
Abstract
Objective
Animal models are indispensable for the development of valve prostheses like we currently know them. Recent developments have questioned the validity of sheep as the model of choice for the evaluation of mechanical heart valves. The pig has been raised as a better alternative due to a more comparable coagulation system. We therefore compared the thrombogenicity of the sheep compared to the pig in a model of pulmonary valve replacement.
Methods
Pigs (n = 12) and sheep (n = 5) underwent pulmonary valve replacement with a mechanical valve in orthotopic position. No antithrombotic medication of any kind was given. Follow-up period was 5 months or until established valve thrombosis. Valve performance was assessed by monthly cardiac ultrasounds combined with post-mortem macro- and microscopical analysis of the valve and downstream organs.
Results
In the pig cohort, valve thrombosis was established after less than a month in all but one animal. Post-mortem valve examination showed terminal valve thrombosis with immobilized hinges. In the sheep cohort, all animals completed the follow-up period of 5 months. At post-mortem examination, all valves were free from any thrombi or deposits with both leaflets mobile.
Conclusion
The sheep model appears not thrombogenic enough to elicit mechanical valve thrombosis in the highly thrombogenic pulmonary position. Contrarily, the porcine model elicits massive thrombosis at a fast rate in an identical position. These findings confirm that we should shift to the pig as a standard for (mechanical valve) thrombosis research.
This is a visual representation of the abstract.
Introduction
In the world of prosthetic heart valves, animal models have been indispensable for pre-clinical valve development and testing before human use. While many advancements have been made, there is still research needed to bridge the gap between currently used valves and the ideal valve prosthesis. An ideal valve prosthesis would be durable, allow normal physiological hemodynamic flow with minimal regurgitation, show no signs of thrombogenicity or damage to blood elements and allow easy implantation. 1 Two large groups of prosthetic valves have been developed. Bioprosthetic valves are made of biologic material and mechanical valves that are made of non-biological material such as pyrolytic carbon (PYC) or polyether ether ketone (PEEK).
Sheep have traditionally been the preferred animal model for valve research due to their anatomical similarity to humans, docile nature, and widespread availability. However, concerns arose when the Medtronic Parallel valve showed high thrombosis rates in humans, despite positive preclinical results in sheep. 2 Further research revealed that sheep platelets have lower activity compared to humans, making them less ideal for studying blood clot formation.3–6 Pigs, on the other hand, may offer a better model for thrombosis research because their platelet behavior and coagulation systems are more similar to humans.5,7,8 Pig platelets tend to behave more like human platelets, spreading effectively on pyrolytic carbon, the material commonly used in mechanical valves. 4 This may make pigs better suited for studying thrombosis in mechanical valves. Additionally, pigs may even exhibit a hypercoagulable state, further aligning them with human thrombotic responses.9,10
Another key factor in animal model design is valve placement. Orthotopic placement, in the native valve position, allows for physiological flow and normal valve function but requires cardiopulmonary bypass (CPB), raising costs and risks. A heterotopic model of valve replacement, developed by McKellar, incorporates the valve in a bypass circuit in the descending aorta, reducing costs and complications by avoiding CPB. 11 It offers better survival rates but lacks normal flow, impairing normal valve movement as there is laminar instead of pulsatile flow over the valve. While the heterotopic model is ideal for testing non-warfarin anticoagulants, orthotopic placement is essential for evaluating new valve designs and materials due to the importance of normal valve function allowing washout of the hinge regions and struts. When considering orthotopic valve placement, the aortic and mitral valves are the most commonly replaced in humans. However, using the aortic position in pigs is challenging due to the fragility of their aortic wall and notorious rhythm restoration problems, leading to high mortality. The mitral position also poses difficulties, with studies showing variable survival rates and complications like mitral valve thrombosis, resulting in pulmonary edema and early euthanasia in non-anticoagulated pigs.12,13 Pulmonary position offers an interesting alternative, as it can be done without cardioplegia, reducing risks and complications. Although pulmonary valve replacement with a mechanical valve is known to cause thrombotic changes, normal valve movement is generally preserved allowing for fair comparison.14,15
The main objective of this study was to compare the thrombogenic response of sheep and pigs to a mechanical valve implanted in pulmonary position, in order to develop a better animal model for mechanical valve thrombosis.
Materials and methods
Ethics statement
This study was approved by the Animal Ethics Committee of the University of Leuven (P119/2021).
Study design
A total of 17 animals (12 neutered Landrace×Large White pigs (4 months of age, 38.5 ± 6.7 kg) and 5 female adult Swifter sheep, 73.6 ± 4.5 kg) were acquired from the ZOOtechnical center (ZTC, Lovenjoel, Belgium) and cared for at the animal care facility of University of Leuven under supervision by a veterinarian in accordance with the ‘Guide for the care and use of laboratory animals, eighth Edition’, formulated by the National Research Council. 16 All animals were housed for a minimum of one week before valve implantation. The follow-up period was 5 months or until valve failure due to thrombosis or other reasons was established. Valve failure was defined as total absence of any valve movement on cardiac ultrasound. Follow-up consisted of serial blood samples combined with monthly cardiac ultrasounds (see Figure 1). In the pig cohort, follow-up was intensified after the first 3 animals to every 2 weeks to capture valve failure earlier. Cardiac ultrasound was performed using a GE Healthcare Vivid E9 with an M5S probe. All valves used were 21 mm bileaflet mechanical valves. In the pig cohort, 6 animals received St. Jude Medical® Mechanical Heart Valve (SJM; St. Jude Medical Inc.; Minneapolis, Minn), 3 On-X mechanical heart valve (CryoLife and BicarbonVR, LivaNova) and 3 Carbomedics Top Hat (CM; Sulzer, Carbomedics, Austin, TX). In the sheep cohort, 2 animals received the St. Jude Medical® Mechanical Heart Valve (SJM; St. Jude Medical Inc.; Minneapolis, Minn) and 3 animals received the On-X (On-X, CryoLife and BicarbonVR, LivaNova). Experiments were performed from March 2021 until August 2022. Follow-up of the last animal was completed in October 2022.

Study groups and flowchart.
Surgery
Sheep cohort
Sheep were fasted 24 h prior to surgery. Sheep were sedated using ketamine by jugular venous injection. Arterial pressure line was inserted in the right ear and venous access line was inserted in left upper leg. Anaesthesia was induced and maintained by intravenous propofol. Positive pressure ventilation was started after intubation. A large bore gastric tube for gastric decompression was placed. Antibiotic prophylaxis by ceftiofur was given. Animals were positioned in right lateral recumbent position followed by surgical scrubbing and draping to expose the left cervical region and left chest wall.
A left anterolateral thoracotomy was made in the third intercostal space. Lidocaine was given for arrhytmia prevention. The pericardium was incised anteroposteriorly and cradled by single sutures. Care was made to spare the phrenic nerve. Normothermic CPB was established by cannulation of the left carotid artery (Medtronic EOPA arterial cannula, 18F, vented) and jugular vein (Medtronic Bio-Medicus One-Piece Femoral Venous Cannula 27F×30”, Non-Vented 1/2”) after heparinization (heparin sodium, 250 IU/kg bodyweight; Rhone-Poulenc Rorer,Brussels, Belgium). A target ACT of 350 s was reached and maintained.
The distal pulmonary artery was clamped once sufficient venous drainage was achieved. The pulmonary trunk was opened at the level of the sino-tubular junction. Supplementary venous drainage was achieved by inserting a sump catheter in the right ventricle trough the pulmonary valve ensuring a dry working field. The native valve was excised and a 21 mm mechanical heart Valve was implanted orthotopically. The pulmonary trunk was closed with a single running suture after properly de-airing. The sheep were decannulated once adequate weaning of CPB was achieved. The pericardium was left open and the chest closed in standard fashion with resorbable sutures. One pleural drain was placed. The jugular incision was closed in layers with resorbable sutures.
Pig Cohort
Pigs were fasted 24 h prior to surgery. Pigs were sedated using intramuscular midazolam and xylazine. Arterial pressure line was inserted in the right ear and venous access line was inserted in the left upper leg. Mechanical ventilation was started after intubation and ceftiofur antibiotic prophylaxis was given according to animal weight. Animals were surgically scrubbed in right lateral recumbent position and surgically draped.
A left anterolateral thoracotomy was made in the third intercostal space. Lidocaine was given to prevent ventricular arrhythmias. The pericardium was incised in a T-shaped fashion directly over the main pulmonary artery and the heart was suspended in a pericardial cradle. After dissection of the aortopulmonary window and heparinization (300 IU/kg, target activating clotting time (ACT) > 500), normothermic CPB was established by cannulating the ascending aorta (Medtronic DLP arterial cannula, vented, 14F) and right atrial appendage (Medtronic DLP single stage venous cannula, angled 28F). As the aortic wall in pigs is fragile, double polypropylene 5–0 purse string sutures reinforced with ericardium pledges were used.
Once sufficient venous drainage was confirmed, the distal pulmonary artery was clamped. The pulmonary artery was opened anteriorly at the level of the sinotubular junction. A suction catheter in the right ventricle (via the incised pulmonary artery) enabled a dry working field. A 21-mm mechanical heart valve was implanted in orthotopic position after excising the native pulmonary valve leaflets. Position and function were verified thoroughly prior to de-airing and closure of the pulmonary artery. The pig was weaned from CPB and once haemodynamic parameters are stable, the heart-lung machine was stopped and cannulas removed. The pericardium was left open and the chest closed in a standard fashion over one pleural drain.
Postoperative care
The chest drain was removed about 1–2 h after surgery, when sedation was fading and the animal was breathing adequately. Feeding was allowed immediately. Adequate analgesia (sheep: piritramide, pigs: meloxicam and buprenorphine), diuretics (pigs and sheep: furosemide) and antibiotics (sheep: ampicillin, pigs: ceftiofur) were given during the first 2 postoperative days. During the first postoperative week, low molecular-weight heparin (pigs and sheep: enoxaparin 20 mg twice daily) was administered by subcutaneous injection. At the end of the first week, all medication and anticoagulation was stopped. Animals were sedated during the cardiac ultrasounds. Indices taken were valve area (cm²), cardiac output (L/min), peak and mean gradient (mm Hg) and valve insufficiency. Cardiac ultrasounds were performed by a cardiologist blinded to the implanted valve type.
Explant procedures
At valve thrombosis (total absence of any valve movement on cardiac ultrasound) or follow-up completion, animals were euthanized with pentobarbital after heparinization (heparin 300IU/kg) to prevent post-mortem thrombosis. A cardiectomy was performed. The valves were carefully dissected form the surrounding tissue and assessed for evidence of structural degradation, thrombus (weight), vegetation, pannus overgrowth, hinge integrity and paravalvular leak. The lungs, as the first downstream capillary bed, were macroscopically evaluated and random lung biopsies were taken to screen for thrombo-embolism.
Data analysis
Baseline study population characteristics by animal cohort were described using mean and standard deviation. Univariable analysis were unpaired student T-tests for normally distributed variables and Mann-Whitney U tests for not normally distributed variables. A significance level of p < 0.05 was used. All tests were 2-sided. Software used was GraphPad Prism 10.0.2 (Dotmatics, MA, USA).
Results
Perioperative outcomes and valve patency
At the time of surgery, the pig is less heavy than the sheep. The pig breed used (Landrace×Large White) grows at an average of 5–10 kg/week. Juvenile pigs (40 kg) are used to account for the weight and size increase during follow-up. The sheep used are at adult weight, no size or weight increase is expected during follow-up (see Supplementary file 1).
All animals in both groups survived the immediate perioperative period (see Table 1). The operating and CPB-times are comparable in both groups (see Figure 2A). In the pig cohort, dissection of the aortopulmonary window is required for proper exposure of the underlying ascending aorta. Two purse strings reinforced with pericardial pledged are needed, as it is known that the aortic wall of these juvenile pigs is rather fragile. This is not needed in the sheep cohort, as the neck vessels are ideal for proper and easy cannulation. Overall, both procedures can happen in less than 2 h, making this a fairly fast and straightforward experiment.

A. Procedure time. B: Probability of valve patency. CPB: cardiopulmonary bypass. OR: operating time.
Perioperative parameters of both sheep and pig cohort.

All sheep completed the follow-up period of 5 months. Contrarily, most pigs showed at their first cardiac ultrasound severe valve dysfunction due to thrombosis leading to their premature sacrifice. This difference was statistically significant (see Figure 2B).
Cardiac ultrasound
In the pig cohort, severe gradients were noted almost immediately at the first operative control (see Table 2). For most animals, terminal valve thrombosis was established after as few as 2 weeks. High gradients combined with immobile leaflets and absent valve clicks on cardiac ultrasound confirmed terminal valve thrombosis. There was right ventricle septal flattening, indicating pressure overload. The massively dilated right ventricle compromised normal functioning of the left ventricle. Valve thrombosis was usually combined with severe insufficiency, as the leaflets are usually fixed in the (partially) open position. 9 pigs were sacrificed immediately after the first ultrasound. 2 pigs had 2 ultrasounds before their sacrifice right after: pig#5 was sacrificed at 36 days and pig#11 at 24 days. Only pig#12 survived until almost 2 months, however with high gradients and insufficiency from the beginning.
Cardiac ultrasound parameters.

POD: Post Operative Day, VA: Valve Area, CO: Cardiac Output, MG: Mean Gradient, PG: Peak Gradient, PI: Pulmonary Insufficiency. SJM: Saint-Jude Medical. CM: Carbomedics Top hat.
In the sheep cohort, all sheep survived until study completion (see Table 3). Sheep #1 showed no abnormalities at the first cardiac ultrasound. Both leaflets were mobile and valve gradients were low. At 2 months, the valve had increased gradients with suspicion of one immobile leaflet. The final cardiac ultrasound at 4 months showed slightly better gradients, however still elevated. Insufficiency was stable at 2/4 during follow-up. The 4 other sheep had consistently normal monthly check-ups. Gradients remained low, good excursion of both leaflets combined with the absence of any insufficiency indicated normal valve functioning.
Cardiac ultrasound parameters.

POD: Post Operative Day, VA: Valve Area, CO: Cardiac Output, MG: Mean Gradient, PG: Peak Gradient, PI: Pulmonary Insufficiency. SJM: Saint-Jude Medical.
Cardiac Ultrasound Parameters Combined.
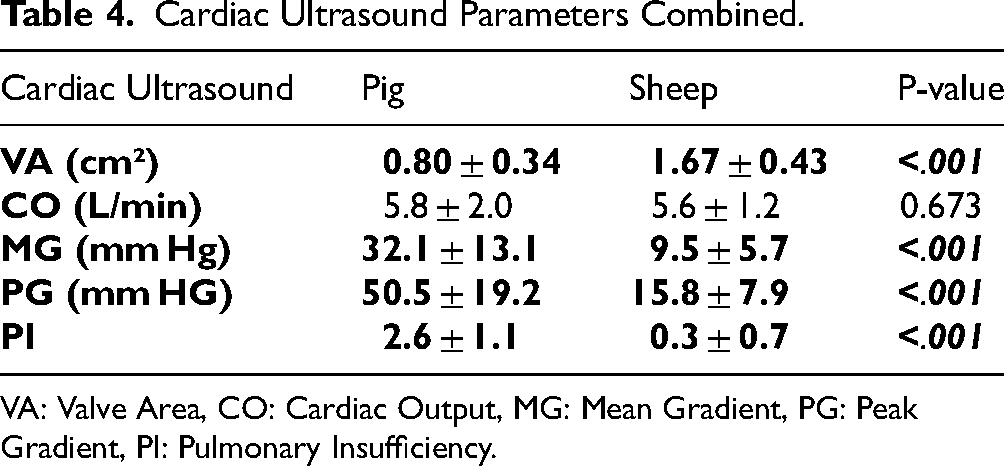
VA: Valve Area, CO: Cardiac Output, MG: Mean Gradient, PG: Peak Gradient, PI: Pulmonary Insufficiency.
Valve area, mean gradient, peak gradient and (pulmonary) valve insufficiency were significantly better for the sheep cohort (see Table 4 and Figure 3). It is important to note that the cardiac output does not differ. This is of importance, due to the fact that a difference in cardiac output may exaggerate or blur cardiac ultrasound parameters. The significant difference in valve area indicates terminal valve thrombosis, which is also clearly visible from the higher mean and peak gradients. Contrarily, all sheep have valve areas and gradients comparable to normal clinical values.17,18

Cardiac ultrasound parameters.
Macroscopic evaluation at autopsy
A formal necropsy was performed in all animals. There were no macroscopic signs of pulmonary embolism nor were there any signs of bleeding.
In the pig cohort, the valves showed complete thrombosis of the hinges blocking leaflet movement (see Figure 4). All valves were fixed in the partially open position. Most valves had thrombus formation in the hinges, obstructing leaflet movement. In some animals, the thrombus on the hinges went over in a pannus partially overriding the valve housing. In all explanted valves, leaflets could not be mobilized by forceps manipulation.

Representative images of three different explanted bileaflet valves in the pig cohort.A, B: Saint-Jude Medical. C, D: Carbomedics Top Hat. E, F: On-X.
In the sheep cohort (see Figure 5), sheep #1 had small thrombi around one hinge. Despite being small, their strategic location inside or near the hinge explained the increased gradient and insufficiency of the valve in this animal. One immobile leaflet was also confirmed on cardia ultrasound. All 4 other sheep had a perfectly clear valve free of any deposits. The hinges were mobile, falling open when turning the valve upside down. This correlates with the consistently low gradients seen in these animals.

Representative images of explanted bileaflet valves in the sheep cohort. A, B: Saint-Jude Medical. C, D: On-X.
Histological evaluation
In both groups, random biopsies of the lungs were absent of microscopic signs of thrombo-embolic disease. The thrombi showed no signs of inflammation or infection. In conclusion, there were no histological particularities. When compared to human valve thrombi, no difference was found. 19
Blood results
Laboratory values were absent for ongoing infection or signs of hemolysis due to valve implantation. No other observable effects of valve implantation could be found. Blood values can be found in Supplementary file 1.
Discussion
Valve implantation in chronic, large animal models is indispensable for the preclinical evaluation of new heart valve prostheses. A good animal model studying mechanical valve thrombosis is needed. With this paper, we aimed to elaborate and refine the porcine model of pulmonary valve replacement as the new reference model for mechanical valve thrombosis.
As stated before, this model has several key advantages. Firstly, pigs are widely available. They can be bought from vendors practically everywhere at low cost. Secondly, pulmonary valve replacement is a fairly straightforward procedure with low surgical risk. The point of highest surgical risk is the cannulation of the fragile aortic wall. We strengthened our sutures with small pledges of pericardium. This is sufficient to avoid tearing out the suture. Another technical advantage of this model is the absent need for cardioplegia which obsoletes weaning difficulties and rhythm restoration, which are notorious in pigs. Adequate venous drainage can be achieved by properly positioning the venous cannula in the right atrium. If venous drainage is inadequate, repositioning of the cannula or placement of an extra sump catheter in the right ventricle via the incised pulmonary trunk suffices to continue the surgery. Thirdly, this model produces thrombosis that is similar in size and position to valve thrombosis seen in humans. 19 The thrombus is located at the hinges and the pannus is minimal to absent, making the results of this model clinically comparable. Fourthly, fully thrombosed valves in pulmonary position are well tolerated. We did not experience any clear negative consequences impeding completion of follow-up or impacting general animal well-being, in contrary to the mitral positioning with the risk of pulmonary oedema or aortic positioning with its inherent surgical risks. Lastly, as histological analysis needs evaluate the first capillary bed for micro thromboembolism, only the lungs need to be evaluated in pulmonary position contrarily to mitral or aorta, where all downstream organs (brain, liver, adrenal etc) need to microscopically evaluated. This greatly reduces workload and study cost.
It is to be noted that pigs grow considerably faster than the adult sheep. The Landrace×Large White pig strain used in this study gain an average of 5–10 kg body weight weekly, in stark contrast with the steady weight of the adult sheep. The 21 mm valve at the time of surgery is oversized, however this oversizing is needed to account for the additional growth of the animal. While it poses a technical difficulty to descend the oversized valve in the pulmonary root, it is possible.
The cardiac ultrasound results are striking. Terminal valve thrombosis is evident at the first cardiac ultrasound in the pig cohort, compared to the normal valve functioning in the sheep cohort even at 120 days postoperatively without any coagulation. These findings confirm the low thrombogenicity of the sheep, obsoleting their relevance for thrombosis research.
Conclusion
This study aimed to confirm the limitations of the sheep model and proposes a valid alternative. For testing mechanical valve thrombogenicity, pulmonary valve replacement in a pig seems a good model to base future mechanical valve thrombosis research for better and translational results. Future mechanical valve research at our center will be based on this model, results are to be expected shortly.
Limitations
The main limitation of this study is the small sample size. It is known that animal experiments are costly and cumbersome. Since this is merely a proof-of-concept study, we opted to keep the numbers small and manageable. Earlier first time echocardiography at 2 weeks postoperatively and longer follow-up should elude the survival difference. Another limitation of this study is valve implantation in pulmonary position, while it intended use is mitral or aortic. As stated before, pulmonary position was chosen as it is a highly thrombogenic position and obsoletes the need for cardioplegic arrest during valve implantation. Future research at our department aims to compare thrombogenicity of mitral, aortic and pulmonary position in the porcine heart.
Supplemental Material
sj-docx-1-hvs-10.1177_30494826241297123 - Supplemental material for Development of an orthotopic pulmonary valve replacement porcine model for mechanical heart valve thrombosis
Supplemental material, sj-docx-1-hvs-10.1177_30494826241297123 for Development of an orthotopic pulmonary valve replacement porcine model for mechanical heart valve thrombosis by Tom Langenaeken, Manon Van Hecke, Pieter De Meester, Jean Roets, Arthur Meuris, Peter Verbrugghe, Filip Rega and Bart Meuris in Journal of the Heart Valve Society
Supplemental Material
sj-pptx-2-hvs-10.1177_30494826241297123 - Supplemental material for Development of an orthotopic pulmonary valve replacement porcine model for mechanical heart valve thrombosis
Supplemental material, sj-pptx-2-hvs-10.1177_30494826241297123 for Development of an orthotopic pulmonary valve replacement porcine model for mechanical heart valve thrombosis by Tom Langenaeken, Manon Van Hecke, Pieter De Meester, Jean Roets, Arthur Meuris, Peter Verbrugghe, Filip Rega and Bart Meuris in Journal of the Heart Valve Society
Footnotes
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tom Langenaeken is a PhD researcher from the University of Leuven supported by the Experimental Research Fund Cardiovascular Surgery. No external funds were received for the conduction of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data underlying this article will be shared upon reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.