
Abstract
Valvular heart disease (VHD) is a significant contributor to global cardiovascular morbidity and mortality. Recent advances in transcatheter heart valve therapies have expanded treatable populations and improved outcomes, especially for those at high or intermediate risk. However, clinical management often overlooks the anatomical and functional cardiac damages associated with VHD and overall heart health due to concomitant diseases, focusing primarily on the severity of valvular lesions. To enhance risk stratification and decision-making, Généreux et al proposed a classification scheme for staging cardiac damage (CD) in aortic stenosis (AS) in 2017. This staging system, validated in over 30 studies with approximately 40,000 patients, emphasizes the need to assess extravalvular CD resulting from hemodynamic overload and myocardial dysfunction, which can lead to heart failure. Emerging evidence suggests that CD staging can potentially optimize intervention timing, particularly in asymptomatic patients with severe AS. Integrating CD staging with the traditional severity of VHD may help with the decision-making and improve outcomes. Future research and clinical trials will provide critical insights into the benefits of early intervention based on CD staging. Ultimately, incorporating these CD staging into routine practice could potentially enhance patient management and outcomes across major valvular pathologies.
This is a visual representation of the abstract.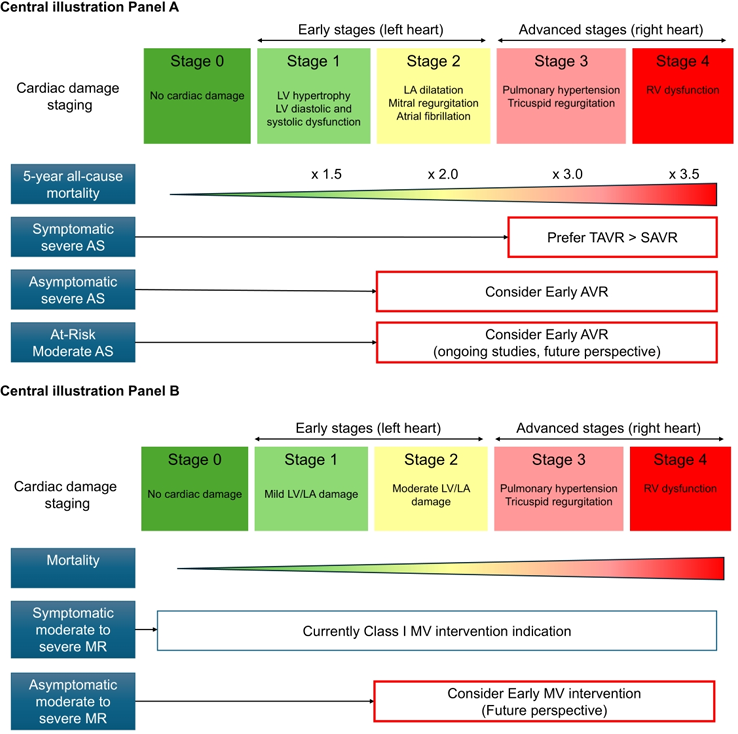
Keywords
Key Points
A CD staging classification, introduced in 2017 for severe aortic stenosis (AS), includes stages: 0 (no damage), 1 (LV damage), 2 (LA or mitral damage), 3 (pulmonary vasculature or tricuspid damage), and 4 (right ventricular damage).
Advanced CD stages are linked to poorer clinical outcomes, and the utility of the CD staging system for risk stratification has been validated across various VHDs, including severe symptomatic AS, asymptomatic AS, moderate AS, significant aortic regurgitation, and mitral regurgitation.
EARLY TAVR results demonstrated that: a) asymptomatic patients with severe AS already had some degree of CD, and b) earlier intervention associated with reduction of unplanned HF hospitalizations.
Randomized control data for management of asymptomatic patients with significant regurgitant valvular disease is lacking. Given the steady growth of transcatheter valve therapies, timely intervention before CD becomes irreversible might be a superior approach requiring proper investigation.
Staging patients with VHD during Heart Team assessment may help identify those who could benefit from additional interventions beyond the valve lesion that is being addressed.
Introduction
Valvular heart disease (VHD) is one of the significant contributors to global cardiovascular morbidity and mortality. Over the past few decades, advances in transcatheter heart valve therapies have significantly expanded the treatable patient population and improved clinical outcomes, especially for those at high and intermediate surgical risk. With these advancements, it is increasingly recognized that the clinical course of VHD is influenced not only by the severity of the valvular lesion but also by the anatomical and functional cardiac damage associated with the VHD as well as concomitant cardiac conditions. Furthermore, even non-severe VHD can impact overall heart health and participate in heart failure symptoms, particularly in patients with preexisting cardiac comorbidities. However, current guidelines do not consistently incorporate these consequences into the decision-making algorithms for determining the optimal timing of intervention.1,2
To enhance risk stratification and therapeutic decision-making, a classification scheme for staging the anatomical and functional damages associated with the VHD - namely, the extent of cardiac damage (CD) - was first proposed for aortic stenosis (AS) by Généreux et al in 2017. Since then, more than 30 studies involving approximately 40,000 patients have validated and adapted this staging system across various AS populations, as well as aortic regurgitation (AR) and mitral regurgitation (MR) in relation to patient outcomes. Extravalvular CD arises from a complex interplay of hemodynamic overload -whether due to pressure or volume overload - ventricular remodeling, and myocardial dysfunction, ultimately leading to heart failure and reduced survival. Thus, it is essential not only to accurately grade the severity of VHD but also to assess the extent of associated extravalvular CD to optimize the timing of intervention, address concomitant comorbidities and ultimately improve outcomes.
In this review, we will explore the current understanding of CD staging in AS, AR, and MR since these are the only types of VHD for which cardiac damage staging has been systematically evaluated. We will also discuss the clinical implications of these staging systems and their potential integration into routine practice to enhance patient management and outcomes.
Cardiac Damage Staging in Aortic Stenosis
Symptomatic Severe AS
With AS progression, pressure overload leads to compensatory left ventricular (LV) hypertrophy, diastolic dysfunction, left atrial (LA) enlargement, the development of mitral and tricuspid regurgitation, and elevated pulmonary artery (PA) pressures. Then right ventricular (RV) dysfunction may develop in some patients over time due to a sustained hemodynamic burden as well as concomitant cardiac disease. A study by Généreux et al using data from the Placement of Aortic Transcatheter Valves (PARTNER) 2A and 2B trials, proposed the first framework for an integrated staging system to quantify these anatomical and functional damages associated with AS progression. 3 This staging classification was used to evaluate the prevalence of CD and the impact of such CD on clinical outcomes in 1661 patients who all underwent either transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR). The classification consists of five stages from stage 0 to stage 4, depending on the presence or absence of extravalvular CD or dysfunction as detected by transthoracic echocardiography (TTE) as shown in Table 1. Patients were hierarchically classified at the worst stage if at least one of the proposed criteria was met within that stage. In this retrospective analysis of severe symptomatic AS patients with intermediate risk, at the time of AVR, 2.8% patients were in Stage 0 (no cardiac damage), 12.8% patients were in Stage 1 (LV damage), 50.8% patients were in Stage 2 (LA or mitral valve damage), 24.9% patients were in Stage 3 (pulmonary vasculature or tricuspid valve damage), and 8.7% patients were in Stage 4 (RV damage) (Figure 1). Patients in more advanced stages tended to be older, predominantly male, with higher the Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM) and the European System for Cardiac Operative Risk Evaluation (EuroSCORE) values. They also had a higher prevalence of diabetes, prior myocardial infarction, coronary artery bypass grafting, frailty, and oxygen-dependent chronic obstructive pulmonary disease (COPD). This finding suggests that the extent of CD is influenced not only by severe AS but also by concomitant conditions. Survival analysis revealed a strong association between the degree of baseline CD and 1-year survival following aortic valve replacement (AVR). The proposed staging classification system provided significant incremental value in predicting 1-year mortality, outperforming several established predictors of poor outcomes after AVR, including patient frailty and the STS-PROM score.
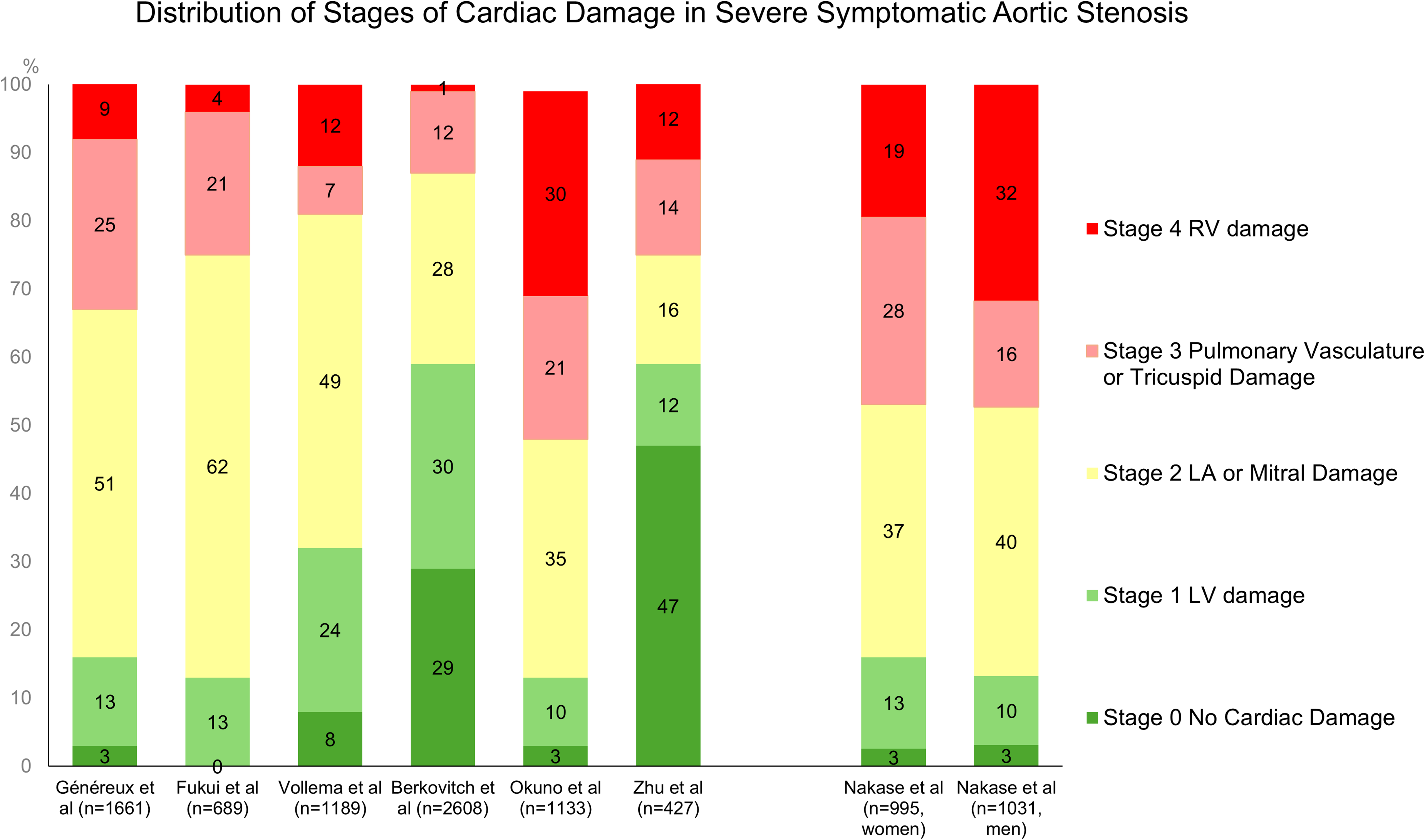
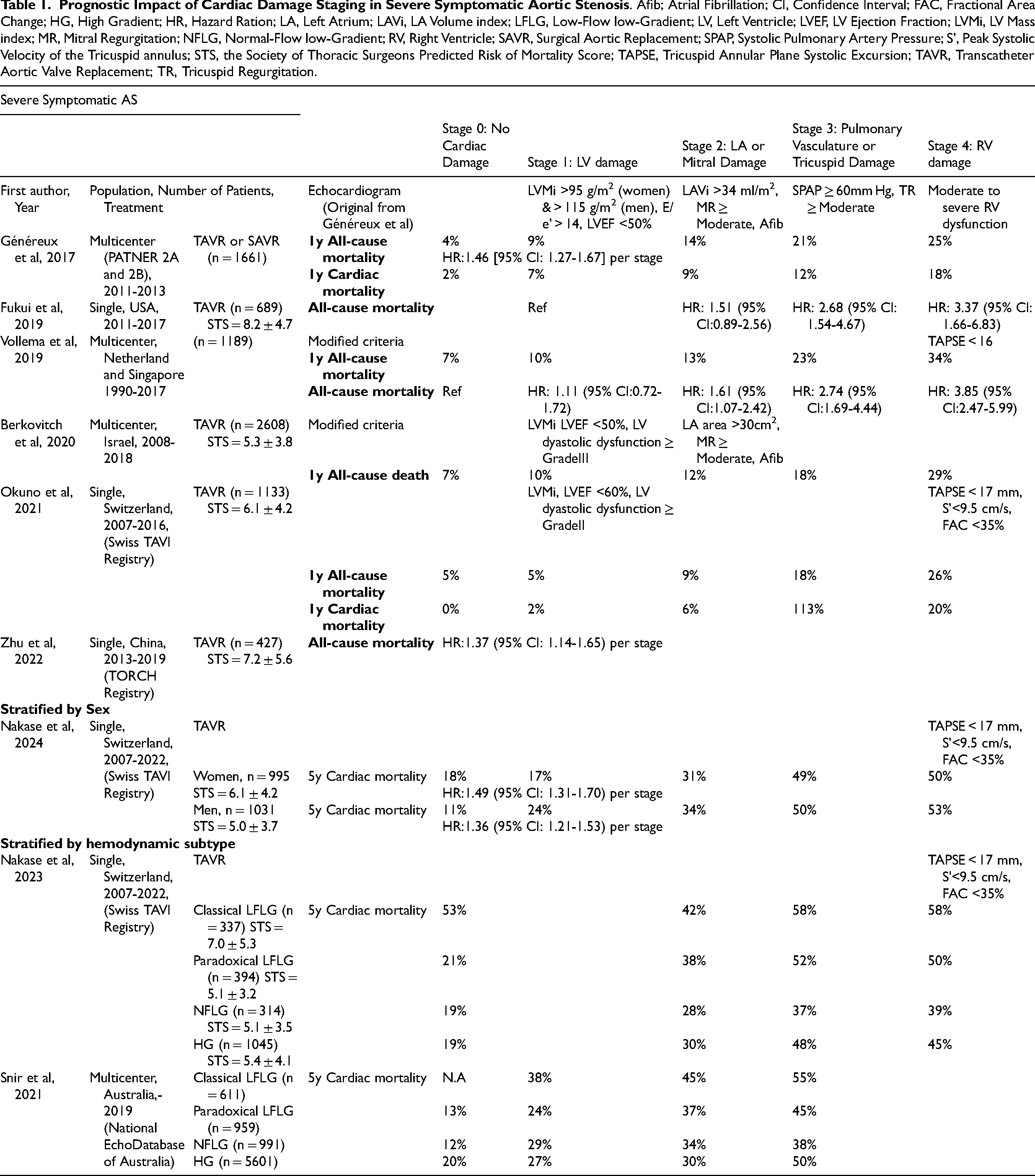
Since then, numerous studies have validated the concept of CD staging using real-world cohorts of patients with severe symptomatic AS.4–8 (Table 1) Most of these studies involved patients who underwent AVR, predominantly through TAVR. Pre-procedure echocardiographic assessments were used to classify the stages of CD. Some variation in methodology for RV functional assessment was noted in the identification of Stage 4 across the studies, reflecting differences in RV functional evaluation among institutions. In the original PARTNER 2 study and the subsequent validation by Fukui et al, Stage 4 RV damage was identified using qualitative visual assessment, which indicated greater than moderate dysfunction in 9% and 4% of patients, respectively. A separate validation study by Vollema et al utilized tricuspid annular plane systolic excursion (TAPSE) < 16 mm, following an earlier echocardiographic guideline, and identified RV damage in 12%.5,9 Furthermore, Okuno et al refined the identification of RV damage by integrating the latest echocardiographic guidelines, using TAPSE < 17 mm, peak systolic velocity (S’) < 9.5 cm/s, and fractional area change (FAC) < 35%, which led to the identification of Stage 4 in 30.5% of the intermediate to high-risk cohort.7,10 Although there were some differences in the prevalence of each stage, the overall staging classification of CD demonstrated a clear, graded association with adverse outcomes, including all-cause and cardiac mortality as shown Table 1. Indeed, the report by Vollema et al showed that the absolute excess all-cause mortality rates at 5 years were +12% for Stage 2 compared to Stage 0 or 1, + 28% for Stage 3, and +37% for Stage 4. 5 Furthermore, multivariable Cox regression analyses across the studies have shown an independent association between each increase in stage and mortality. When evaluating the individual stages of CD, especially Stages 3 and 4, these remained independently associated with mortality. In addition, the staging of CD before AVR was shown to be associated with poor concurrent health status, as measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ) score, as well as a worse health status one year after AVR based on data from the PARTNER 2 and 3 trials. 11
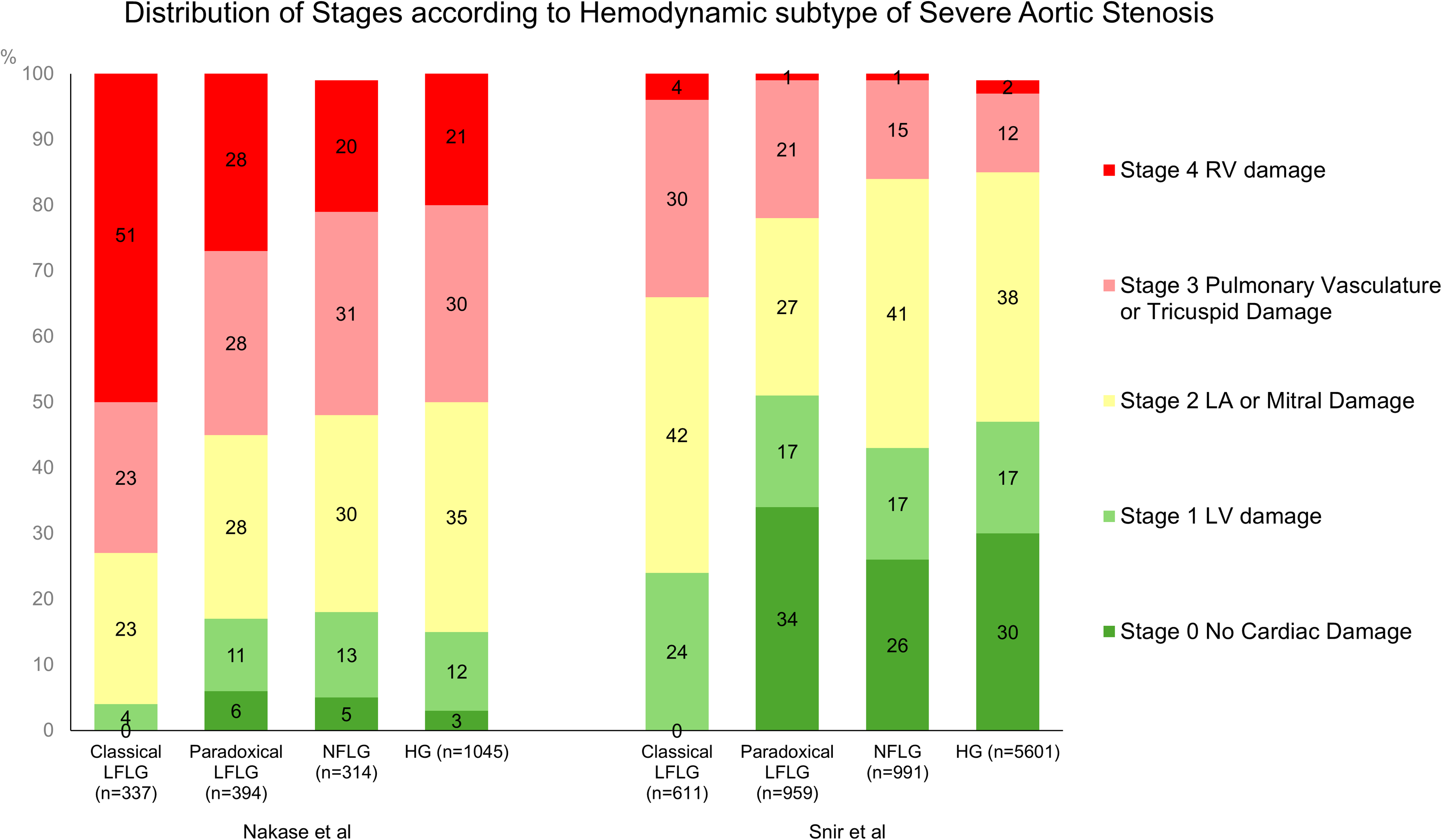
The association between CD staging and mortality has been consistently validated across both genders and different hemodynamic subtypes of AS. According to data from the Swiss TAVI Registry, while Stage 4 CD was more prevalent in men, the overall distribution of early (Stages 0, 1, or 2) and advanced (Stages 3 or 4) stages showed no significant difference between sexes. 12 More advanced CD staging remained a strong predictor of mortality post-TAVR for both men and women. Women demonstrated improved 5-year survival rates in the early stages, though this advantage diminished in the advanced stages. Furthermore, CD staging serves as an effective tool for assessing mortality risk alongside the hemodynamic subtypes of AS. Low-flow low-gradient (LFLG) AS (aortic valve area < 1.0 cm2, aortic valve mean gradient < 40 mg, stroke volume index < 35 ml/m2) are known to be associated with a higher risk of adverse outcomes compared to high-gradient (HG) AS. 13 Data from the National Echo Database of Australia (8162 patients) 14 and the Swiss TAVI Registry (2090 patients) 15 observed that the majority of patients with classical LFLG AS and reduced LVEF presented with advanced cardiac damage (Stage 3 or 4), followed by paradoxical LF LG-AS with preserved LVEF, normal-flow low-gradient (NFLG) AS, and HG-AS.(Figure 2) Mortality rates in both early and advanced stages were highest in patients with classical LF LG-AS, followed by paradoxical LF LG-AS, HG-AS, and NF LG-AS. While advanced cardiac damage increased mortality risk across all AS subtypes, its impact varied between subtypes. Notably, in the report from the Swiss TAVI Registry, the absolute 5-year mortality excess between advanced (Stage 3 or 4) and early (Stage 0, 1, or 2) CD stages was 22% for paradoxical LFLG, 18% for HG, 14% for NFLG, and 10% for classical LFLG AS. 15
Following the validations of the concept of CD in severe AS across multiple large-scale real-world datasets, refined staging classifications have been proposed and evaluated using parameters such as TTE-derived LV global longitudinal strain, 16 stroke volume index, 17 and right ventricular arterial coupling. 18 Additionally, classifications based on invasive hemodynamic19–21 or cardiac CT 22 have also been explored. In all studies, it has been observed that damage to the right heart and pulmonary circulation in advanced stages (Stage 3 or 4) significantly correlates with increased risk of mid- to long-term outcomes compared to early stages (Stage 1 or 2), where damage is confined primarily to the left heart.
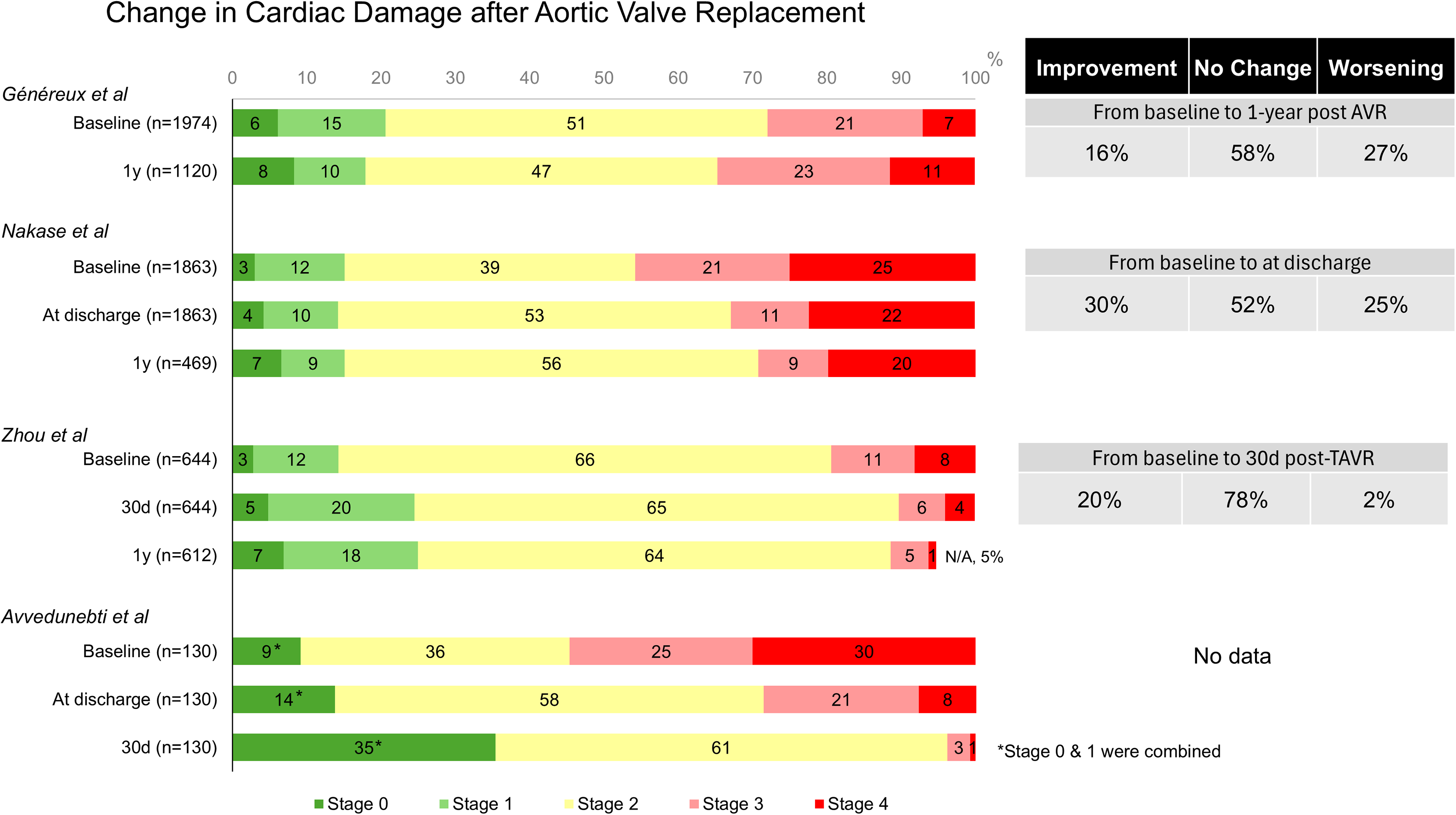
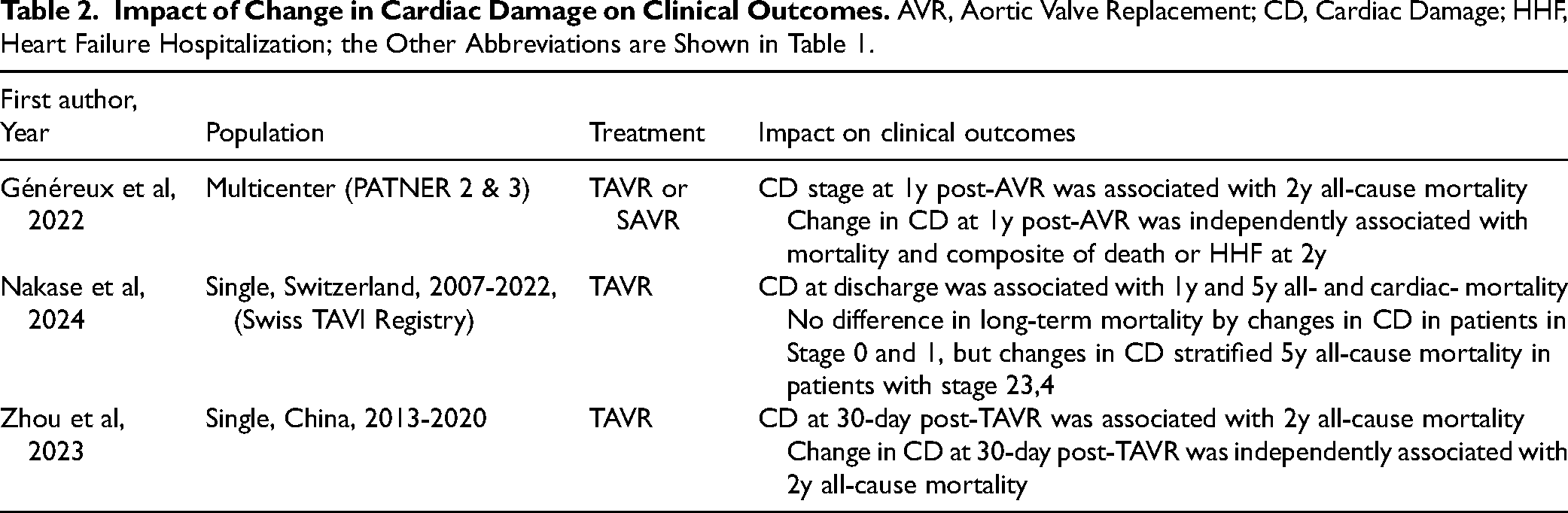
In addition to baseline assessments for CD staging before AVR, the evolution of CD staging post-AVR and its association with subsequent outcomes have also been investigated. In the pooled analysis of the PARTNER 2 and 3 trials, CD stage improved in only 15.6% of patients and deteriorated in 26.5% at one year after AVR. 23 (Figure 3) Additionally, Nakase et al reported from the Swiss TAVI Registry that CD stage improved in 30.1% of patients and deteriorated in 24.7% at discharge. 24 These findings indicate that less than one-third of patients show improvement in CD staging post-AVR, suggesting that valve intervention may be either occurring too late in the disease progression or that a single AV intervention might not be able to revert or correct other concomitant valvular disease or comorbidities. The two-fold difference in improvement rates between the two studies may support the preference for TAVR over SAVR in patients with advanced cardiac damage. This preference arises from the fact that the PARTNER trials included both TAVR and SAVR, whereas the Swiss TAVI Registry focused exclusively on TAVR. Additionally, SAVR is associated with postoperative RV dysfunction due to factors such as cardiopulmonary bypass, incomplete RV myocardial protection during bypass, pericardiectomy, and the subsequent uncoupling of the RV from the pericardial sac. These complications may contribute to the onset of RV dysfunction following SAVR. Another key finding from these studies, along with a report from a single center in China, 25 is that baseline CD stage, as well as residual or unimproved CD early after AVR, are strongly and independently associated with an increased risk of long-term all-cause and cardiac mortality over 2 to 5 years. (Table 2) Furthermore, changes in CD were linked to the degree of health status recovery after AVR. Patients whose CD regressed experienced greater improvements in health status post-AVR compared to those whose CD remained unchanged or deteriorated. 11
Asymptomatic Moderate to Severe AS
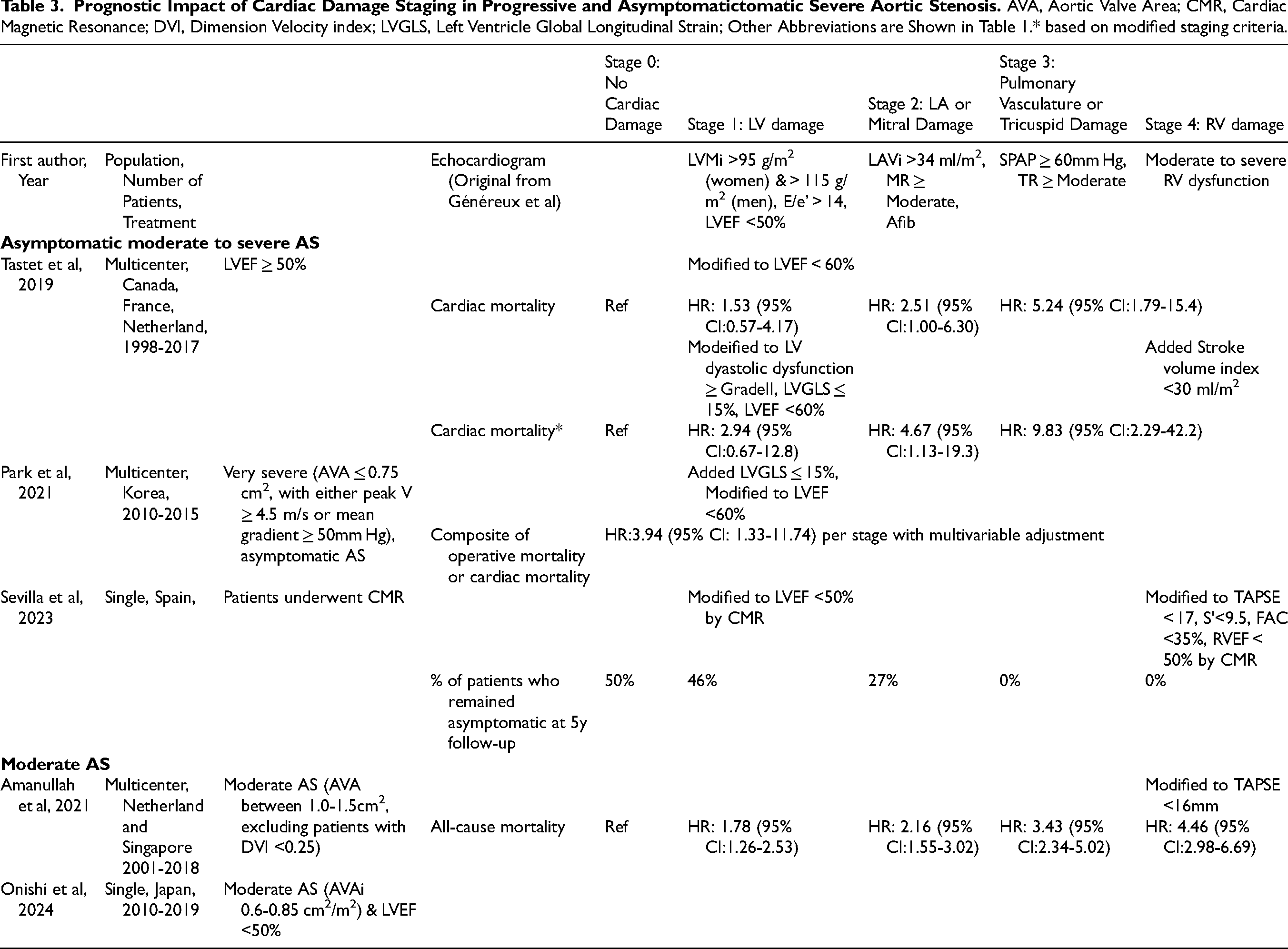
The concept of CD staging has further expanded into the cohort of patients with asymptomatic moderate to severe AS. While current guidelines recommend AVR for patients with severe AS who have symptoms or an LVEF <50%,1,2 the management of those with severe asymptomatic AS and normal LVEF remains debated. In this context, several retrospective studies have explored the usefulness of CD staging (Table 3). A multicenter study by Tastet et al, which included 735 asymptomatic patients with at least moderate AS (defined as an aortic valve area < 1.5 cm²) and preserved LVEF ≥ 50%, found that 15% were in Stage 0, 27% in Stage 1, 50% in Stage 2, 2% in Stage 3, and 6% in Stage 4.(Figure 4) This classification was similar to that used by Généreux et al, with the distinction that LVEF was <60% for Stage 1 instead of ≤50%. 26 This study also tested a modified staging schema, in which impaired LV global longitudinal strain of ≤15% was included as an additional criterion in Stage 1, the elevated LV filling pressures criterion (E/e’ ratio > 14) was replaced by grade ≥ II of LV diastolic function and moderate to severe low-flow state (defined as stroke volume index < 30 ml/m2) was added as a supplemental criterion in Stage 4. The other parameters and criteria were unchanged compared with the original scheme. Irrespective of these modifications, the rate of advanced CD stages (Stage 3 or 4) was lower than that observed in patients with severe AS (4%–30%), consistent with findings from other studies on asymptomatic AS.27,28 Importantly, CD staging has been independently associated with long-term prognosis. Furthermore, Abdelfattah et al performed a meta-analysis of both asymptomatic and symptomatic patients with moderate-to-severe AS. 29 This analysis revealed no significant difference in all-cause or cardiovascular mortality between asymptomatic and symptomatic groups across corresponding CD stages. This highlights the non-benign nature of asymptomatic AS. Additionally, the results suggest that symptoms do not reliably reflect the extent of CD at the time of AVR. The comparable mortality risk seen in both cohorts for those at CD stage ≥ 2 indicates that this threshold could serve as a useful risk stratification tool. This may help identify AS patients who would benefit from earlier intervention and closer echocardiographic monitoring, rather than following the current guideline recommendation of a 2-year follow-up interval.1,2
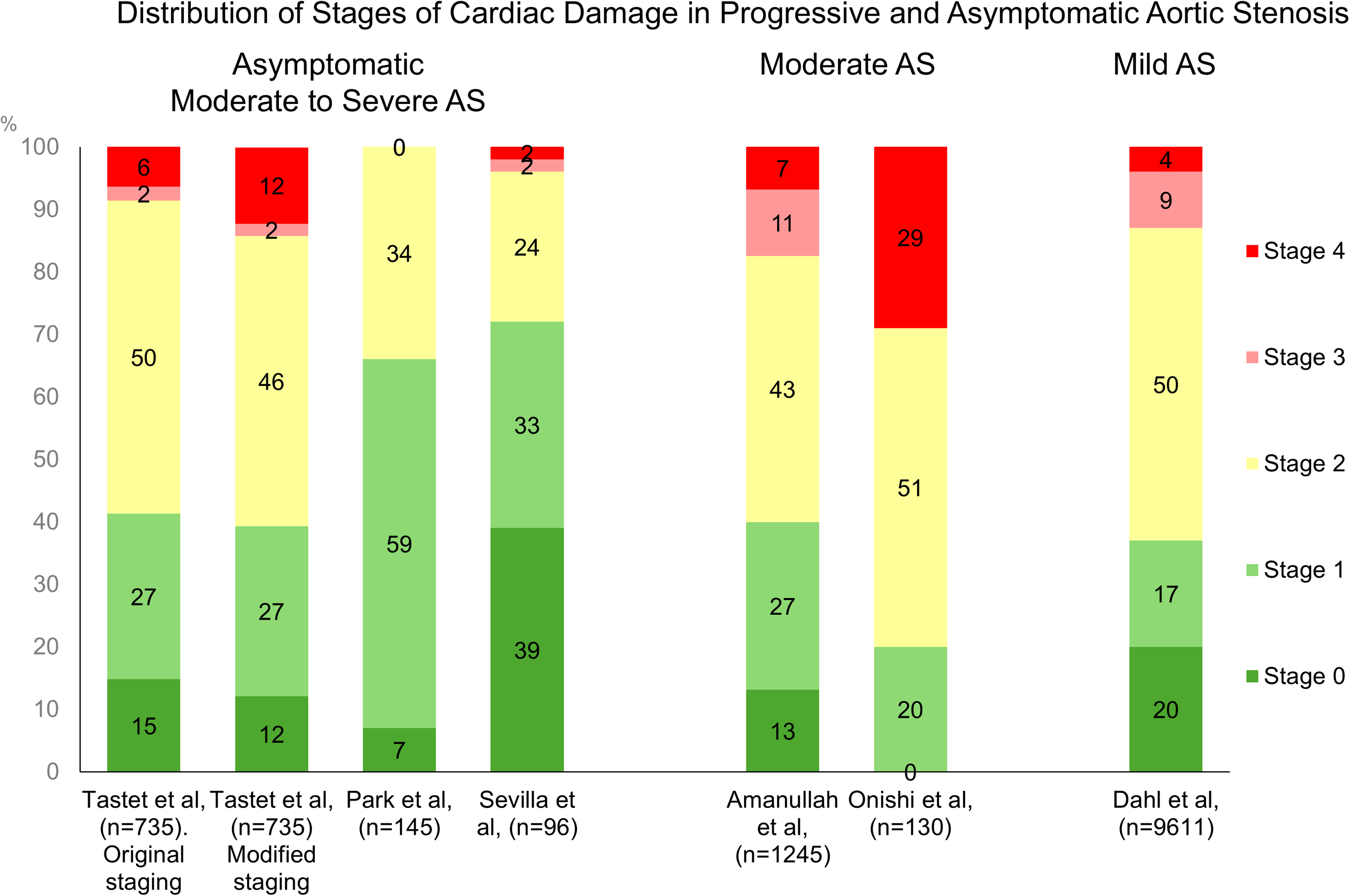
Distribution of Stages of Cardiac Damage in Progressive and Asymptomatic Severe Aortic Stenosis. aS, Aortic Stenosis.
The most recent results of EARLY TAVR (Evaluation of TAVR Compared to Surveillance for Patients With Asymptomatic Severe Aortic Stenosis) study further demonstrated the benefit of earlier intervention by reducing unplanned heart failure (HF) hospitalizations in asymptomatic severe AS patients,
30
supporting the consideration of early, preemptive AV intervention to prevent irreversible CD (
Moderate AS
The current guidelines do not recommend SAVR or TAVR for patients with moderate AS unless there are other compelling factors, such as concurrent cardiac surgery or rapid disease progression.1,2 However, recent data from large echocardiographic national databases suggest that moderate AS is associated with reduced long-term survival, showing a more than two-fold increase in 1-year mortality compared to patients without AS.32,33 Additionally, concomitant conditions such as left or right ventricular dysfunction and mitral or tricuspid regurgitation are known to further elevate mortality risk. Based on these background, the utility of the CD staging system in risk stratification and optimizing the timing of intervention has been investigated in this cohort as well.
A multicenter study from the Netherlands and Singapore demonstrated that extravalvular CD is common, with distribution across stages as follows: 13% in Stage 0, 27% in Stage 1, 43% in Stage 2, 11% in Stage 3, and 7% in Stage 4, using criteria similar to the original proposal by Généreux et al.
34
(Figure 4
Mild AS
Theoretically, with progression of AS severity, CD staging should also advance. However, it remains unclear whether this process is limited to patients with moderate and severe AS. To address this, Dahl et al conducted a study to determine the prevalence of CD in patients with mild AS, to identify factors associated with its presence, and to assess the impact of CD on outcomes. 36 In this large cohort study of 9611 patients with mild AS, all but 20% demonstrated some degree of CD, with 17% classified in Stage 1, 50% in Stage 2, 9% in Stage 3, and 4% in Stage 4.(Figure 4) The greater the CD stage, the worse the clinical outcomes in this cohort, similar with those observed in patients with moderate and severe AS. However, no relationship was found between the degree of CD and AS severity, as indicated by peak aortic valve velocity. Instead, the stage of CD was strongly associated with comorbidities such as hypertension, diabetes, ischemic heart disease, heart failure, chronic kidney disease, chronic pulmonary disease, and peripheral arterial disease. These findings have also been noted in those with moderate and severe AS. This indicates that the CD staging system offers a broader assessment of overall heart health in addition to the direct consequences of AS. It may also support why CD staging changes, even after treatment of severe AS, might not occur. While the CD classification remains useful for providing prognostic information, it should not be used in isolation to determine the optimal timing for AVR It should be considered alongside other clinical and echocardiographic data related to AS severity.
Cardiac Damage Staging in Aortic Regurgitation
Chronic significant AR is characterized by progressive LV volume overload, leading to compensatory LV dilation, initially preserving stroke volume and cardiac output. However, as LV size and wall stress increase, adverse remodeling occurs, including eccentric hypertrophy and reduced ejection fraction. As the disease progresses, chronic AR may also elevate LA pressure, exacerbate mitral and tricuspid regurgitation, and contribute to pulmonary hypertension, further worsening clinical outcomes. Current guidelines for AR recommend AVR only for patients with symptomatic severe AR, or for those with asymptomatic severe AR who have impaired LVEF or significant LV dilatation.1,2 These recommendations are primarily based on small studies conducted a few decades ago. With the advancement of transcatheter therapies for AR, there is a growing debate on the optimal timing for AV intervention in these patients.37,38 Although AS and AR have different initial compensatory mechanisms - concentric hypertrophy in response to pressure overload and eccentric hypertrophy due to volume overload - the downstream cardiac consequences might be common to both conditions. Consequently, the utility of the CD staging system, originally proposed for severe AS, has also been assessed for risk stratification in patients with AR.
Silva et al used the similar CD staging classification proposed by Généreux et al, for severe AS to evaluate the prevalence of CD stages and their prognostic impact in a single center cohort of 571 patients with moderate to severe native chronic AR. 39 The study defined AR using TTE-derived qualitative, semiquantitative, and quantitative parameters. In this study, 12% of the patients were quantified as severe AR, while 33% were asymptomatic. Overall, 14% of patients were classified in Stage 0, 22% in Stage 1, 49% in Stage 2, 12% in Stage 3, and 3% in Stage 4. All-cause death occurred in 11% in Stage 0, 8% in Stage 1, 24% in Stage 2, and 45% in Stage 3 or 4. Survival analysis showed that patients in advanced CD stages experienced higher mortality rates. Furthermore, multivariable Cox regression analysis revealed that Stages 3 and 4 were significantly associated with an increased risk of all-cause mortality (hazard ration (HR) 4.04: 95% confidence interval (CI) 1.73-9.42, p = 0.001).
Cardiac Damage Staging in MR
MR is one of the most common VHDs.
Current guidelines recommend mitral valve (MV) intervention for patients with significant MR, particularly those with symptoms, LVEF ≤ 60%, LV end-systolic diameter (LVESD) ≥ 40 mm, or new-onset atrial fibrillation and/or pulmonary hypertension.1,2 While several nonrandomized studies suggest better outcomes with early MV intervention compared to watchful waiting,40,41 management of asymptomatic patients with significant MR remains controversial unless curative surgery is likely, ie, the likelihood of a successful and durable repair without residual MR is >95% with an expected mortality rate <1%. Since neither approach is universally optimal for all asymptomatic patients, treatment decisions and intervention timing must be individualized based on MR severity, center's expertise for successful MV repair and the patient's risk profile. To aid in comprehensive assessment, a modified CD staging system for MR has been proposed and evaluated in cohorts of both primary and secondary M.Primary MR
Primary MR is caused by a primary problem of the MV leaflets and/or subvalvular MV apparatus (prolapse, flail, etc) resulting in chronic volume overload of the LA, which leads to atrial dilation and increases the risk of arrhythmias, particularly atrial fibrillation. The resulting volume overload on the LA and further the LV leads to progressive LV dilation and compensatory hypertrophy to sustain forward cardiac output. Overtime, this adaptation can impair LV systolic function. In advanced stages, persistently increased LA pressure may lead to pulmonary hypertension, tricuspid regurgitation, and ultimately right heart failure. Considering the similar pathophysiological processes, aside from the volume overload on the LA in MR and the pressure overload on the LV in AS, van Wijngaarden et al 42 and Bernard et al 43 each adapted the initial classification developed for AS to separate MR cohorts. Both proposed a modified classification system that incorporates cutoff criteria within each stage, aligning with guideline recommendations such as LVEF ≤ 60% and LVESD ≥ 40 mm. 1 As shown in Table 4, the two studies applied slightly different criteria for each stage and cohort of patients. One study focused on patients with greater than moderate to severe primary MR who underwent MV surgery, 42 while the other involved asymptomatic patients with moderate or severe primary MR. 3 Although they observed slight variations in the prevalence of CD stages (Figure 5), both studies demonstrated an increase in mortality associated with a greater extent of CD. Notably, more than one-third of patients had some degree of CD even before surgery or during the asymptomatic phase. This finding reinforces the idea that, for most patients, the appearance of symptoms signifies an advancement of the disease to a more severe stage. Current guidelines mainly rely on symptom presence to determine the timing of intervention. However, this approach is subjective and can be challenging to assess in patients, especially when considering other medical conditions and the aging process.
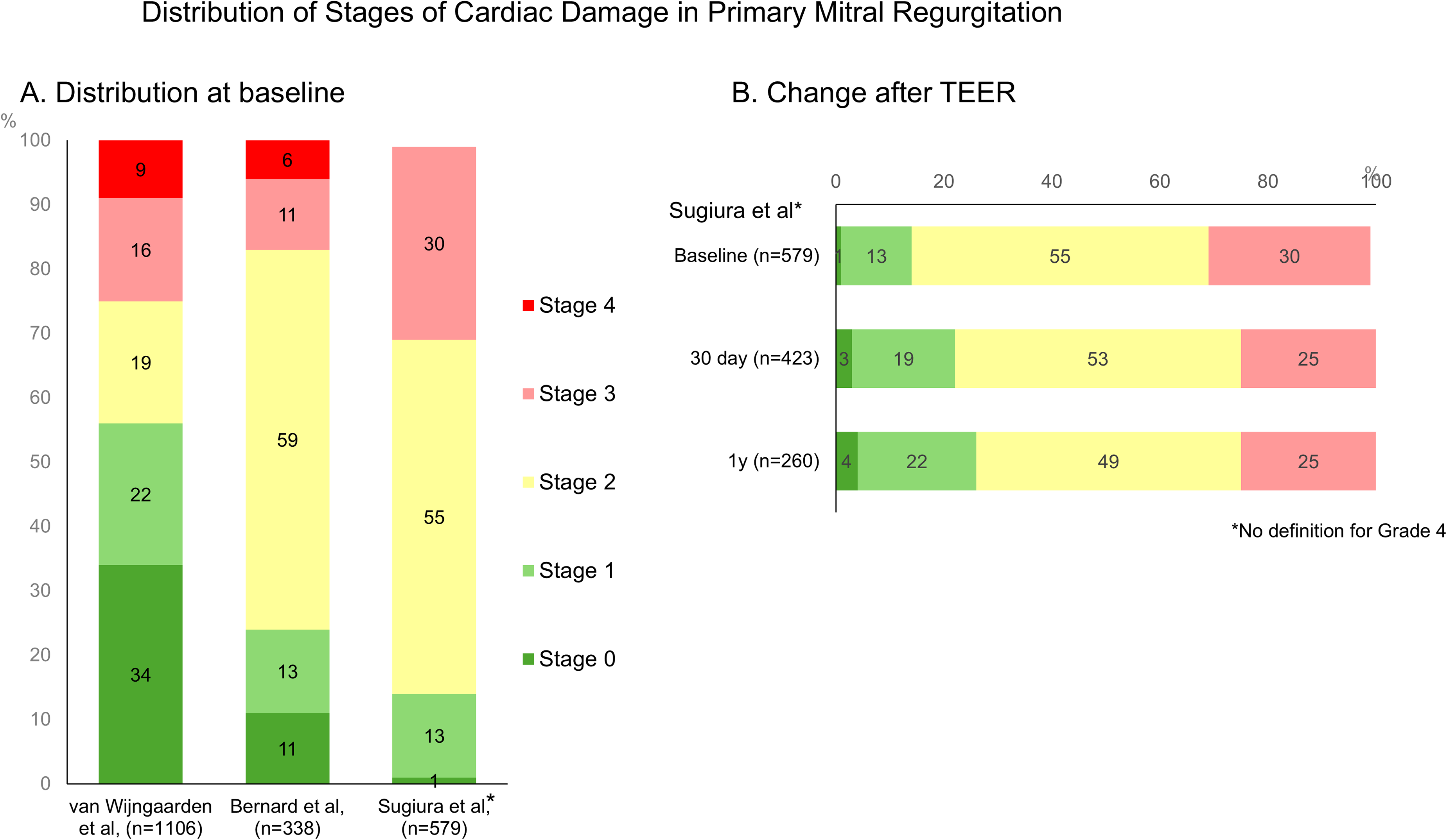
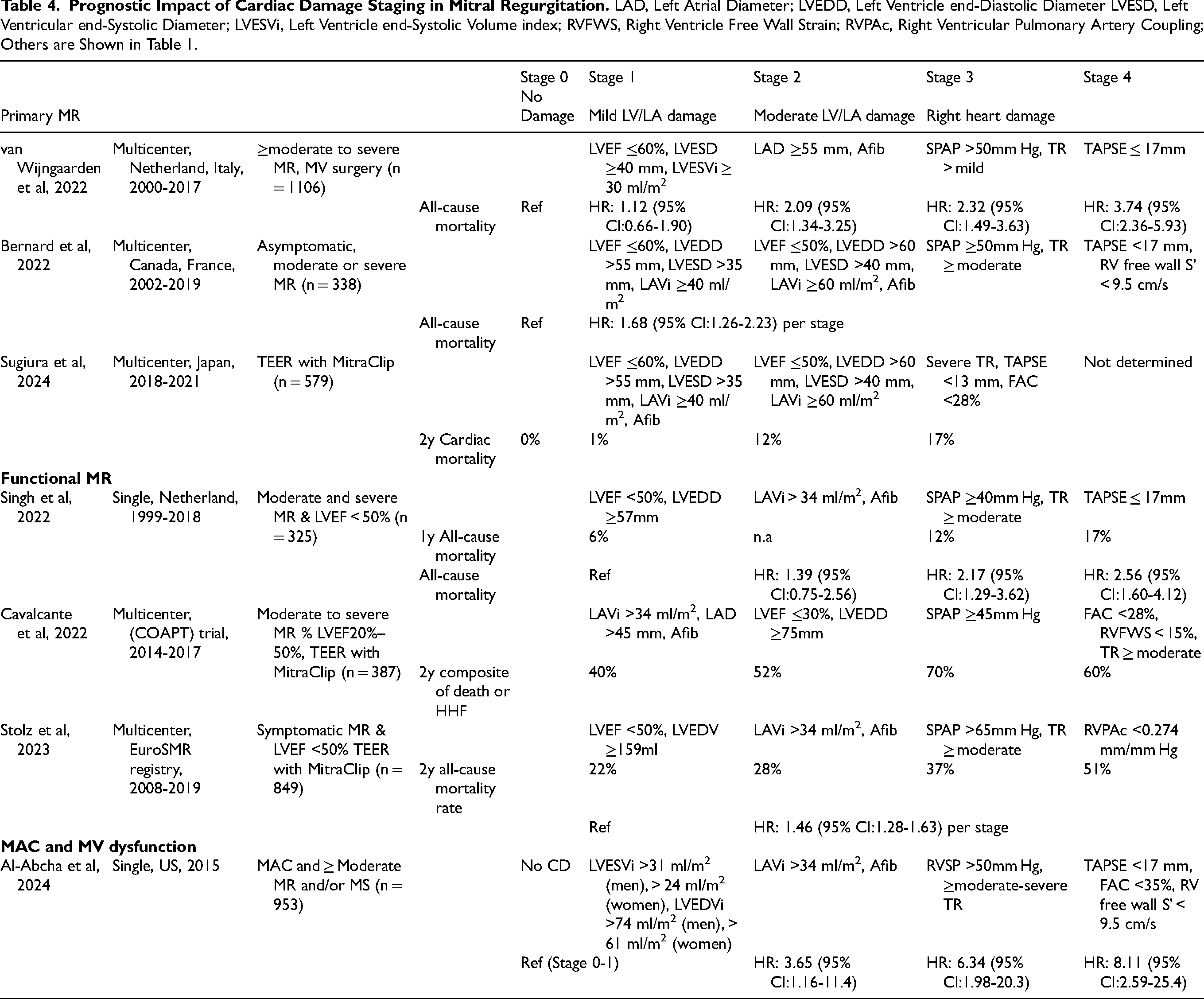
Treatment options have now expanded from surgery alone to also include transcatheter edge-to-edge repair (TEER) therapies, which reduce perioperative complications.44–46 Sugiura et al, using data from a multicenter registry in Japan, assessed the extent of CD in patients undergoing TEER for primary MR and examined its association with clinical outcomes. 47 Although slightly different criteria from the previous studies were applied, nearly all patients (98.6%) exhibited some degree of CD at baseline prior to TEER, with 1.4% in Stage 0, 13% in Stage 1, 55% in Stage 2, and 30% in Stage 3 (Figure 5). In this study, the 2-year mortality rate was 0% in patients without any signs of CD (Stage 0). Mortality increased to 10.5% in patients with mild LV or LA damage (Stage 1), 21.1% in those with moderate LV or LA damage (Stage 2), and 24% in patients with right heart damage (Stage 3). This association between CD staging and increased mortality risk remained significant after adjusting for residual MR and comorbidities. Notably, despite a modest downgrading of CD staging over time, 74% of patients still had Stage 2 or 3 CD 1-year after TEER. These findings suggest that earlier intervention may be warranted before CD progresses to advanced stages, in order to maximize the benefits of MV intervention.
Functional MR
Functional (secondary) MR occurs when the MV is structurally normal, but impaired LV function (eg, from ischemic heart disease or dilated cardiomyopathy) and/or LA dysfunction (eg, due to atrial fibrillation) causes annular dilation, altered valve geometry, and imbalance of opening and closing forces, resulting in inadequate leaflet coaptation and subsequent regurgitation. This pathological process is distinct from primary MR; however, CD staging classification may still hold clinical significance.
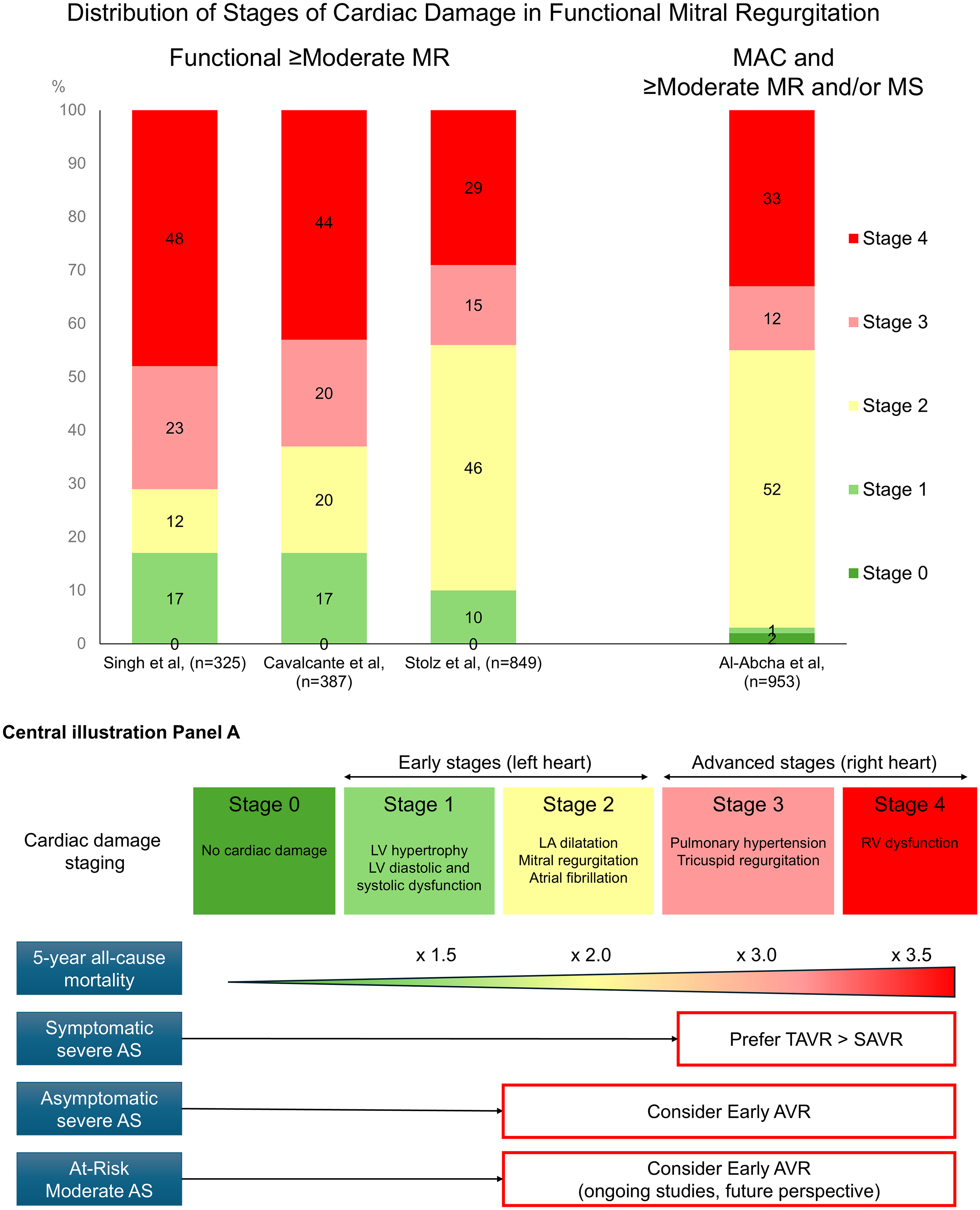
Singh et al, using a single center cohort of 325 patients with moderate and severe functional MR and reduced LVEF <50%, assessed the prevalence of CD and its impact on clinical outcomes.
48
Given the nature of functional MR, no cardiac damage was not defined. LV involvement was noted in 17% of patients, LA involvement in 12%, tricuspid valve or pulmonary artery vascular involvement in 23%, and RV involvement in 48%. (Figure 6
Mitral annulus Calcification (MAC) and MV Dysfunction
MAC is a progressive degenerative process affecting the mitral annulus. This condition is associated with various comorbidities and can lead to adverse outcomes.
Transcatheter mitral valve replacement has emerged as an alternative for patients at high surgical risk, including those with significant MAC. However, the overall outcomes of MV interventions may be influenced by comorbidities associated with MAC. Thus, understanding the stages of extramitral CD related to MAC could be crucial in the treatment decision-making process. Al-Abcha et al, using a single-center cohort of 953 patients with MAC and ≥ moderate MR and/or MS, found that the majority of patients (98%) had extramitral CD with 1.6% in stage 0, 1.4% in stage 1, 52.4% in stage 2, 12.1% in stage 3, and 32.6% in stage 4 (Figure 6). 51 Consistent with findings in primary and functional MR cohorts, more advanced stages were associated with higher rates of all-cause mortality and HF hospitalization. This trend persisted in a subgroup of patients with moderate or severe MAC, with those in Stages 3 and 4 showing significantly elevated mortality and HF hospitalization rates.
Future Directions
Due to the challenges in accurately assessing MR severity in some patients and the subjective nature of symptom reporting, a more objective and comprehensive approach may be beneficial for identifying more appropriate timing of intervention. The utility of the CD staging system in risk stratification has been validated across various etiologies of MR and treatment intervention cohorts. Thus, incorporating CD staging alongside conventional MR grading could provide a clearer framework and simplify decision-making (
Consideration of Cardiac Comorbidities in CD Staging of VHD
The clinical relevance of CD staging has been established across AS, AR, and MR, as demonstrated thus far. In patients with VHD who have no other cardiac comorbidities, the progression of CD staging is theoretically considered to primarily reflect the severity of VHD itself. Conversely, in patients with VHD and multiple cardiac conditions, CD staging is likely to reflect overall heart health, encompassing both the direct effects of VHD and the burden of associated cardiac comorbidities. This concept is supported by consistent findings showing that the advancement of CD staging is associated with a higher prevalence of comorbidities, irrespective of the type or severity of VHD. Nevertheless, the value of CD staging in risk stratification and outcome prediction remains significant. While the CD staging strategy has the potential to guideline earlier intervention, there is currently no prospective randomized controlled data supporting earlier intervention based on CD staging.
Even when CD progression is partially or entirely driven by other comorbidities, the LV and other cardiac chambers are more vulnerable to the hemodynamic stress imposed by VHD. This suggests that early treatment of non-severe VHD might improve clinical outcomes in some patients with advanced CD stages. However, in other patients with advanced CD stages, treating non-severe VHD may prove futile. Further studies are needed to validate these hypotheses. It is also important to consider that early treatment with a bioprosthetic valve implant starts the clock on valve degeneration. Additionally, it exposes the patient to potential prosthetic valve complications, such as valve thrombosis and endocarditis. Taking these various perspectives into account, the principle of proportionality of the VHD severity in relation to the CD stage will be deserved for more extensive discussion in the future.
Conclusion
The CD staging classification, originally developed for severe symptomatic AS, has proven to be a valuable tool for risk stratification across various severity of AS, and significant AR and M.Advanced CD stages that could be induced by VHD as well as comorbidities such as coronary artery disease and COPD, are associated with poorer outcomes. Integrating CD staging into Heart Team assessments may not only enhance risk stratification but also help identify opportunities for addressing broader cardiac damage, potentially improving patient outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.