
Abstract
Objectives:
This study sought to assess the current state of healthcare supply chain practices and discern the influencing factors from the perspective of healthcare professionals in the West Gojjam Zone, Ethiopia.
Methodology:
This research employed a cross-sectional study design, complemented by qualitative study. Data gathering encompassed self-administered surveys and in-depth face-to-face interviews conducted between 30 April and 30 June 2020. Epi-Data facilitated data entry, while SPSS version 20 conducted subsequent analysis. Multiple linear regression was executed, deeming variables with a p-value less than 0.05 as indicative of a significant association. Thematic analysis was applied to analyze the qualitative data.
Result:
A total of 425 questionnaires were disseminated, with 413 (97.2%) effectively completed and returned. Procurement, after-procurement service, and monitoring and evaluation emerged as areas with suboptimal performance, registering mean values of 2.85, 2.24, and 1.86, respectively. In contrast, storage practices demonstrated relatively superior performance, with a mean value of 3.34. Multiple linear regression analyses unveiled significant correlations between various practices and factors such as training frequency, proficiency of staff in Integrated Pharmaceutical Logistics System (IPLS), managerial support, and proximity to Pharmaceutical Fund and Supply Agency (PFSA). Moreover, impediments to supply chain practices were identified, encompassing limited medication availability at PFSA, budget constraints, tardy reimbursement by the Health Insurance Agency, and a dearth of technicians adept in medical equipment maintenance.
Conclusion:
The implementation status of healthcare supply chain practices within public health facilities was discerned to be inadequate, with several impediments hindering their effective execution.
Plain Language Summary
Why was the study done? This study aimed to assess the status of healthcare supply chain practices and the factors influencing them in public health facilities in the West Gojjam Zone, Ethiopia. It sought to understand how well these practices were being implemented and identify the challenges faced by healthcare professionals in managing the supply chain. What did the researchers do? Researchers conducted a study using surveys and interviews with healthcare professionals in the West Gojjam Zone of Ethiopia between 30 April and 30 June 2020. They analyzed the collected data to evaluate various aspects of the healthcare supply chain, including procurement, storage practices, after-procurement service, monitoring, and evaluation. What did the researchers find? Out of 425 distributed questionnaires, 413 were completed and returned. The findings revealed that certain areas of the supply chain, such as procurement and after-procurement service, were not performing well. However, storage practices showed relatively better performance. Factors like staff training, proficiency in pharmaceutical logistics systems, managerial support, and proximity to their suppliers were found to significantly impact the status of these practices. What do the findings mean? The study indicates that healthcare supply chain practices in public health facilities in the West Gojjam Zone of Ethiopia are facing implementation challenges. Issues such as inadequate medication availability at the Pharmaceutical Fund and Supply Agency, budget constraints, slow reimbursements from the Health Insurance Agency, and a shortage of skilled technicians for equipment maintenance were identified as obstacles. These findings underscore the urgent need to address these challenges to improve the efficiency and effectiveness of healthcare supply chain management in the region.
Key points
Poor Implementation Prevails: the study reveals a predominant issue of poor implementation in healthcare supply chain practices within public health facilities.
Numerous Challenges Identified: multiple challenges hinder the achievement of effective healthcare supply chain practices, emphasizing the complexity of the issues that need to be addressed.
Call for Action: the findings underscore the urgency for addressing the identified challenges to pave the way for the successful implementation of healthcare supply chain practices in public health facilities.
Introduction
The Council of Logistics Management delineates supply chain management (SCM) as the systematic and strategic synchronization of conventional business functions within an entity and spanning multiple enterprises. This orchestrated alignment is designed to enhance the enduring efficiency of both the singular organization and the comprehensive supply chain (SC).1 –3 The foundation of the healthcare system relies heavily on effective SCM, as the provision of healthcare services is intricately tied to the timely accessibility of pharmaceuticals and other essential medical supplies in appropriate quantities for patient treatment.4,5
Healthcare SCM involves implementing a set of strategies aimed at connecting pharmaceuticals, equipment, suppliers, healthcare institutions, and transportation systems. The overarching goal is to efficiently use resources and attain thorough quality management within healthcare facilities.6,7 In healthcare service providers, SCM frequently entails the coordination of information, supplies, and finances to procure and transport products and services from suppliers to end-users. This process seeks to improve clinical outcomes while simultaneously managing costs.5,7,8
SC practices comprise a diverse set of activities conducted by an organization to facilitate the efficient administration of its SC.3,9,10 The ultimate goal of every SC practice in healthcare facilities is to ensure commodity security for every customer. When healthcare facilities successfully achieve commodity security, individuals gain heightened confidence in the health program, consequently motivating them to actively pursue and utilize essential healthcare services.10,11 Several key SC practices within healthcare facilities play a substantial role in shaping the quality of healthcare services. These practices encompass the formulation of specifications and standards, procurement, post-procurement services, along monitoring and evaluation. 12
As per the evaluation carried out in Tanzania, merely 22% of the facilities possessed procurement plans. 13 Findings from a study in Ghana revealed a persistent inadequacy in the availability of drugs and other supplies in health facilities, consistently remaining below 60% throughout the years. In addition, approximately 15% of reported deaths were linked to shortages of essential medicines. 14 Results from a survey undertaken in Ethiopia indicated that, on average, 63% of health centers and 43% of hospitals maintained satisfactory conditions for storing medicines. 15 A study conducted in Addis Ababa highlighted a suboptimal quality of pharmacy services within hospitals, attributed to the inadequate availability of essential healthcare supplies. 16 In another study within the Amhara Regional State, it was observed that only 47.4% of health facilities received the complete quantity of requested products from Pharmaceutical Fund and Supply Agency (PFSA). Consequently, these facilities encountered recurrent shortages of pharmaceutical products. 17
Evaluating diverse aspects of healthcare SC practices is essential for achieving ongoing service enhancement, meeting the needs of all stakeholders, and optimizing clinical outcomes to the fullest extent. 18 Hence, the objective of this study was to evaluate the status of healthcare SC practices and the factors associated with them from a healthcare professional perspective in West Gojjam Zone. In addition, the study aims to investigate the challenges associated with these practices. The findings of this study are anticipated to offer valuable insights into the present landscape of healthcare SC practices, serving as a cornerstone for subsequent research in this domain.
Material and methods
Study setting and period
The study was conducted in the West Gojjam Zone, which is one of the most densely populated zones in the Amhara Regional State, Ethiopia. Within this zone, there were a total of 94 health centers and 6 primary hospitals. The total number of healthcare professionals employed across all public health facilities in the West Gojjam Zone was 2774. The data collection period spanned from 30 April 2020 to 30 June 2020.
Study design
The study employed a cross-sectional mixed-method approach, combining quantitative surveys and qualitative interviews, to comprehensively assess healthcare SC practices. Quantitative surveys gathered structured data on various aspects of healthcare SC practices, while qualitative interviews provided depth and context to participants’ perspectives. Integration of these methods allowed for a nuanced understanding of factors influencing healthcare SC practices. In addition, in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement guideline, our study methodology adheres to established reporting standards (Supplementary File 2).
Source and study population
The source population for this study encompassed all health facilities and healthcare professionals within the designated area. The study population, however, was delimited to specific public health facilities and the corresponding healthcare professionals entrusted with diverse responsibilities pertaining to the SC.
Inclusion and exclusion criteria
This study incorporated health facilities with a minimum of 6 months of operational history proceeding the data collection period. It also encompassed healthcare professionals holding membership in the Drug and Therapeutics Committee (DTC) and those serving as heads of respective dispensing units. On the contrary, military health facilities and personnel who commenced their roles within the 6 months leading up to the data collection period were excluded from the study.
Sample size determination
According to the Logistics Indicators Assessment Tool (LIAT) by the United States Agency for International Development (USAID) Delivery Project, it is recommended to include a minimum of 15% of health facilities for sample size determination in the study area. 19 However, in our study, we opted to encompass all hospitals and 50% of the health centers, resulting in the inclusion of 47 out of the total 94 health centers in the area. Consequently, the initial stage of the sampling process involved the selection of 53 health facilities, comprising 6 hospitals and 47 health centers.
In the subsequent stage, the Single Population Proportion Formula was applied to calculate the required number of healthcare professionals for the sample. This computation took into account a 0.5 p-value, a 95% confidence interval, a 5% margin of error, a 10% non-response rate, and a 1.2 design effect. The initially calculated sample size was 506 healthcare professionals. However, as the proportion relative to the total population exceeded 5%, the Finite Population Formula was utilized, yielding a final calculated sample size of 425 healthcare professionals for quantitative data collection. To ensure representation from each chosen public health facility, we proportionally allocated the number of professionals selected based on the total staff count in each facility.
For qualitative data, in-depth face-to-face interviews were conducted with 27 key informants, specifically the pharmacy head and pharmaceutical store manager of each selected public health facility. The interviews continued until a point of information saturation was reached.
Sampling technique
A two-stage simple random sampling technique was employed to choose health facilities and primary respondents, who are healthcare professionals. In this study, the public health facility served as the primary sampling unit, and the individual healthcare professional was the secondary sampling unit. In the initial stage, public health facilities were randomly selected through a lottery method from the sampling frame of available public health facilities. During the subsequent stage of the sampling process, healthcare professionals were chosen through a lottery method from the sampling frame specific to each selected public health facility. The allocation of the number of healthcare professionals included in the sample from each public health facility was conducted proportionally based on the total staff count in each facility (see Supplementary File).
In the qualitative aspect of the study, a purposive sampling technique was applied to select key informants, specifically the pharmacy head and pharmaceutical store manager of health facilities. These individuals were deliberately chosen to gather qualitative data through in-depth face-to-face interviews.
Study variables
The study’s dependent variables encompassed various healthcare SC practices, namely procurement, storage practice, after-procurement service, and monitoring and evaluation. The independent variables encompassed socio-demographic characteristics (such as educational level, years of experience), management-related factors (such as management support, frequency of supportive supervisions, frequency of trainings sessions, and budget allocation), and health facility-related factors (such as service volume level of health facilities, Integrated Pharmaceutical Logistics System (IPLS) skills of staff, number of pharmacy staff, distance from the PFSA, Health Commodities Management Information System (HCMIS) implementation site, and health facility type) (see Figure 1).

Conceptual framework of the study.
Data collection tool and process
Quantitative data regarding the SC practices of health facilities were gathered using a self-administered structured questionnaire. Respondents were required to provide answers to a series of questions formulated on a Likert-type scale with five options: 1 denoting “Strongly Disagree,” 2 indicating “Disagree,” 3 representing “Neutral,” 4 signifying “Agree,” and 5 corresponding to “Strongly Agree.” This scale was used to determine the extent of agreement and disagreement regarding the questions posed to them. The questionnaire demonstrated high internal consistency reliability (Cronbach’s alpha = 0.93), indicating consistent measurement of the underlying construct by its items. In addition, the principal investigator conducted in-depth face-to-face interviews with key informants, utilizing a semi-structured questionnaire to collect qualitative data. The data were collected by pharmacy professionals experienced in health commodity-related SC practices.
Data processing and analysis
Quantitative data were meticulously processed and analyzed using a systematic approach. Prior to entry into the Epi-Data software, a comprehensive check for completeness was conducted, ensuring the integrity of the data set. Missing values were consistently recorded during data entry to denote their absence, and particular attention was given to mitigating any potential impact of these values on the validity of statistical inferences during analysis using the Statistical Package for Social Sciences (SPSS) program, version 20.
Various statistical metrics, including frequency distributions, means, and percentages, were computed to provide a comprehensive overview of the quantitative data. Simple and multiple linear regressions were then employed to establish associations and predict outcomes between selected variables. Variables with simple linear regression p-value < 0.25 were selected for multiple linear regression, which further identified associations and predicted outcomes with significance determined at p < 0.05 within the 95% confidence interval. Regression models for each healthcare SC practice were developed using a backward stepwise model-building technique.
For the qualitative component of the study, a rigorous manual analysis approach was undertaken. Digital files were transcribed meticulously, with each transcription undergoing careful review, read twice while listening to the recording, to ensure accuracy. Thematic content analysis was then applied to the qualitative data, facilitating the identification of recurring themes and patterns within participants’ narratives.
The integration of quantitative and qualitative findings in section “Discussion” facilitated a comprehensive triangulation of results, revealing convergent and divergent insights between the two data sources. This triangulation not only strengthened the validity and reliability of the study findings but also provided a nuanced understanding of the intricate interplay between healthcare SC practices and the factors influencing them.
Data quality management
Data quality was meticulously guaranteed through the careful design and pretesting of questionnaires. A pretest was administered to 5% of the total sample size, involving respondents situated outside the study area. The feedback from this pretest informed appropriate modifications to the questionnaires. Furthermore, the quality of the data was reinforced by systematically categorizing and coding the questionnaires. Data collectors, comprising pharmacy professionals well-versed in health commodities’ SC practices, underwent training to ensure proficiency. In addition, prior to analysis, a comprehensive assessment of completeness was conducted on the filled questionnaires.
Operational definitions
Healthcare SC practices: the practices were deemed as under-performed if their mean value was 3 or less. Conversely, practices were considered better-performed if their mean value exceeded 3.
Training: in this study, a mean value of 2.5 or less is categorized as Low, a mean value greater than 2.5 and less than 4.5 is considered Medium, and a mean value exceeding 4.5 is regarded as High.
Supportive Supervision: in this study, a mean value of 2.5 or less indicates Low support, a mean value greater than 2.5 and less than 4.5 denotes Medium support, and a mean value exceeding 4.5 signifies High support.
Budget Allocation: in this study, a mean value of 2.5 or less signifies a Low budget, a mean value greater than 2.5 and less than 4.5 indicates a Medium budget, and a mean value exceeding 4.5 denotes a High budget.
IPLS Skill of Staff: a mean value of 2.5 or less is classified as Poor, a mean value greater than 2.5 and less than 4.5 is categorized as Good, and a mean value exceeding 4.5 is considered Very Good.
Management Support: a mean value of 2.5 or less indicates Low support, a mean value greater than 2.5 and less than 4.5 denotes Medium support, and a mean value exceeding 4.5 signifies High support.
Health Facility Type: in this study, the healthcare service providers are categorized as health center, primary hospital, general hospital, referral hospital, and specialized hospital.
Health Facility’s Service Volume Level: As per the Federal Ministry of Health (FMOH) of Ethiopia, health centers are classified as follows: Low (daily patient load ⩽ 50), Medium (daily patient load between 50 and 80), and High: if daily patient load ⩾ 80 and meeting any three criteria from the following: designation as ART sites, implementation of more than 5 Dispensing Units (DUs) in IPLS, HCMIS implementation, and at least 3 years since HCMIS implementation. Alternatively, serving more than 50 patients and meeting all four criteria. 20
Ethical clearance
Ethical approval was secured from the Institutional Review Board of Jimma University (IHRPGD197/18). Before initiating data collection, approval for the process was sought from each public health facility. Verbal consent was obtained from all participants, with a guarantee of the confidentiality of their information. Given the minimal risk associated with the study, obtaining verbal informed consent aligns with the National Research Ethical Review Guideline of Ethiopia. 21
Result
The study meticulously examined data from each distinct healthcare SC practice, conducting a thorough analysis to yield precise insights. The outcomes were subsequently visually depicted through charts and tables, complemented by concise explanations. The survey involved the distribution of 425 questionnaires to participants, with a noteworthy 97.2% response rate, attesting to its excellence based on the criteria established by Mugenda. 22
Demographic characteristics of respondents
Characteristics of respondents
A substantial proportion of the survey participants, constituting 261 (63.2%) individuals, possessed a diploma from a college or university, while 147 (35.6%) respondents held a Bachelor’s degree (Figure 2). Among the entire participants, 317 (76.8%) individuals reported having less than 5 years of professional experience, while 94 (22.7%) respondents had a work history spanning from 5 to less than 10 years (Figure 3).

Educational level of respondents who participated in this study.

The work experience of respondents who participated in the study.
Characteristics of studied health facilities
The predominant segment among the health facilities, 46 (88.5%), were identified as health centers, with 61.5% of them not currently employing HCMIS. In addition, 6 (11.5%) of the health facilities were designated as primary hospitals, and notably, all of them were actively implementing HCMIS. In terms of service volume categorization, the distribution was as follows: 20 (38.46%) of health facilities were classified with higher service volumes, 17 (32.69%) with medium service volumes, and 15 (28.85%) with lower service volumes (Table 1).
The percentage of type of health facility included in the study.

HCMIS: Health Commodity Management Information Systems.
Other health facility and management-related factors
The mean values for responses pertaining to the levels of management support, IPLS skill of staff, number of trainings, budget allocation, and the frequency of supportive supervisions were 3.12, 3.31, 3.20, 3.26, and 3.1, respectively. Among the surveyed health facilities, 12 (23%) were located within the range of 150–200 km from PFSA. Following this, 11 (21.1%) of the total were located at a distance between 50 and 100 km from PFSA. The distribution of pharmacy staff in health centers and primary hospitals stood at 96 (53.63%) and 83 (46.37%), respectively (Table 2).
Other health facility and management-related factors in the study.

PFSA: Pharmaceutical Fund and Supply Agency; IPLS: Integrated Pharmaceutical Logistics System.
Healthcare SC practices
A comprehensive assessment encompassed diverse healthcare SC practices, ranging from procurement and storage practices to after-procurement services and monitoring and evaluation.
Status of procurement practice
Twelve questions were asked to assess the status of procurement practice and the majority of the questions had a mean value greater than 3.0. Notably, the question achieving the highest mean value, at 3.62 (with a standard deviation of 0.923), was related to “the development and regular updating of a facility-specific medicine list.” Conversely, the question reflecting the lowest mean value, at 1.72 (with a standard deviation of 0.564), related to “the comprehensiveness and appropriateness of the standards and specifications developed for the current clinical setup” (see Table 3).
Descriptive statistics of procurement practices.
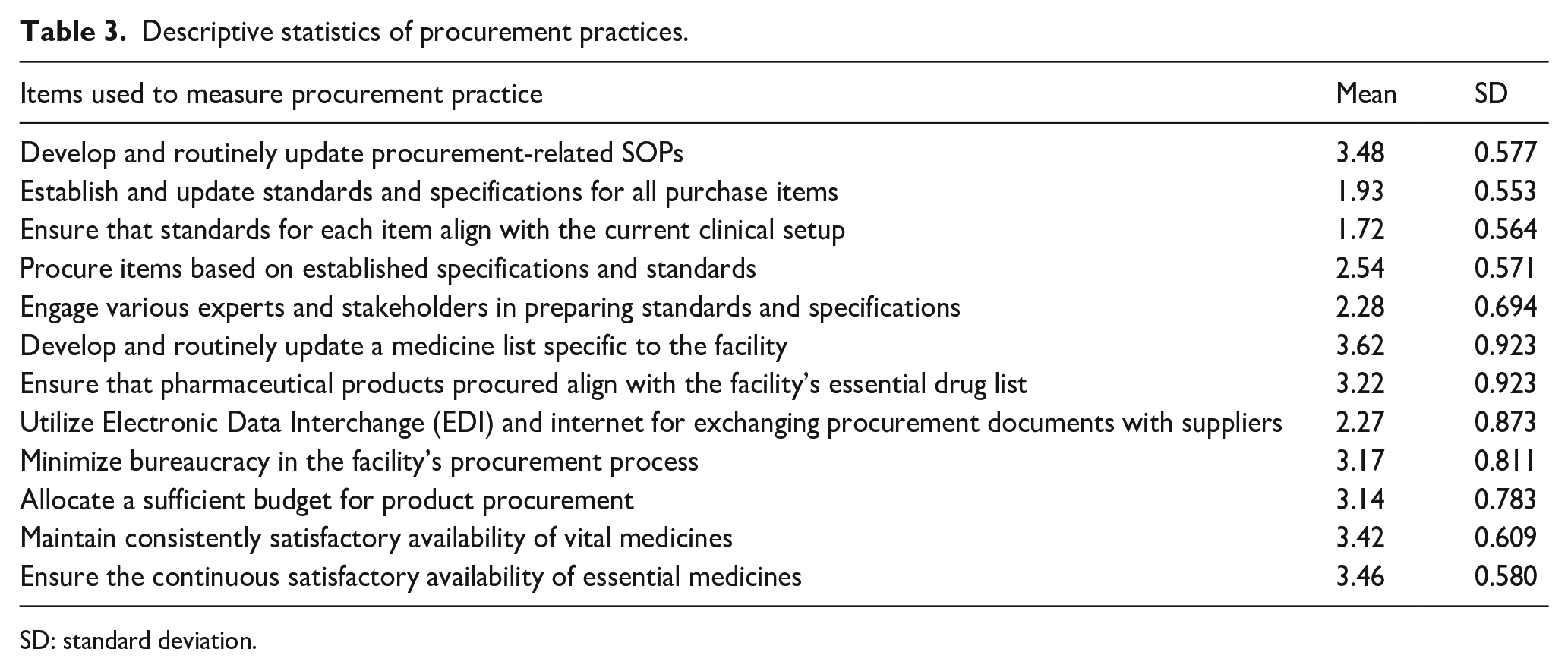
SD: standard deviation.
Determinants of procurement practice
The multiple linear regression analysis elucidated that the coefficient of determination (R 2 ) was 0.53. This denotes that management support, distance from PFSA, number of trainings, service volume level, and budget collectively accounted for 53% of the variability observed in procurement practices. With a p-value of 0.000 (below 0.05), the statistical significance of the procurement practice model is affirmed at a 5% level of significance (see Table 4).
The model summery of regression analysis for procurement practice.
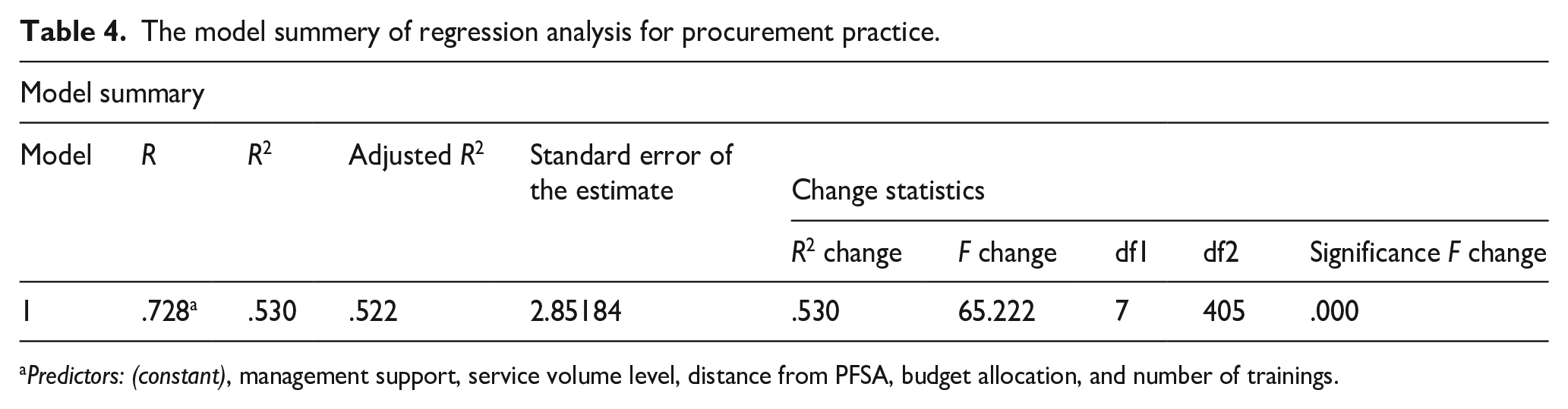
Predictors: (constant), management support, service volume level, distance from PFSA, budget allocation, and number of trainings.
The developed multiple linear regression model for procurement practices is articulated as follows

This model signifies that with all factors, including management support, distance from PFSA, IPLS skill of the staff, number of trainings, service volume level, budget, and number of pharmacy staff, set at zero, the predicted procurement performance would be 8.812 units. Specifically, the model reveals that an enhancement in management support from bad to good is associated with an increase in procurement performance by 2.255 units. Furthermore, an increase of one unit in the distance from PFSA to health facilities is correlated with a decrease of procurement performance by 0.012 units. Likewise, a rise of one unit in the number of trainings leads to an increase in procurement performance by 1.116 units. As the service volume level of health facilities changed to higher level by one level, the procurement performance also rises by 0.752 units. Finally, an augmentation of one unit in the budget is associated with a procurement performance increase by 0.8 units (see Table 5).
The multiple linear regression analysis of procurement practice.

PFSA: Pharmaceutical Fund and Supply Agency; VIF: variance inflation factor.
Dependent variable: procurement practice.
Status of storage practice
A total of 14 questions were employed to evaluate the status of storage practices. The majority of these questions yielded mean values exceeding 3.0. The question with the highest mean value was “Is the storeroom always protected from water penetration?” with a mean and standard deviation of 4.00 (0.749). Conversely, the question registered the lowest mean value was “Is an adequate budget always allocated by the facility for renovations or renewals of the store or other storage-related practices?” with a mean and standard deviation of 2.40 (0.684) (see Table 6).
Descriptive statistics of storage practice..
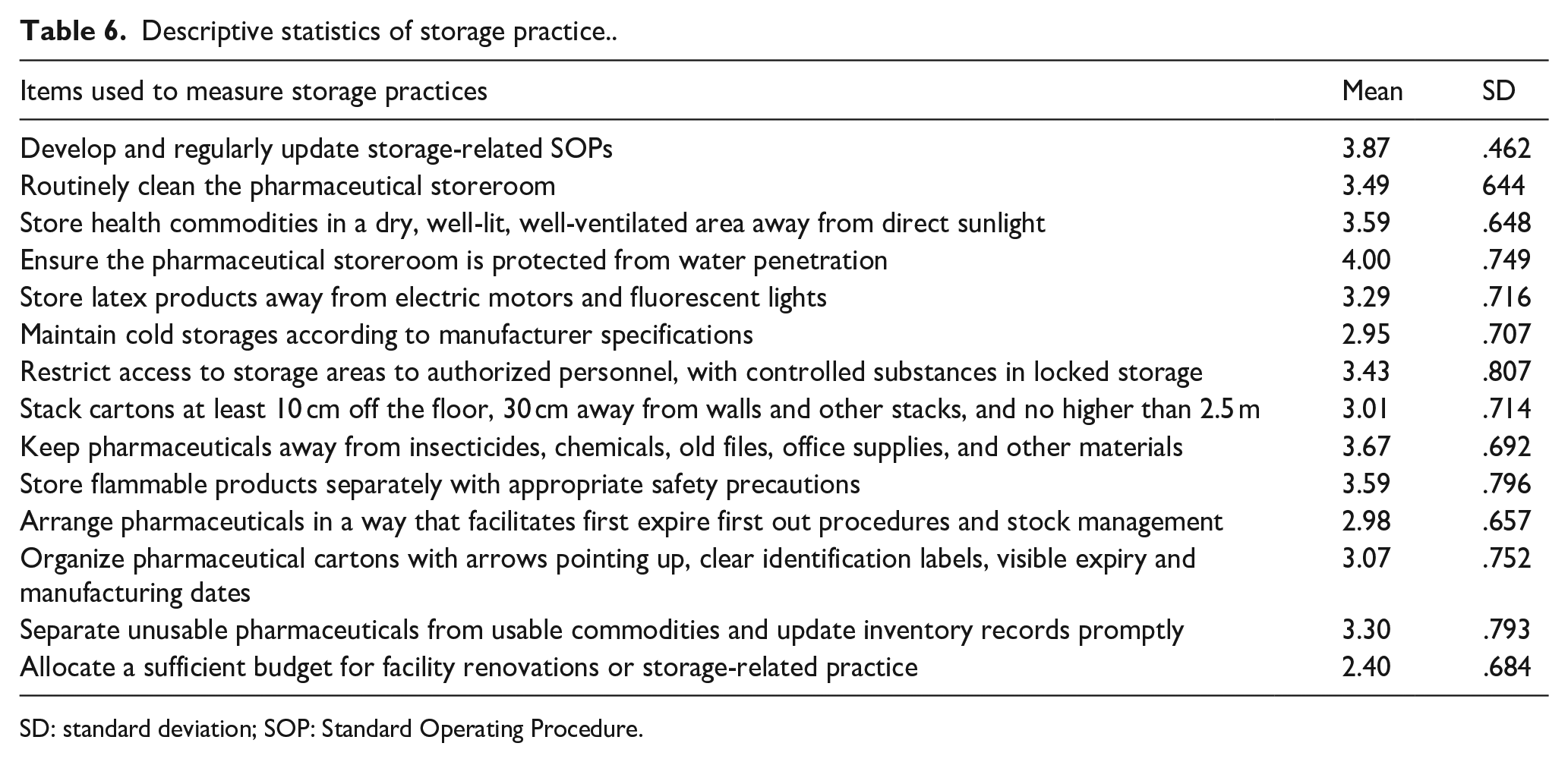
SD: standard deviation; SOP: Standard Operating Procedure.

Determinants of storage practice
The regression analysis unveiled that the coefficient of determination (R 2 ) was 0.599, signifying that 40.1% of the variability in storage practices remained unexplained by the factors of the number of trainings, management support, budget, and IPLS skill of staff. With a p-value of 0.000 (less than 0.05), the storage practice model is deemed statistically significant at a 5% level of significance (see Table 7).
The model summary for regression analysis of storage practice.

Predictors: (constant), number of trainings, budget allocation, IPLS skill of the staff, and management support.
In addition, the multiple linear regression model for storage practices is delineated as follows
The model implies that when the number of trainings, IPLS skill of the staff, budget, and management support are all valued at zero, the predicted storage practice performance is 0.96 units. Specifically, the model also revealed that as the number of trainings increases by one unit is associated with increment of the storage practice performance by 0.05 units. Likewise, as the management support changes from bad to good, the storage practice performance increases by 0.266 units. As the IPLS skill of the staff improves from bad to good, there is a corresponding increase in storage practice performance by 0.385 units. Finally, an increase of one unit in the budget corresponds to a storage practice performance increase by 0.385 units (see Table 8).
The multiple linear regression of storage practice.
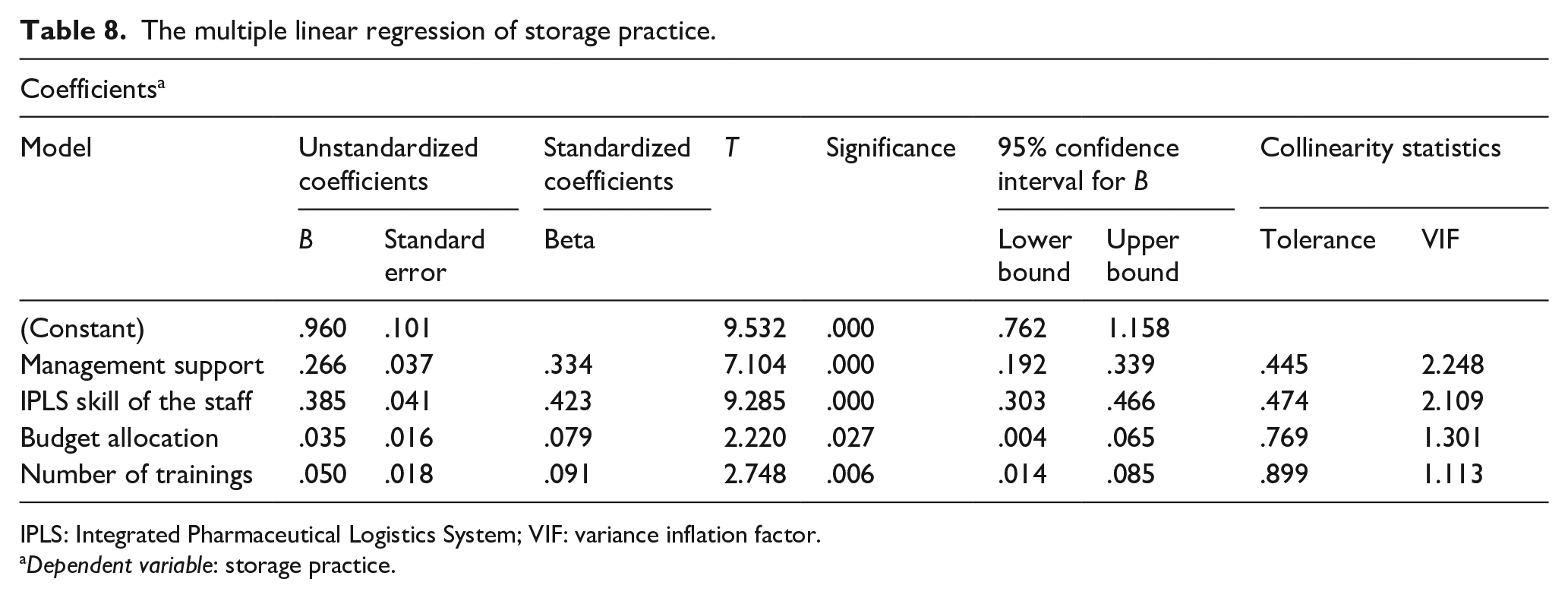
IPLS: Integrated Pharmaceutical Logistics System; VIF: variance inflation factor.
Dependent variable: storage practice.
Status of after-procurement service
Participants were asked to respond to six questions aimed at evaluating the current status of after-procurement services. The mean values of all questions were below 3.0. Among the questions, the one that garnered the highest mean value was “medical equipment has never malfunctioned due to the absence of maintenance and repair services,” scoring a mean and standard deviation of 2.72 (0.694). In contrast, the question scoring the lowest mean value was “the facility has developed and regularly updates Standard Operating Procedures (SOP) related to after-procurement service,” with a mean and standard deviation of 1.65 (0.660) (see Table 9 for detailed results).
Descriptive statistics of after-procurement service.
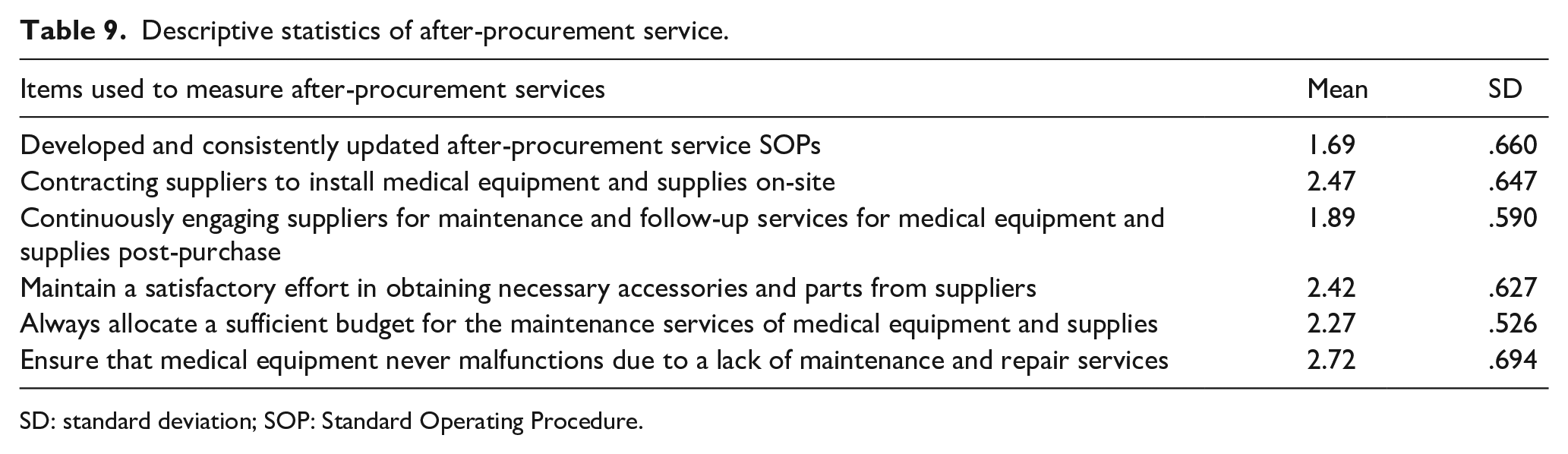
SD: standard deviation; SOP: Standard Operating Procedure.
Determinants of after-procurement service
The regression analysis uncovered that the coefficient of determination (R 2 ) stood at 0.496. This indicates that factors such as management support, budget, and distance from PFSA collectively explain 49.6% of the variability observed in the after-procurement service status. The p-value of 0.000, which is below the 0.05, implies that the after-procurement service model is statistically significant at a 5% level of significance (see Table 10).
The model summary of regression analysis of after-procurement service.

Predictors: (constant), distance from PFSA, budget allocation, and management support.
Furthermore, the multiple linear regression model can be expressed as follows

The equation illustrates that in a scenario where management support, budget, and distance from PFSA are all set to zero, the after-procurement service performance would be 1.134 units. Furthermore, the equation reveals that an improvement in management support from bad to good is associated with an increase in after-procurement service performance by 0.289 units. Similarly, one-unit increase in budget is associated with increment of the after-procurement service performance by 0.05 units. Finally, as the distance from PFSA increases by one unit, the after-procurement service performance decreases by 0.002 units (see Table 11).
The multiple linear regression analysis of after-procurement service.

PFSA: Pharmaceutical Fund and Supply Agency; VIF: variance inflation factor.
Dependent variable: after-procurement service.
Status of monitoring and evaluation
Four questions were asked to assess the status of monitoring and evaluation related to healthcare SC practices. The mean value of all the questions was less than 3.0. The question with the highest mean value was “Did the facility formulated and regularly revised SCM-related M & E indicators?” with a mean and standard deviation of 2.10 (0.606). The lowest mean value was received from the question “Has the facility developed and regularly updated SOP related to monitoring and evaluation?” with a mean and standard deviation of 1.61 (0.700) (see Table 12).
Descriptive statistics of monitoring and evaluation practices.

SD: standard deviation; SOP: Standard Operating Procedure; SCM: supply chain management.
Determinants of monitoring and evaluation
The regression analysis revealed a coefficient of determination (R 2 ) of 0.383, signifying that 61.7% of the variability in monitoring and evaluation remains unaccounted for by factors such as the number of pharmacy staff, training, and IPLS skill of staff. The low p-value of 0.000 (below 0.05) suggests that the monitoring and evaluation model holds statistical significance at the 5% level (see Table 13).
The model summary of regression analysis of monitoring and evaluation.

Predictors: (constant), IPLS skill of staff, number of trainings, and number of pharmacy staff.
Furthermore, the multiple linear regression equation for monitoring and evaluation is articulated as follows

The equation signifies that when the number of pharmacy staff, IPLS skills of the staff, and the number of trainings are all set to zero, the monitoring and evaluation performance would be −0.259 units. Moreover, it suggests that for each one-unit increase in the number of pharmacy staff, the monitoring and evaluation performance rises by 0.038 units. Similarly, with a one-unit increase in training, the monitoring and evaluation performance increases by 0.081 units. Finally, as the IPLS skill of the staff improves from bad to good, the monitoring and evaluation performance increases by 0.524 units (see Table 14).
The multiple linear regression of monitoring and evaluation.

IPLS: Integrated Pharmaceutical Logistics System; VIF: variance inflation factor.
Dependent variable: monitoring and evaluation .
Qualitative study
Challenges related to procurement practice
Extensive face-to-face interviews were undertaken with key informants to uncover hurdles associated with procurement practices. The predominant challenge, as highlighted by the majority of respondents, was the government’s constrained budget allocation for procurement. This limitation has led to a decline in the accessibility of critical and indispensable medicines and supplies. A key informant concisely expressed this concern, stated as:
The government’s budget for pharmaceutical procurement is severely restricted. The current year’s allocation is nearly identical to that of the past two or three years. Meanwhile, the costs of pharmaceutical products have notably surged, particularly from private suppliers.
Nearly all respondents expressed that the government’s procurement policy presented a difficulty in the context of pharmaceutical procurement within their health facilities. As one respondent explained:
. . . When we receive the stock-out letter from PFSA, our only option is to issue a tender to private wholesalers. However, the government’s procurement policy mandates the involvement of at least three bidders. This becomes problematic when the medicine we need is only available at one wholesaler. As a result, we are unable to purchase that item even though it is vital.
In addition, a majority of the key informants highlighted the leakage of information about product stock-outs from PFSA to private wholesalers as a significant issue. Consequently, this has led to an undesirable surge in prices by private wholesalers. As one of the key informants said:
. . . When products become out of stock at PFSA, private wholesalers promptly informed about it, leading to an immediate escalation in the prices of medicines. At times, these prices soar to two or three times the original cost per item because they know we don’t have any other option but to buy from them.
Some respondents also identified a challenge related to the untimely reimbursement of the budget by the health insurance agency. One respondent elaborated on this matter, stated as:
. . . Our community is increasingly becoming members of health insurance. Therefore, the number of patients that we are serving without direct cash payment is dramatically increasing. However, the Health Insurance Agency is not prompt in reimbursing our payments, causing frequent shortages in the budget allocated for pharmaceutical procurement in our health facility.
Challenges related to storage practice
In this study, key informants were interviewed to ascertain challenges associated with storage practices, and a predominant concern highlighted by most respondents was the lack of standardized in the pharmaceutical storeroom, identified as a significant impediment to appropriate storage practices. One respondent articulated this issue by noting:
. . . Our medicine store was not initially designed for pharmaceutical storage purposes. It was originally an antenatal care room with constrained space, and the proximity of the roof to the medicine stacks exacerbates the situation.
Furthermore, a substantial number of participants identified the lack of refrigeration facilities as a significant hindrance to effective cold chain management. A key informant elucidated on this matter, stated as:
. . . In our facility, there is only one small refrigerator that we primarily use for vaccines unless there is available space. Therefore, other products requiring cold chain storage are kept outside the refrigerator until space becomes available.”
Moreover, some respondents highlighted inadequate support from management as a substantial barrier to the implementation of effective storage practices. An informant expressed this concern, stating:
. . . The facility management exhibits reluctance in addressing diverse challenges associated with the pharmaceutical store. Notably, recommendations from supervisory visits by the Regional Health Bureau and PFSA consistently advise the acquisition of shelves and pallets. Despite concerted efforts by pharmacy professionals to advocate for these improvements, the facility management does not prioritize the matter, leading to the stacking of medicines on the floor.
Challenges related to after-procurement service
In the context of post-procurement services, key informants underwent interviews to elucidate challenges, with nearly all participants highlighting the dearth of proficient technicians capable of delivering maintenance and repair services as a prominent obstacle in the maintenance and repair of medical equipment and supplies. As one of the respondents said:
. . . Within this facility, numerous medical equipment units remain non-operational due to the absence of a skilled technician proficient in their maintenance and repair.
Furthermore, the majority of primary informants identified budgetary constraints as a significant impediment to post-procurement services within their facility. One respondent articulated this issue, stating:
. . . Our facility operates within a constrained annual budget, with a particularly limited allocation for maintenance and repair services. Meanwhile, the expenses quoted by organizations capable of offering these services are exceedingly high. Consequently, this situation leads to the accumulation of non-functional medical equipment within our facility.
Challenges related to monitoring and evaluation
Inquiries were made to key informants regarding the impediments encountered in monitoring and evaluating SC practices. Nearly all participants cited a deficiency in training for monitoring and evaluation as a primary bottleneck. As one of the informants said:
. . . This concept is unfamiliar to me, and we have not systematically undertaken monitoring and evaluation at our facility, aside from certain calculations performed at the conclusion of the fiscal year. For instance, this involves determining the overall annual expenditure on pharmaceutical procurement.
In addition, certain informants pinpointed the insufficiency of high-quality SC-related data within health facilities as a significant hurdle in the implementation of monitoring and evaluation practices. A key informant elucidated on this matter, stating:
. . . Following supportive supervision from health offices and PFSA supervisors, our attempts to carry out monitoring and evaluations for specific supply chain practices at our facility were impeded by the unavailability of requisite data.
Discussion
This study delved into the assessment of health commodity procurement practices, revealing a suboptimal performance, indicated by a mean value of 2.85. This suggests a deficient implementation of crucial procurement practices within public health facilities, exerting a notable influence on product availability and effective budget utilization. The observed underperformance can be attributed to challenges elucidated by key informants during interviews, including insufficient budget allocation for procurement, leakage of stock-out information from the PFSA to private suppliers, an incongruous government-enforced procurement policy, and delayed reimbursement of payments by the Health Insurance Agency. Importantly, these findings align with similar studies conducted in Kenya.23,24 Nevertheless, our observed procurement practice score was comparatively lower than that reported in another study conducted in Kenya. 25 This disparity might be attributed to the difference in the study scope; the Kenyan study exclusively focused on hospitals, whereas our investigation encompassed both hospitals and health centers. The outcomes of multiple linear regressions further unveiled significant associations between the procurement practice status and various factors, including management support, proximity to the PFSA, number of training sessions, health facility service volume level, and budget allocation. Thus, enhancing the performance of these identified factors holds the potential to elevate the status of procurement practices in public health facilities.
The examination of storage practices in this study, representing another facet of the heathcare SC, yielded the highest overall mean score (mean = 3.34) in comparison to the other assessed practices. This outcome implies a relatively higher success rate among public health facilities in safeguarding pharmaceutical products against damage and preserving their quality in the face of inappropriate storage conditions. Nonetheless, this score falls below that reported in a parallel study in Ghana (mean = 4.48), a difference possibly influenced by a higher non-response rate in the Ghanaian study. 26 Moreover, the outcomes of multiple linear regressions disclosed significant associations between the status of storage practices and various factors, including the number of training sessions, management support, IPLS skill proficiency of the staff, and budget allocation. In-depth interviews with key informants further highlighted poor management support, unstandardized pharmaceutical storage facilities, and an insufficient number of refrigerators for cold chain products as major challenges impeding sound storage practices. Hence, mitigating these challenges is imperative for public health facilities to optimize the performance of their storage practices.
The evaluation of after-procurement services was a crucial aspect of this study, revealing a suboptimal performance with a mean score of 2.24. This underscores a substantial deficiency in the provision of maintenance and repair services for medical equipment and supplies, leading to a notable presence of idle resources that, in turn, adversely impacts the continuity of healthcare services within these facilities. The underperformance in this practice is attributable to a limited budget allocation for after-procurement services and a dearth of skilled technicians for equipment maintenance and repair, as highlighted through qualitative interviews. Notably, the mean score in our study was lower than that reported in a parallel investigation conducted in Kenya (mean = 4.69). 12 This discrepancy can be ascribed to the scope differences between the two studies, with the Kenyan research exclusively focusing on hospitals, whereas our study encompassed both hospitals and health centers. Furthermore, the outcomes of multiple linear regression analysis illuminated significant associations between after-procurement service performance and various factors, including budget allocation, management support, and proximity to the PFSA. Addressing these factors becomes pivotal in enhancing the delivery of after-procurement services in public health facilities.
The examination of monitoring and evaluation practices pertaining to healthcare SC operations constitutes another integral facet of this study. The findings reveal that this particular practice exhibited the lowest performance compared to other healthcare SC practices, registering a mean value of 1.86. This signals a noteworthy deficiency in facilities’ ability to discern the strengths and weaknesses inherent in their healthcare SC practices, thereby hindering their capacity to undertake targeted measures for enhancing the execution of underperforming practices. The limited implementation of this practice can be ascribed to a dearth of training in monitoring and evaluation of healthcare SC practices, coupled with an insufficiency of high-quality data suitable for these processes within public health facilities. Key informants identified these factors as predominant challenges impeding effective monitoring and evaluation practices. Remarkably, the findings of this study demonstrate a lower mean score compared to a similar investigation conducted in Kenya (mean = 2.71). 23 This discrepancy may arise from contextual differences in the implementation of monitoring and evaluation practices in distinct healthcare settings.
In addition, multiple linear regression analyses elucidated significant associations between the status of monitoring and evaluation practices and several factors, including the number of pharmacy staff, the frequency of training sessions, and the IPLS proficiency of staff. Recognizing and addressing these factors is crucial for fostering an improved culture of monitoring and evaluation within public health facilities.
Limitation of the study
The study’s reliance on healthcare professionals’ perspectives as the primary data source introduces potential limitations related to bias and imprecision. Information derived solely from healthcare professionals may overlook nuances captured through document review and observation, leading to potential underrepresentation or overemphasis of certain healthcare SC practices. In addition, the questionnaire used in this study was not pilot-tested prior to administration, which may have introduced potential limitations in terms of questionnaire clarity and comprehensibility for the study population.
Furthermore, the study’s restricted discussion due to a scarcity of literature on similar healthcare SC practices in public health facilities limits the context for comparing and contextualizing findings. The absence of a robust comparative analysis reduces the depth of interpretation, and the directional bias leans toward a limited external benchmarking of the study’s results. The magnitude of this limitation is notable as it influences the generalizability and transferability of the study’s insights to broader contexts. Addressing this limitation involves acknowledging the constrained scope for benchmarking and emphasizing the need for future research to expand the literature base in this specific domain of study.
Conclusion
In conclusion, the findings of this scientific study underscore the critical gaps and challenges within the healthcare SC practices of public health facilities. The research reveals a notable underperformance in key areas such as procurement, after-procurement service, and monitoring and evaluation. While storage practices were relatively better executed, monitoring and evaluation emerged as the least implemented aspect of the healthcare SC.
Importantly, the study identifies several factors significantly associated with the performance of healthcare SC practices. The number of trainings, the IPLS skill of the staff, management support, and the proximity of health facilities to the PFSA all play pivotal roles in shaping the effectiveness of healthcare SC operations.
Furthermore, the research sheds light on the formidable challenges hindering the successful implementation of healthcare SC practices. Limited medicine availability within PFSA, budget shortages, delayed reimbursement by the Health Insurance Agency, and the absence of skilled technicians for medical equipment maintenance emerge as major obstacles. Addressing these challenges and leveraging the identified factors associated with performance could pave the way for significant improvements in the healthcare SC practices of public health facilities, ultimately enhancing the overall efficiency and effectiveness of healthcare delivery.
Supplemental Material
sj-docx-1-map-10.1177_27550834241263702 – Supplemental material for Status and determinants of healthcare supply chain practices in public health facilities, Northwest Ethiopia: Mixed-method study
Supplemental material, sj-docx-1-map-10.1177_27550834241263702 for Status and determinants of healthcare supply chain practices in public health facilities, Northwest Ethiopia: Mixed-method study by Bereket Bahiru Tefera and Gizachew Tilahun Anbessa in The Journal of Medicine Access
Supplemental Material
sj-docx-2-map-10.1177_27550834241263702 – Supplemental material for Status and determinants of healthcare supply chain practices in public health facilities, Northwest Ethiopia: Mixed-method study
Supplemental material, sj-docx-2-map-10.1177_27550834241263702 for Status and determinants of healthcare supply chain practices in public health facilities, Northwest Ethiopia: Mixed-method study by Bereket Bahiru Tefera and Gizachew Tilahun Anbessa in The Journal of Medicine Access
Supplemental Material
sj-docx-3-map-10.1177_27550834241263702 – Supplemental material for Status and determinants of healthcare supply chain practices in public health facilities, Northwest Ethiopia: Mixed-method study
Supplemental material, sj-docx-3-map-10.1177_27550834241263702 for Status and determinants of healthcare supply chain practices in public health facilities, Northwest Ethiopia: Mixed-method study by Bereket Bahiru Tefera and Gizachew Tilahun Anbessa in The Journal of Medicine Access
Footnotes
Acknowledgements
The authors are grateful to the staff of public health facilities in West Gojjam Zone for their cooperation and support in providing the necessary data, as well as their willingness to provide information via interviews. The authors also thank all data collectors because this study would not have been possible without their cooperative efforts.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.