
Abstract
Purpose
The aim of this study was to analyze 15 years of all-comers experience in sutureless valves at our center.
Methods
In this monocentric, retrospective study, all patients who received a sutureless valve between 2007 and June 2022 at our center were included (N = 1136). The inclusion criteria were any sutureless aortic valve replacement (AVR), regardless of combined procedures. Follow-up data were included until June 31, 2022. A competing risk analysis using cumulative incidences was used for the long-term endpoints.
Results
A total of 1136 patients received a sutureless valve, with a median age of 79 years (interquartile range [IQR]: 75-82) and 50.2% male. The median EuroSCORE II was 4.1 (IQR: 2.4%-7.2%). 44.5% of procedures were single AVR, 27.1% were AVR with coronary artery bypass graft, and 28.1% were multiple concomitant procedures. In-hospital mortality was 3.4% (n = 39), postoperative complications include 4.2% reoperation for bleeding, a 1.8% stroke rate, and 1.4% need for new dialysis. Survival at 5 years was 71.1% and 25.2% at 10 years. Long-term valve-related events included endocarditis and severe structural valve deterioration (SVD), with an incidence rate of 0.50% for endocarditis and 0.74% for severe SVD.
Conclusions
Sutureless AVR can be used in various settings, as it is suitable for both minimally invasive single AVR and in difficult combined procedures, where it saves valuable cross-clamp time. Our study shows favorable early and late outcomes with low rates of endocarditis, severe SVD, and need for reintervention.
This is a visual representation of the abstract.
Introduction
Guidelines increasingly name transcatheter aortic valve replacement (TAVR) as the gold standard treatment for aortic valve replacement (AVR) in older patients due to its less invasive features, and non-inferiority compared to surgery. In turn, this led to push surgical alternatives towards less invasive techniques and treatments as well. Sutureless aortic valve replacement (SU-AVR) is one example of this innovation push in surgical AVR to keep up with TAVR.1–3
In 2007, a new sutureless aortic bioprosthetic valve—Perceval™ S—was introduced into the world of cardiac surgery. The Perceval™ valve (Corcym srl, Milan, Italy) is a bovine bioprosthetic valve utilizing a self-expanding nitinol frame that deploys and positions the valve without the need for additional sutures. SU-AVR enables faster implantation, lower cardiopulmonary bypass (CPB), and cross-clamp times and was developed to combine fast implantation and the benefits of a surgical approach.4,5 The Perceval™ valve has shown a stable hemodynamic performance with acceptable gradients, safety, and versatility however, good long-term durability is important and needs to be investigated.6,7 Over the 15 years of Perceval's use, several design and usage changes have been made. In October 2017, following a root-cause analysis that identified oversizing as the main cause of complications, the manufacturer issued new recommendations for proper sizing of the sutureless valve, improving hemodynamic performance and patient outcomes. 8 At the end of 2020, Perceval™ Plus introduced 2 major changes: the introduction of the FREE tissue treatment and a reduction in the height of the inflow ring in the XL size. 9
The purpose of this study was to evaluate the outcome of the Perceval™ valve after 15 years of continued use, in 1136 patients at our institution.
Methods
Study design
In this retrospective, single-center study, all patients who received a sutureless valve (Perceval™) between 2007 and June 2022 at our center (University Hospitals Leuven) were included (N = 1136). The inclusion criteria were any sutureless AVR, regardless of combined procedures (coronary artery bypass graft [CABG] and/or multiple valves). Data on patient's characteristics, operative and follow-up data were retrospectively extracted from patient's records, in accordance with regulations on data protection. Follow-up data were included until June 31, 2022. Permission to perform this analysis was granted by the ethics committee UZ/KU Leuven on December 7, 2020, with approval number s64845. Informed consent was not required because of the retrospective nature of this study. Data regarding included patients whom since index operation underwent valve-in-valve TAVR (ViV TAVR) were extracted from a TAVR registry with approval number s61523.
Outcome variables
The main outcome measures of this study were long-term survival and freedom of AV reintervention at 10 years, with incidence rates calculated by the number of events divided by the total patient-years and expressed as a percentage per patient-year (% PPY). The iEOA was calculated for all patients of whom the effective orifice area (EOA) was measured at discharge. Patient prosthesis mismatch (PPM) was defined by the indexed effective orifice area (iEOA) in accordance with VARC-3, with moderate PPM defined as an iEOA between 0.85-0.66 for patients with a BMI <30 and 0.70-0.56 for patients with a BMI >30. Severe PPM was defined as an iEOA ≤0.65 or ≤0.55 for patients with a BMI <30 and >30, respectively. 10 Severe structural valve deterioration (SVD) was defined as the presence of central valve insufficiency of >2/4, an increase in mean gradient >20 mmHg, or a mean gradient >40 mmHg, in accordance with the standardized definitions by ESC/EACTS/EAPCI. 11
Statistical analysis
Statistical analysis was performed using SPSS and RStudio. Continuous data are presented as mean ± standard deviation (SD) or median and interquartile range (IQR). Categorical data are presented as frequency and percentage. Survival analysis and Cox univariate and multivariate regression were performed using the “Survival” package in RStudio. Variables with a P .10 in univariate analyses or with known associations with the outcomes of interest were used for multivariate analyses. Competing risk analysis with all-cause mortality, onset of endocarditis of the bioprosthetic valve or SVD as competing events were performed using the “ggsurvfit” package. Figures were truncated at number at risk lower than 10.
Results
Study population
Between 2007 and 2022, 1136 patients underwent sutureless AVR. The median age of our patients was 79 years (IQR 75-82), with 43.3% octogenarians. 50.2% male and the median EuroSCORE II was 4.2% (IQR: 2.4-7.7) (Table 1).
Preoperative characteristics.
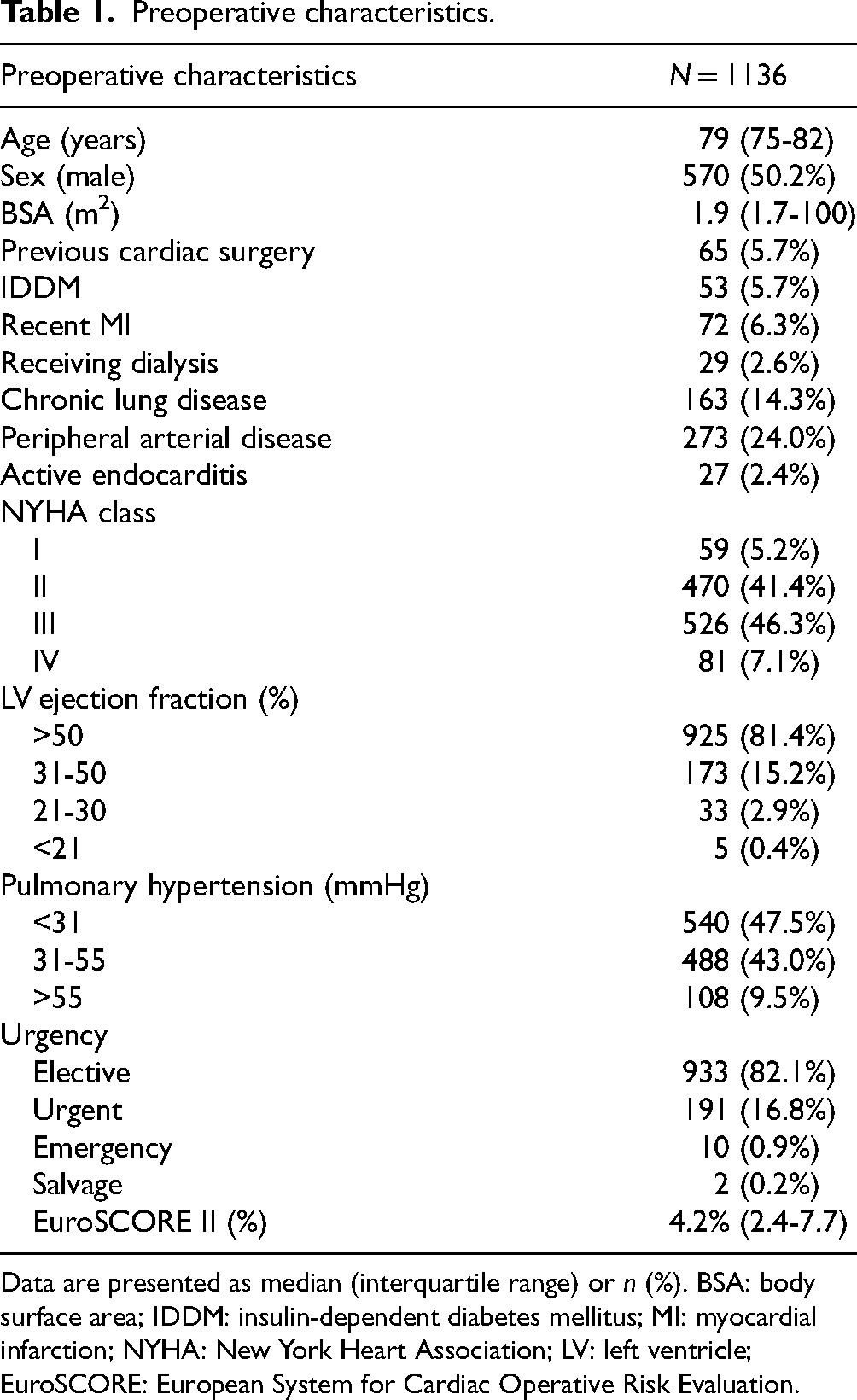
Data are presented as median (interquartile range) or n (%). BSA: body surface area; IDDM: insulin-dependent diabetes mellitus; MI: myocardial infarction; NYHA: New York Heart Association; LV: left ventricle; EuroSCORE: European System for Cardiac Operative Risk Evaluation.
Of all interventions, 44.5% were single AVR, concomitant CABG occurred in 27.1% of patients and 28.1% underwent multiple procedures such as multiple valve replacement. Most patients were treated through a full median sternotomy (751 patients, 66.1%), within the single AVR subgroup, the most used approach was minimally invasive (74.3%), either by mini-sternotomy or anterior right thoracotomy (Table 2).
Intraoperative characteristics.
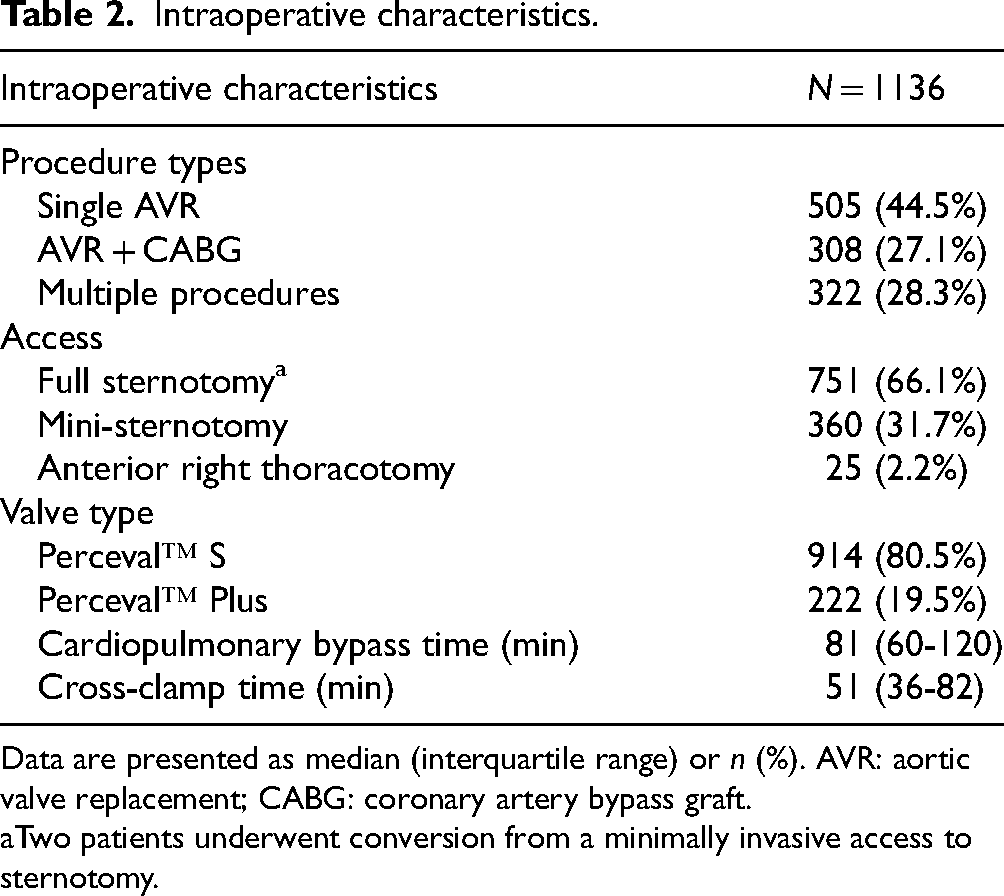
Data are presented as median (interquartile range) or n (%). AVR: aortic valve replacement; CABG: coronary artery bypass graft.
Two patients underwent conversion from a minimally invasive access to sternotomy.
Early outcome
The in-hospital mortality rate was 3.4% (n = 39). Postoperative stroke occurred in 1.8% of patients, 16 patients (1.4%) had had acute renal failure requiring dialysis, and 4.2% of patients required reoperation for bleeding (Table 3). Permanent pacemaker implantation (PPI) was necessary in 8.1% of patients. Within the different time periods, the pacemaker rate decreased from 11.0% in the OLD sizing cohort to 6.1% in the new sizing cohort and 6.8% in Perceval™ Plus. Median hospitalization length was 10 days (IQR: 7-14) with a median intensive care unit (ICU) stay of 3 days (2-5), although 237 patients (20.9%) were not transferred to ICU and were fast-tracked to the ward.
Postoperative events.

Data are presented as median (interquartile range) or n (%).
ICU LOS of non-fast-tracked patients
Hemodynamic results at discharge include a peak and mean gradient of 23 (IQR: 18-30) and 13 (IQR 10-17) mmHg (Table 4). The median EOA and iEOA were 1.6 cm2 (IQR: 1.3-2.0) and 0.9 cm2/m2 (IQR: 0.7-1.1). Paravalvular leakage of >1/4 occurred in 1.8% of patients. Moderate and severe PPM were 24.6% and 12.3%, respectively.
Discharge echocardiographic data.

Data are presented as median (interquartile range) or n (%). EOA: effective orifice area; iEOA: indexed effective orifice area; PPM: patient prosthesis mismatch.
Late outcome
During a cumulative follow-up time of 3775.7 patient-years, the median survival time was 7.2 years (±0.3 years) (Kaplan-Meier estimate), 5-year survival was 71.1% and 10-year survival was 25.2%. Freedom from reoperation was 97.8% at 5 years and 95.3% at 10 years. Endocarditis incidence rate of 0.50% PPY, 14 patients (1.2%) underwent reoperation for endocarditis, which translates to an incidence of 0.37% PPY. SVD incidence rate of 0.74% PPY (Figure 1). Predictors for developing SVD were investigated and shown in Table 5. Overall, the transprosthetic gradients remained stable throughout follow-up as visually represented in Figure 2.

Competing risk analysis with mortality, endocarditis, and severe SVD as competing risks for healthy survival.

Transprosthetic gradients during follow-up.
Univariate and multivariate cox analysis of determinants for severe SVD.

BSA: body surface area; NYHA: New York Heart Association; EuroSCORE: European System for Cardiac Operative Risk Evaluation; EOA: effective orifice area; iEOA: indexed effective orifice area; PPM: patient prosthesis mismatch.
From this study population, 10 patients required ViV TAVR procedures as treatment for a degenerated sutureless valve, with a mean time to ViV TAVR of 5.4 ± 1.2 years. The experience of ViV TAVR in sutureless valves and discussion of the first 9 patients at our center is reported by Dubois et al. 12
Discussion
The already established main benefits of Perceval™ are the short procedure times and the minimal manipulation of the aorta, providing low early mortality rates in a more complex patient cohort. It lends itself well to adapt minimally invasive techniques and it also offers a way to limit procedure time in multiple or complex procedures. During the study period, the field of AVR and its guidelines have changed, but it is important to highlight that in Belgium, the number of reimbursed TAVR procedures was quite limited, with a slight increase in May 2023. Although the guidelines were updated in 2021, current policy at our center still prioritizes TAVR for the most frail and high-risk patients and thus age—particularly being over 75 years—does not automatically make a patient eligible for TAVR. At our center, the proven stability of sutureless AVR outcomes is well acknowledged by cardiologists and is an integral part of the Heart Team's decision-making process.
Notwithstanding, when first introduced the Perceval™ has shown poor results in terms of postoperative PPI need (with occasionally also high gradients), caused by manifest oversizing. 13 This issue has since been addressed and the pacemaker rate decreased significantly throughout time due to the changes in sizing shift, and simultaneously improving transprosthetic gradients.8,14 Besides the importance of proper sizing, an issue remains with the XL valve size, which is a known independent predictor for PPI. To address this issue, the Perceval™ Plus XL size has been redesigned, specifically by reducing the protrusion of the sub-annular valve collar in an effort to lower the incidence of PPI further. Similar to the preliminary results of the MANTRA study, 15 we saw improved results in the pacemaker implantation rate after XL implantation decreased from 12.8% prior to the Perceval™ Plus to only 4.0% in our study population. Nevertheless, the pacemaker implantation rate after sutureless AVR remains higher compared to conventional stented AVR, as shown by Lorusso et al. 16 However, several studies have been unable to show a significant difference in midterm clinical adverse outcomes in patients with postoperative PPI.17,18 Another study from Vogt et al reported decreasing rates of pacemaker dependency after SU-AVR requiring PPI. 19 More recent data regarding SU-AVR, implementing both the new sizing technique and Perceval™ Plus showed a PPI rate of 4.0%, similar to the reported PPI rate after conventional stented AVR.15,20,21
Additionally, attention should be paid to PPM as it is associated with worse early-, mid-, and long-term outcomes.22,23 In our study population, moderate and severe PPM occurred in 24.6% and 12.3%, respectively, based on the measured EOA at discharge. Similar to the PPI rate, the total PPM rates have decreased from 50.1% to 32.2% due to the updated sizing technique. The total PPM rate in the subpopulation treated with Perceval™ Plus was 22.1%. However, further efforts to decrease the PPM rate are warranted to limit the negative impact on outcome and limit the risk of PPM after ViV TAVR.24,25 Valve durability is crucial information for both surgeons and patients when making informed treatment choices. Structural valve deterioration is a multifactorial process, leading to calcification and leaflet damage, which can cause valve stenosis or leaflet tears resulting in regurgitation. Bioprosthetic valves made from bovine pericardium are more prone to stenosis-based SVD. 26 Different valve designs and material treatments impact durability and hemodynamic profiles, with increased flow potentially causing early degeneration.27,28 Although PPM is an established a strong independent predictor of SVD due to structural degeneration and higher gradients, our study did not show this correlation in a Cox regression. 29 As for endocarditis, in our cohort we saw an endocarditis rate of 0.50% PPY, similar to endocarditis rates reported on other bioprosthetic valves.7,30
Although reintervention rates are low, another important benefit is that Perceval™ is well suited to perform ViV TAVR procedures as its leaflets avoid the sinotubular junction when open, preventing sinus blockage and maintaining coronary patency and access. Thus, Perceval™ serves as an ideal docking station for transcatheter valves in cases of SVD. 12
Limitations
The preliminary limitation of this study is its retrospective design. Nevertheless, this patient population represents a diverse range of procedures, not confined to elective cases, providing a reasonably accurate reflection of a real-world setting. Additional limitations include the lack of a control group, such as patients undergoing AVR with conventional bioprosthetic valves or TAVR, and the absence of established criteria for valve failure (eg, VARC-2 criteria for SVD, non-SVD, endocarditis, and thrombosis). The long-term adverse events such as reintervention rate can also potentially be influenced by older age of the study population and lower rate of survival at 10 years. The follow-up period for most patients remains limited, though it is expected to extend in the coming years and will be crucial for obtaining more robust evidence.
Conclusion
In this large cohort study, we observed low rates of 30-day mortality, stroke, and reoperation for bleeding in combination with a good hemodynamic performance and an improving pacemaker rate. Long-term results show stable results with low rates of endocarditis, severe SVD, and reinterventions. Additionally, sutureless AVR can be used in various settings, as it is suitable for both minimally invasive single AVR and as an option to limit procedure time during more difficult combined and redo procedures.
Footnotes
Abbreviations
Author contributions
BM, PV, CD, and ML contributed to the study. ML, BS, and DS gathered and processed experimental data. ML performed the analysis, drafted the manuscript, and designed the figures. All authors discussed the results and commented on the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ML is a PhD student funded by a research grant from Corcym. FR, PV, and BM are consultants to Corcym. CD receives speaker fees from Corcym. All other authors have declared no conflicts of interest.
Data availability
The data that support the findings of this study are available upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.