
Finally, recent research focused specifically on sex-difference in patients undergoing TTVI.
Women with TR often present for transcatheter intervention at more advanced stages, with worse functional status and comorbidities. 170 Although procedural outcomes are similar, 171 men may derive greater quality-of-life improvements. 172 These patterns suggest later referral in women, potentially due to slower disease progression, underrecognition of symptoms, or differing clinical thresholds. 173
A multicentric study by Fortmeier et al 171 enrolling 702 patients undergoing TTVI found no difference of 2-years overall mortality between sexes, however were reported different prognostically sex-specific threshold of tricuspid annulus plane systolic excursion and mean pulmonary pressure ratio (TAPSE/mPAP). A higher TAPSE/mPAP threshold in women has been identified, potentially suggesting that women could present better right ventricular systolic performance relative to pulmonary artery pressure levels than men. 171 The tendency of women to present higher right ventricular systolic reserve was also reported by a study involving patients with significant TR, where men reported lower right longitudinal function parameters for the same TR degree severity. 174 Nevertheless, these findings seem not to translate in outcome sex-differences after TTVI accordingly to current studies.171,175
Clinical Implication
Sex differences in TR are present in epidemiology, etiology and treatment-outcome link (Figure 3). Evidence supporting prompt referral for early surgery or transcatheter options is growing in order to improve the outcome, especially for moderate to severe TR. Despite surgery being long-time the gold standard of TR interventions, transcatheter approaches offer nowadays promising alternative. However, sex-disparities persist in treatment rates, delays, redo-interventions, and outcomes. Standardized care and risk assessment could improve treatment selection, particularly for women, reducing disparities. More research is required to assess the best treatment option (surgical vs transcatheter) accounting for sex-differences.
Conclusions
Sex-specific differences are prevalent across VHDs, impacting diagnosis, referral for treatment, treatment selection, and outcomes. Women often experience underestimation of VHD severity and delayed treatment referral due to insufficient sex-specific or indexed parameters for severity assessment and surgical triggers.110,176 Additionally, symptoms in women tend to be less pronounced, further complicating accurate evaluation. These sex-specific features also influence postintervention outcomes. Addressing these gaps of knowledge is crucial for improving women's valvular heart health, necessitating prompt referral and tailored intervention choices without delay when required. 177
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: P.S. holds a research grant from University of Verona (Verona, Italy). MA.C. holds the Canada Research Chair on Women Valve and Heart Health from the Canadian Institutes of Health Research (Ottawa, Canada), Institute of Circulatory and Respiratory Health (Grant No. CRC-2024-00315).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MA.C. received funding from Edwards Lifesciences for CT core laboratory analyses and Research grant from Medtronic, Edwards Lifesciences, Novartis, Rednvia, Novartis, and Pi-Cardia with no direct personal compensation and unrelated to the present work.