
Abstract
Background
There are few prospective and large registries on outcomes after aortic valve repair/sparing or replacement in patients with aortic valve regurgitation (AR), with or without ascending aorta aneurysm.
Methods
A total of 2,026 patients enrolled prospectively in The Aortic Valve Insufficiency and ascending aorta Aneurysm InternATiOnal Registry (AVIATOR) were included in this analysis. The primary endpoint was the composite of all-cause death or aortic valve and/or aorta reintervention.
Results
1,630 (80%) received surgical repair/sparing versus replacement in 396 (20%). During a mean follow-up of 3.8 ± 1.9 years, 187 (9.2%) events occurred, including 106 reinterventions and 81 deaths. The incidence of the composite endpoint was higher in the replacement versus repair group (25.3% vs. 11.8%; log-rank p < 0.001). In particular, the incidence of death was higher in the replacement versus repair group (21.9% vs. 4.5%; p < 0.001), while the incidence of reintervention was comparable between groups (8.2% vs. 5.1%; p = 0.16). AR ≥ grade 2 (mild-to-moderate) at discharge (2.9%) was more common in repair versus replacement (3.5% vs. 0.3%; p < 0.0001). AR (Grade 2) at discharge was significantly associated with higher incidence of the primary endpoint (adjusted HR: 2.60 [95% CI 1.01–6.74]; p = 0.04).
Conclusion
Surgical repair was associated with better survival than replacement at mid-term follow-up without increased risk of reoperation. However, the incidence of postoperative AR ≥ grade 2 was higher in repair than in replacement surgery. AR ≥ grade 2 at discharge was a strong predictor for reintervention during follow-up, stressing the importance of achieving complete correction of AR at the time of aortic valve repair.
Graphical abstract summarizing the study design, main hemodynamic outcomes, and adverse event analysis. (Top) This study included 2,026 patients from the multicenter registry AVIATOR (Aortic Valve Insufficiency and ascending aorta Aneurysm InternATiOnal Registry) undergoing surgical aortic valve and/or aorta repair or replacement. (Middle) Temporal changes in aortic valve regurgitation grade before and up to 3 years after surgery. (Bottom) Incidence of adverse clinical events, including the composite of death or reintervention, death alone, and reintervention alone. Weighted HRs (95% confidence intervals) were obtained following inverse probability of treatment weighting analysis. HR = hazard ratio
Introduction
Aortic valve regurgitation (AR) is the third most common valvular heart disease in high-income countries after aortic valve stenosis and mitral valve regurgitation.1,2 Severe AR can be a consequence of primary valve disease and/or aortic root and aortic ascending aortic dilation. Aortic valve (AV) repair has been shown to be a valuable and potentially better alternative to AV replacement, particularly in those with favorable anatomy.3–7 The definition and classification of aortic valve and aorta lesions are decisive in the choice of the adapted surgical strategies. 8
The optimal timing of surgery and the choice between repair and replacement in patients with severe AR, with or without aortic dilation, remain areas of ongoing debate. While there is growing support for earlier intervention to improve long-term repair outcomes, current recommendations remain limited.9,10 This is in part due to the paucity of large, multicenter studies that provide longitudinal clinical outcomes and echocardiographic data to inform practice. Although there is evidence to support the benefit of AV repair in terms of survival and reduced valve-related complications,3–7 most of this evidence arises from single-center studies, limiting its generalizability. 11 Therefore, additional data from large, international, multicenter registries are needed to further guide surgical decision-making and support expanded use of AV repair. 12
The Aortic Valve Insufficiency and ascending aorta Aneurysm InternATiOnal Registry (AVIATOR) is the first longitudinal observational multicenter and international cohort study enrolling patients with aortic valve insufficiency and/or ascending aorta aneurysm undergoing surgical repair or replacement. 12 Baseline data and early results of AVIATOR surgical registry were recently reported. 13
The objective of this study was to compare the 3-year hemodynamic and mid-term clinical hemodynamic outcomes between aortic valve repair/sparing and replacement surgery from the AVIATOR registry participating sites.
Methods
Study Population
The purpose and design of the AVIATOR surgical registry were previously described.12,13 We enrolled 2,026 patients who were operated with AV/aorta repair or replacement between 2013 and 2018. 13 Exclusion criteria included age <18 years, isolated aortic valve stenosis, intervention for active endocarditis or aortic dissection (type A), and incomplete or missing data on surgical procedure. The study population thus includes all consecutive patients with AR (including mixed AV disease) and/or aortic aneurysm (root or tubular ascending aorta) undergoing surgical intervention. This study was approved by the institutional review board of the participating centers. Individual informed consent was waived.
Surgical Technique
In all patients, the choice between AV/aorta repair or replacement was performed based on anatomical suitability and the severity of regurgitation or aortic dilation, adhering to the contemporary clinical guidelines.
Briefly, patients were operated on via median sternotomy, with central aortic cannulation, cardiopulmonary bypass, and aortic cross-clamping. Myocardial protection was achieved using antegrade or retrograde cardioplegia. AV repair techniques included aortic cusp repair, resuspension, and annuloplasty in patients with suitable anatomy.14,15 For patients with concomitant aortic root or ascending aorta dilation, valve-sparing procedures such as reimplantation or remodeling were employed.16,17 AV replacement consisted of the excision of native valve and implantation of a mechanical prothesis, biological prothesis, homograft, or the Ross procedure. Concomitant ascending aorta replacement was performed using tubular grafts in patients with significant dilation.
Echocardiographic and Follow-up Data
Patients had clinical and echocardiographic follow-up through outpatient visits. The AVIATOR registry encourages yearly clinical and echocardiographic examinations. Clinical and echocardiographic data were gathered in the AVIATOR database.12,13
Transthoracic echocardiography was performed using commercially available ultrasound systems at enrollment (preoperative examination), at discharge (postoperative examination), and thereafter repeated annually. Echocardiographic data were available in 92.9% of patients at baseline, 86.1% at discharge, 51.8% at 1-year, 48.6% at 2-year, and 36.3% at 3-year follow-up. All echocardiographic examinations were conducted according to guidelines at the time of enrollment.18–21 The severity of aortic, mitral, and tricuspid regurgitation was graded using a granular classification: (1) none/trace; (2) grade 1 (mild); (3) grade 2 (mild-to-moderate); (4) grade 3 (moderate-to-severe); and (5) grade 4 (severe). Two-dimensional measurements of aortic dimensions were performed at 4 levels: (1) annulus; (2) sinuses of Valsalva (or root); (3) sinotubular junction (STJ); and (4) proximal ascending aorta (or tubular). LV dimensions included LV end-diastolic and systolic dimensions. LVEF was measured using the biplane Simpson method.
Study Endpoints
The primary endpoint was the composite of death from any cause or AV and/or ascending aorta reintervention. The secondary endpoints were: (i) the composite of cardiovascular death or AV and/or ascending aorta reintervention; (ii) the risk of AV and/or ascending aorta reintervention; (iii) postoperative hemodynamic endpoints including: ≥grade 2 (mild-to-moderate) or worsening (≥1 grade) of AR, and/or transaortic mean gradient ≥15 mmHg or increase ≥10 mmHg, (iv) structural aortic changes endpoint including: increase in proximal aortic (sinus or STJ or tubular aorta) > 3 mm.
Statistical Analysis
Continuous data were expressed as mean ± SD or median (interquartile range [IQR]) and tested for the normality of distribution and homogeneity of variances with the Shapiro–Wilk and Levene tests, respectively. Comparison of continuous data was performed using Student's t-test or Wilcoxon–Mann–Whitney test as appropriate. Categorical data were expressed as percentage and compared with the χ2 test or Fisher's exact test as appropriate. Repeated measures mixed models were used to evaluate the changes in aortic dimensions (root, sinotubular junction, and tubular), LV dimensions and LV ejection fraction between the repair and replacement groups from preoperative visit to 3-year follow-up after surgery. Patients undergoing reintervention over the 3-year period after surgery were censored at the time of reintervention, and echocardiographic follow-up beyond the specified time were ignored.
Kaplan–Meier curves and log-rank tests of the time-to-event data were used to compare the survival function according to surgical procedure as well as pre and/or postoperative risk factors. The 30-day clinical and hemodynamic outcomes were compared between the repair and replacement groups using logistic regression. Following inverse probability of treatment weighting (IPTW) adjustment, results were presented as weighted odds ratio (OR) and 95% confidence intervals (CI). The IPTW method is frequently used in observational studies to adjust for confounding factors by creating a weighted sample in which the distribution of measured covariables is balanced between treatment groups. The weights are generated from a propensity score analysis, which estimates the probability of receiving a specific treatment based on observed covariables. This approach simulates the effect of randomization by reducing selection bias, thus providing for a more accurate comparison between treatment groups as in a randomized controlled trial. The variables included in the IPTW analysis are presented in Supplemental Table S1. The weighted analyses were performed to account for the imbalance in preoperative characteristics between repair and replacement groups with respect to the risk of the composite endpoint of all-cause death or reintervention. Multivariable Cox proportional hazards model was used to determine the independent association between surgical intervention type and clinical outcomes (including composite endpoint). The selection of the variables for the multivariable analyses was based on their clinical relevance (i.e. known risk factors) and/or because of their significant association with clinical outcomes in univariable analysis. Results of the Cox models were presented as hazard ratio hazard ratios (HRs) and 95% CI. Subgroup analyses were performed to determine the heterogeneity of surgical procedure in each subgroup of patients. Results were presented as weighted HR and 95% CI to account for the differences between both surgical treatments. A p value <0.05 was considered statistically significant. Statistical analyses were performed with Stata software (V.14.2, StataCorp, College Station, TX).
Results
Study Population
Perioperative clinical and echocardiographic characteristics of the study population are presented in Table 1. Among the 2,026 patients included in the present study, the mean age was 52 ± 16 years and 19% were female. A total of 1,630 (80%) patients received surgical repair, and the remaining 396 (20%) received surgical replacement (Table 1). Patients in the replacement group were older (57 ± 16 vs. 51 ± 15 years; p < 0.001); had more symptoms, higher incidence of diabetes, previous other cardiac surgery, chronic obstructive pulmonary disease, pulmonary hypertension, endocarditis, and as a result presented with higher EuroSCORE II, but had a lower proportion of diagnosed connective tissue disease compared to those in the repair group (Table 1). In terms of echocardiographic characteristics, there were significant differences. Patients in the repair group had a higher prevalence of bicuspid aortic valve (40% vs. 27%, p < 0.001) and larger aortic dimensions including sinus and sinotubular junction (all; p < 0.01), while those in the replacement group had more severe AR (p < 0.001) and a higher prevalence of patients with LVEF <50% (13% vs. 21%, p < 0.001) (Table 1).
Preoperative Characteristics of the Study Population.

Values are mean ± SD or median (25th-75th percentiles). COPD = chronic obstructive pulmonary disease; EuroSCORE II = European System for Cardiac Operative Risk Evaluation II; LV = left ventricular; NYHA = New York Heart Association.
Insulin- or non-insulin-dependent diabetes mellitus.
Operative data, including the type of surgical repair versus replacement are presented in Table 2. Concomitant procedures including coronary artery bypass graft, aortic arch or hemiarch replacement, or other procedures were more common in the replacement versus repair group (40% vs. 29%, p < 0.001). However, bypass time was longer in the repair group than in the replacement group (147 ± 51 vs. 132 ± 63 min, p < 0.001).
Operative Characteristics of the Study Population.

Values are mean ± SD or median (25th-75th percentiles). AV = aortic valve; AVR = aortic valve replacement.
Surgical Treatment, Hemodynamic Endpoints, and Structural Aortic Changes
Figure 1 shows the distribution of AR grade across study timepoints between the treatment groups. In both treatment groups, there was substantial reduction in AR grade at discharge, but patients in the repair group had more AR ≥ grade 2 (≥ mild-to-moderate) than those in the replacement group (3.5% vs. 0.6%; p = 0.002) (Figure 1A and 1B). From discharge to 3-year follow-up, ≥mild-to-moderate AR increased in the repair group but remained stable in the replacement group (at 3-year: 15.8% vs. 0.9%; p < 0.001) (Figure 1). Among the 1,386 patients with echocardiographic follow-up exam over the 3-year period after discharge, 492 (35%) patients had an increase in AR grade (i.e. ≥1 grade). The proportion of patients with an increase in AR grade was greater in the repair than the replacement group (40% vs. 16%; p < 0.001).

Distribution of aortic valve regurgitation grade across study timepoints. Comparison of AR grade (A) and ≥mild-to-moderate AR (B) according to repair and replacement treatments from preoperative visit to 3-year postoperative visit. Numbers on the bars indicate the % of patients. Numbers between brackets indicate the number of patients at each time point. Pre-op = preoperative.
Figure 2 shows the changes in aortic dimensions across study timepoints between the treatment groups. There were significant reductions in aortic dimensions, and comparable changes in aortic dimensions between groups, from discharge to 3-year follow-up (Figure 2). Although there were statistically significant differences between discharge and 3-year follow-up for the repair group, changes in sinotubular and tubular dimensions were clinically relatively small (Figure 2). In subgroup analyses, similar results were observed when considering the type of surgical procedure (root ± valve repair or replacement vs. tubular ± valve repair or replacement) (Supplemental Figures S1 to S3).

Changes in aortic dimensions across study timepoints. Linear prediction of the changes in sinus (A) sinotubular (B) and ascending aorta (C) from preoperative visit to 3-year postoperative visit between repair and replacement treatments. Numbers on the graph indicate mean value ± standard errors.
The hemodynamic endpoints and structural aortic changes (including annulus size and proximal aortic increase) at 1-, 2-, and 3-year follow-up are presented in Supplemental Table S2. Overall, AR > mild remained more common in the repair group, and aortic dimensions remained comparable between both treatment groups (Supplemental Table S2). Changes in LV dimensions and LVEF between both treatment groups are presented in Supplemental Figure S4.
Type of Surgical Procedure Versus Clinical Outcomes
After surgery, clinical follow-up was complete in 1,740 (86%) patients, and 1,113 (55%) patients had clinical follow-up after 3 years. During the overall mean follow-up of 3.8 ± 1.9 years, a total of 187 (9.2%) clinical events occurred, which included 106 (5.2%) reinterventions and 81 (4.2%) deaths (without reintervention). Twenty-two (27%) of the 81 deaths were cardiovascular. Six patients were not included in the survival analysis due to missing clinical event dates.
Twenty (1.0%) patients died within 30 days after surgery, 11 (0.7%) patients in the repair group and 9 (2.3%) in the replacement group (Table 3). Following IPTW adjustment, there was no significant difference in the 30-day mortality rate between groups (weighted OR: 0.84 [95% CI 0.29–2.41]; p = 0.74) (Table 3). Reinterventions were due to AR in 73 (69%) cases, endocarditis in 12 (11%) cases, ascending aorta in 10 (10%) cases, progressive stenosis in 3 (3%) cases, other causes in 7 (7%) cases, and one unknown case (Supplemental Table S3). Furthermore, structural valve dysfunction was the leading cause (85%) for AV dysfunction (Supplemental Table S3). The incidence of reinterventions at 30 days was comparable between repair and replacement procedure (1.5% vs. 1.0%; p = 0.63). Following IPTW adjustment, similar results were obtained for the incidence of reinterventions at 30 days (weighted OR: 1.72 [95% CI 0.33–8.88]; p = 0.52) (Table 3). Notably, the sum of weights (repair group: 1,441 with a mean weight of 1.2 ± 0.3 vs. replacement group: 343 with a mean weight of 5.2 ± 3.4) remained close to the unweighted sample size for both treatment groups, suggesting that the IPTW method did not significantly inflate or deflate the sample size.
30-Day Clinical and Hemodynamic Outcomes.

Figure 3 shows the risk of the composite endpoint of all-cause death or reintervention, as well as the risk of all-cause death and reintervention alone. The cumulative incidence of the composite endpoint was higher in the replacement group than in the repair group (25.3% vs. 11.8%; p < 0.001) (Figure 3A). After multivariable adjustment including pre- and operative risk factors, surgical replacement remained significantly associated with a higher risk of all-cause death or reintervention (Supplemental Table S4). The risk of the composite endpoint of cardiovascular death or reintervention was nonetheless similar between repair and replacement procedure (Supplemental Table S5). When analyzing the two components of the composite endpoint separately, the incidence of all-cause death was higher in the replacement group compared to the repair group (21.9% vs. 4.5%; p < 0.001) (Figure 3B). In contrast, the incidence of reintervention was comparable between groups (8.2% vs. 5.1%; p = 0.16) (Figure 3C). Further IPTW-adjusted analyses showed that the repair group remained significantly associated with a lower risk the composite of all-cause death or reintervention (weighted HR: 0.62 [95% CI 0.38–1.00]; p = 0.05) as well as all-cause death alone (weighted HR: 0.44 [95% CI 0.24–0.79]; p = 0.006) (Supplemental Table S6). There were no significant differences between both procedures for the remaining clinical outcomes (Supplemental Table S6). The risk of the composite endpoint of all-cause death or reintervention, as well as the risk of all-cause death and reintervention alone between repair and replacement in the subset of patients with AR > mild at baseline are presented in Supplemental Figure S5.

Incidence of clinical outcomes according to surgical procedure. Kaplan–Meier curves (A), and Cox adjusted curves (B) of the composite endpoint of all-cause death or reintervention according to surgical procedure. Kaplan–Meier curves of all-cause death (C) and reintervention (D) according to surgical procedure. % are mortality rates at 6-year follow-up. AV = aortic valve; CI = confidence interval; HR = hazard ratio.
Predictors of Clinical Outcomes
Pre and postoperative predictors of the primary endpoint were reported in Supplemental Table S4. Of these predictors, AR ≥ mild-to-moderate at discharge (2.9%) was associated with a 3-fold increase in the incidence of death or reintervention compared to no or mild AR at discharge (34.5% vs. 10.9%; p < 0.001) (Figure 4A). However, the incidence of death was similar between groups (Figure 4B), while the incidence of reintervention was markedly higher for AR ≥ mild-to-moderate at discharge (Figure 4C). Of note, among the patients with available assessment of AR jet eccentricity at discharge (n = 369), those with an AR eccentric jet (24%) had a significantly higher incidence of reintervention compared to those with a central AR jet (22.5% vs. 6.7%; p < 0.001). The increase in AR grade over the 3-year echocardiographic follow-up after discharge (i.e. increase ≥1 grade, n = 492) was also significantly associated with an increased risk of primary endpoint following Cox multivariable analysis (HR: 2.81 [95% CI 1.61–4.92]; p < 0.001) (Supplemental Table S4). Similar results were observed for the composite risk of cardiac mortality or reintervention (HR: 4.29 [95% CI 2.18–8.44]; p < 0.001) (Supplemental Table S5). In exploratory analyses, we found that the repair group, rheumatic disease, and ≥grade 3 (≥moderate) AR at baseline were the strongest predictors of AR ≥ mild-to-moderate at discharge (Supplemental Table S7).
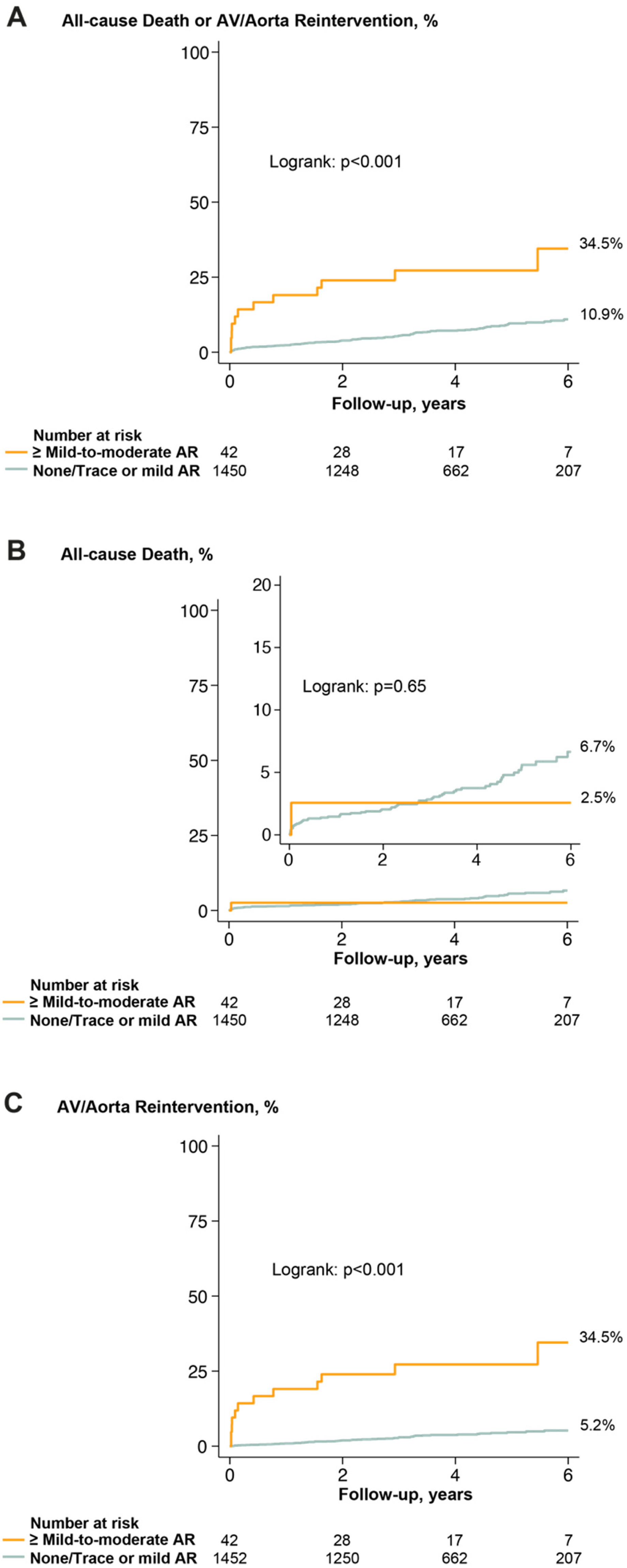
Aortic regurgitation at discharge and incidence of clinical outcomes. Kaplan–Meier curves of the composite endpoint of all-cause death or reintervention (A), all-cause death (B), and reintervention (C). % are mortality rates at 6-year follow-up. AR = aortic valve regurgitation; other abbreviations as in Figure 3.
Treatment Effect and Subgroup Analyses
The weighted interactions between the type of surgical treatment and various subgroups, in relation to the composite endpoint of all-cause death or reintervention, are presented in Supplemental Figure S6. There was no significant interaction between subgroups and surgical intervention type, with only a trend toward a significant interaction for age, sex, and NYHA classification (Supplemental Figure S6).
Discussion
In this 3-year analysis of the AVIATOR surgical registry, the key findings are as follows: (i) surgical repair was associated with better survival than replacement at mid-term follow-up; (ii) aortic dimensions were stable and comparable between repair and replacement intervention through 3 years after surgery; (iii) AR ≥ grade 2 (mild-to-moderate) was more common at hospital discharge in the repair versus replacement group and was significantly associated with an increased risk of reintervention.
Early results from the AVIATOR registry previously indicated encouraging clinical and hemodynamic outcomes following surgery for severe AR and/or aortic aneurysm. 22 The findings of the present study with mid-term follow-up suggest that valve repair may be more effective than valve replacement for the treatment of AR. Surgical repair has the unique advantage of preserving the patient's native aortic valve tissue, which is associated with favorable long-term outcome.3,23,24 It has been suggested that aortic flow-related abnormalities after aortic valve intervention, including eccentricity and vorticity, may play an additional role. 25 Interestingly, in our study, we observed a significant association between aortic jet eccentricity following surgery and an increased incidence of reintervention during follow-up. Moreover, compared to AV repair, replacement is associated with several limitations, including lifelong anticoagulation with mechanical prostheses, limited durability of biological prostheses, and prothesis-related endocarditis or thromboembolism requiring reintervention. 26 In current valvular heart diseases guidelines, AV repair is primarily recommended for selected patients with favorable AV anatomy, especially when both the AV and ascending aorta require surgical intervention.9,10 However, recent updates in the EACTS/STS guidelines for the management of aortic diseases reflect a growing trend toward less restrictive requisites for valve-sparing operations, particularly in cases involving aortic root or ascending aorta dilation when performed by experienced surgeons. 11 This shift acknowledges the increasing evidence supporting the durability and safety of AV repair in expanded patient populations.27,28
In this international multicentric study, the in-hospital (i.e. 30 days) mortality rate and surgical complications were low, which further supports the overall trend towards reduced mortality and morbidity in this population.29–31 While the adjusted risk for the primary endpoint of all-cause death or reintervention was similar at 30 days, surgical repair was associated with lower risk of the primary endpoint and of mortality during subsequent follow-up. These findings are consistent with previous studies suggesting better short-term and mid-term survival in patients receiving surgical repair.32–34 Moreover, a recent meta-analysis of Wong et al. 7 showed a trend toward lower in-hospital and 1-year mortality following surgical repair compared to replacement. However, these previous studies were either limited by: (i) their small sample size; (ii) the lack of appropriate comparison between both surgical interventions; or (iii) the heterogeneous risk profile between patients undergoing repair versus replacement. The favorable survival of patients undergoing surgical repair may have been influenced by their younger age and better risk profile than those undergoing surgical replacement. In contrast to previous studies, we further confirmed the favorable mid-term and long-term survival associated with surgical repair using inverse probability weighting analyses to account for the different risk profiles between repair and replacement. Although this strategy is very effective to compare the characteristics of non-randomized patients, the effect of unmeasured confounding factors cannot be excluded. The survival benefit of AV repair observed in the present study may be also related to the reduced survival associated with mechanical or biological prostheses in patients under 55 years of age. 35 Interestingly, most patients enrolled in this registry underwent surgery prior to their sixties. Furthermore, in the replacement group, most patients received a biological or mechanical aortic valve, with very few undergoing a Ross procedure, which could also have influenced long-term outcomes.36–38
The survival benefit associated with surgical repair should be balanced with other adverse effects including higher risk of residual AR and of reintervention. Previous studies have shown an association between AV repair and the risk of AR at discharge.39,40 In the AVIATOR registry, although there was a significant reduction of AR, repair was associated with increased risk of ≥grade 2 (mild-to-moderate) residual AR at discharge. In addition, surgical repair was associated with worsening of AR over the 3-year follow-up compared to replacement. Importantly, although infrequent (i.e. ∼3%), ≥mild-to-moderate AR at discharge was one of the strongest predictors of reintervention during follow-up. Besides residual AR at discharge, the increase of AR grade during follow-up which was more frequent in repair than replacement (40% vs. 16%), was also significantly associated with an increased risk of composite clinical events, including reintervention. Hence, these findings suggest that residual AR following AV repair remains a major concern, probably mitigating reverse remodeling as confirmed with CMR studies. 41 Further advances in the assessment of AV reparability and surgical standardization as well as strict tolerance of post repair AR (i.e. ≤grade I central) are required to improve the durability of AV repair. Additionally, the longer bypass time in the repair group highlight the need for more technical and technological innovations aimed at reducing the time required for AV repair. Given that surgical repair involves more intricate procedures than replacement, such advancements could broaden the feasibility of repair and expand indications. For instance, improvements in surgical techniques, specialized tools, and intraoperative imaging technologies could significantly reduce operative times while maintaining or improving outcomes.
Previous studies reported durable outcomes after repair of aortic root aneurysm.42,43 However, longitudinal data about the change in aortic size following repair versus replacement are scarce. The present analysis of the AVIATOR registry provides important information about the imaging surveillance of aortic dimensions up to 3 years after surgery. Both repair and replacement procedures were effective to normalize aortic dimensions, which remained stable through 3 years of follow-up. Notwithstanding these findings, further studies with long-term echocardiographic follow-up are needed to confirm these observations.
Clinical Implications
The clinical management and decision-making in non-elderly patients undergoing AV surgery remain challenging. Hence, the results of the AVIATOR registry have important clinical implications and may help in providing tailored management for patients with AR, with or without aortic aneurysm. The short-, mid-, and long-term survival benefit associated with surgical repair provides strong support to this procedure as an alternative to surgical replacement in patients with AS. The presence of residual AR ≥ grade 2 (mild-to-moderate) at discharge was rare but associated with an increased risk of reintervention. These findings suggest that the decision between repair or replacement should be carefully evaluated in light of several factors, including age, anatomic characteristics favoring a complete correction of AR, as well as the patient's preferences. Further studies including randomized clinical trials and longitudinal observational data are needed to corroborate these findings and guide the treatment strategy (i.e. timing and choice of type of intervention) in patients with AR and/or aortic aneurysm.
Study Strengths and Limitations
This study was not a randomized clinical trial; thus, the results of the present analysis should be interpreted with caution. We performed an IPTW analysis to improve balance between treatment groups based on observed covariables; however, this method is still subject to potential residual confounding, especially due to unmeasured covariables. Echocardiographic measures were not analyzed in a central core-lab. Moreover, the attrition rate for echocardiographic follow-up is a limitation of the present study. Hence, predictors of hemodynamic outcomes including residual or increase in transaortic mean gradient could not be assessed due to the study design and the large proportion of missing echocardiographic data during follow-up beyond hospital discharge. The predominance of repair over replacement in the current registry may result from selection bias, with greater involvement of centers primarily performing repair techniques. While there have been considerable advances in repair techniques, this approach to treatment is not yet generalizable.
Nonetheless, the AVIATOR registry represents a unique effort to collect comprehensive clinical, echocardiographic, and long-term outcome data from international multiple centers.
Conclusion
In this study of the AVIATOR registry, surgical repair was associated with better survival than replacement without a significant increased risk for reoperation at mid-term follow-up. Aortic dimensions were stable and similar between repair and replacement intervention during 3-year follow-up. More than mild-to-moderate (Grade 2) residual AR at hospital discharge was rare but more frequent following repair versus replacement and was associated with a markedly increased risk of adverse outcomes including reintervention during follow-up. This study demonstrates the excellent outcomes of aortic valve repair in patients with AR but also stresses the importance of achieving complete correction of AR at the time of the procedure to further optimize postoperative outcomes.
Supplemental Material
sj-docx-1-hvs-10.1177_30494826241300881 - Supplemental material for Mid-term Clinical and Hemodynamic Outcomes in Patients Treated for Aortic Regurgitation and/or Ascending Aorta Aneurysm: The 3-Year Flight of the AVIATOR Registry
Supplemental material, sj-docx-1-hvs-10.1177_30494826241300881 for Mid-term Clinical and Hemodynamic Outcomes in Patients Treated for Aortic Regurgitation and/or Ascending Aorta Aneurysm: The 3-Year Flight of the AVIATOR Registry by Lionel Tastet, Erwan Salaun, Frederieck de Heer, Jolanda Kluin, Ismail El-Hamamsy, Vincent Chauvette, Aline Jazayeri Laubriet, Mikita Karalko, Adrian Kolesar, Igor Rudez, Peter Verbrugghe, Alejandro Crespo de Hubsch, Jaroslav Hlubocký, Rubina Rosa, Marek Jasinski, Sébastien Hecht, Christian Dinges, Patrick Yiu, Fabrizio Ceresa, Ilaria Chirichilli, Laurent de Kerchove, Emmanuel Lansac, Philippe Pibarot and On Behalf of the Aortic Valve Repair Research Network Investigators of AVIATOR Registry in Journal of the Heart Valve Society
Footnotes
Ethical Considerations
This study was approved by the institutional review board of the participating centers. Individual informed consent was waived.
Funding
This research study has been made possible thanks to the HVS AV Database data team, funded by Edwards Lifesciences and Terumo. VC is a Vanier Scholarship recipient. PP holds the Canada Research Chair in Valvular Heart Diseases from CIHR, Ottawa, Ontario, Canada.
Declaration of Conflicting Interests
Dr Pibarot received funding from Edwards Lifesciences and Medtronic for echocardiography core laboratory analyses in the field of transcatheter and surgical aortic valve replacement with no direct personal compensation.
Data Availability
The data of the present study are available from the corresponding author upon reasonable request and after acceptance by the Aortic Valve Repair Research Network Investigators.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.