
Abstract
Current guidelines for surgical intervention in severe aortic regurgitation may be too conservative, potentially missing the window for optimal outcomes. This editorial highlight growing evidence suggesting that earlier surgical intervention—particularly in patients with LVEF between 50—55%—may prevent adverse events such as cardiogenic shock, even in patients with preserved systolic function. Chronic LV volume overload can mask early dysfunction, delaying critical treatment. The authors advocate for refined risk stratification using advanced imaging and biomarkers, and call for a prospective randomized trial to establish updated, evidence—based surgical thresholds.
This is a visual representation of the abstract.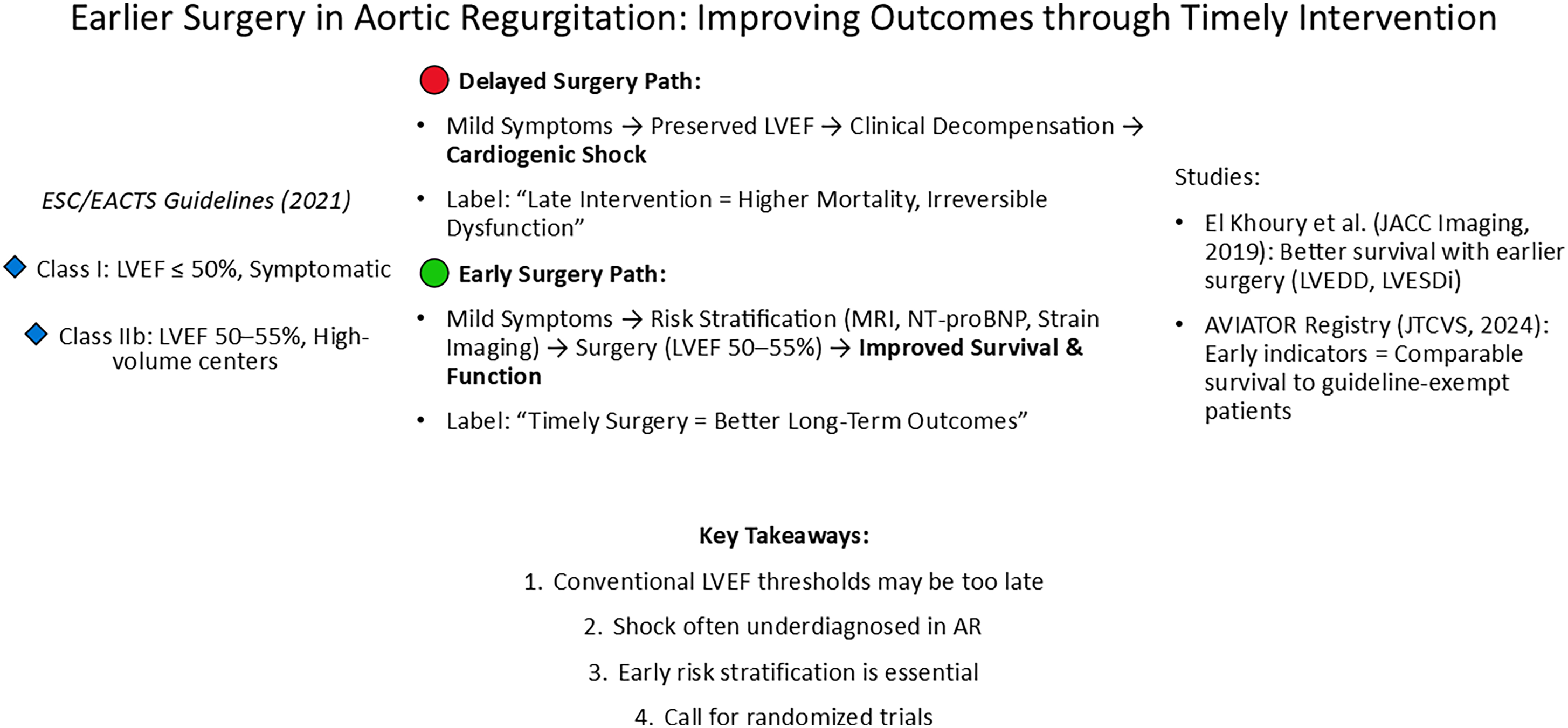
Keywords
Key Points
Earlier surgery in aortic regurgitation improves outcomes
Delaying surgery leads to worse survival and heart function. Patients with LVEF between 50–55% may already benefit from earlier intervention.
Current guidelines might be too conservative
The traditional LVEF cutoff of 50% may be too late for optimal patient outcomes, highlighting the need for reconsideration.
Cardiogenic shock in aortic regurgitation is underestimated
Patients with preserved LVEF may still develop severe shock due to delayed intervention, which is often misrecognised.
Better risk stratification is needed
Advanced imaging (strain analysis, MRI) and biomarkers should guide the timing of surgery more precisely than LVEF alone.
A prospective randomized trial is necessary
Future studies should compare early versus late surgery to establish new evidence-based recommendations.
In the most recent 2021 European Society of Cardiology (ESC)/ European Association of Cardiothoracic Surgery (EACTS) Guidelines for the management of valvular heart disease, 1 surgery for severe aortic regurgitation (AR) is recommended in symptomatic patients regardless of left ventricular (LV) function and in asymptomatic patients with LV end-systolic diameter (LVESD) > 50 mm or indexed LVESD (LVESDi) > 25 mm/m2 body surface area (BSA) or resting LVEF ≤50% (Class I). However, surgery may be considered in asymptomatic patients with LVESDi >20 mm/m2 BSA (especially in patients with small body size) or resting LVEF ≤55% if surgery is carried out at aortic centres of excellence (Class IIb). LV dysfunction is a spectrum of impairment in heart function that may or may not cause symptoms with cardiogenic shock (CS) representing an acute, critical state where this dysfunction is so severe that it leads to life-threatening low blood pressure and inadequate blood flow to organs. Is it, therefore, underestimated in patients with severe AR?
Low cardiac output syndrome and even cardiogenic shock, as its most fatal end of the spectrum, may be underestimated in patients with AR due to the complex interplay between the two conditions. AR can lead to chronic LV volume overload, allowing the heart to adapt and maintain output for long periods, often delaying the onset of obvious heart failure symptoms. 2 When decompensation occurs, it can be sudden and severe, leading to CS (low systolic blood pressure or the requirement of vasopressor support, low cardiac index, pulmonary congestion, absence of hypovolemia, and signs of organ hypoperfusion.3,4 However, the chronic adaptation may mask early signs of LV dysfunction, causing clinicians to miss or underestimate the risk of CS.
Several Factors Contribute to the Underestimation of CS in AR Patients
Atypical presentation: In AR, the left ventricle becomes dilated and hypertrophied over time to accommodate the volume overload caused by the regurgitation of blood from the aorta back into the heart. 2 This adaptation can mask early signs of heart failure and shock, leading to delayed recognition. By the time cardiogenic shock develops, symptoms might be attributed to the chronic progression of AR rather than acute hemodynamic instability.
Preserved systolic function: In the early to middle stages of AR, patients may have relatively preserved or even increased left ventricular ejection fraction, which can give the false impression that the heart is coping well. However, as AR progresses with increasing volume of fibrous tissue and myocyte apoptosis, the left ventricle can suddenly decompensate, leading to shock. 2 Clinicians may underestimate the severity of the underlying left ventricular dysfunction due to initially normal systolic function on echocardiograms.
Difficulties in hemodynamic assessment: In AR, standard monitoring techniques often overestimated the forward stroke volume because of the regurgitant volume. 5 This can obscure the severity of reduced effective cardiac output, making it harder to assess the progression toward cardiogenic shock. Hemodynamic measures like blood pressure might also appear deceptively normal until the late stages. Given the challenges in recognising early LV dysfunction in AR, additional diagnostic tools may aid in detecting latent or impending CS, even in patients with preserved systolic function. Biomarkers such as NT-proBNP, as well as advanced imaging techniques like cardiac MRI with tissue characterisation, could provide valuable insights into myocardial strain, fibrosis, and subclinical dysfunction. These modalities may help refine risk stratification and guide surgical timing before overt decompensation occurs. Integrating such tools into clinical practice could improve early intervention strategies and prevent progression to a critical state.
Gradual progression and compensation: AR can be a slow-progressing condition, allowing the body to compensate for the hemodynamic changes over time. This compensatory phase may lead to clinicians underestimating the risk of acute decompensation and shock, particularly when the patient presents with a more chronic disease course. 6
In the authors’ opinion, two important trials looked into the long-term results of patients who were operated on more aggressively in terms of left ventricular function. First was a study from the Brussels team led by El Khoury, published in JACC: Cardiovascular Imaging in 2019, 7 where they analysed 356 consecutive patients who underwent surgical correction of severe AR. The authors identified improved 10-year survival in patients who had their indication for surgery based on volume overload (LV end-diastolic diameter (LVEDD) and LVESDi used as key metrics to assess the degree of LV dilation and overload) compared to those operated due to heart failure symptoms or LVEF < 50%. Similar results were obtained for cardiovascular survival and hospitalisations for heart failure. They concluded that increased risk associated with a low LVEF is present as soon as LVEF falls below 55%. Second was a recent observational study from the Aortic Valve Insufficiency and Ascending Aorta Aneurysm International Registry (AVIATOR) database, published in The Journal of Thoracic and Cardiovascular Surgery. 8 Hanet and colleagues set out to investigate the prognostic impact of various indications for surgery, including the presence of symptoms, left ventricular ejection fraction (LVEF), and LVESDi, based upon the current established guidelines. After evaluating 1899 patients, those who were operated on ESC/EACTS Class I recommendations had significantly worse outcomes. Patients who underwent surgery based on earlier indicators (LVEF 50-55% or LVESDi 20–25 mm/m²) had survival rates similar to those who never reached conventional guideline-based triggers, suggesting potential benefits of earlier intervention.
In conclusion, while cardiogenic shock is a well-recognized complication of severe AR, it can be underestimated in certain patients because of subtle or delayed clinical signs and the condition's chronic nature. Careful monitoring and early intervention are critical in AR 9 to avoid acute deterioration. Both already mentioned trials report worse postoperative outcomes when patients with severe AR undergo surgery with an ESC/EACTS Class I trigger, including symptoms, low LVEF, and increased LV end-systolic diameter. No doubt, a robust prospective multicentric randomised clinical trial comparing patients with and without LV dysfunction, including cardiogenic shock, should be conducted to address this issue.
Footnotes
Acknowledgements
The authors acknowledged the editorial services of Urska Antonic of UMC Maribor.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.