
Abstract
Objectives:
An unintended pregnancy and unmet need for contraception remains a serious public health issues both in developed and developing countries. This study aimed to investigate the relation between unmet needs for contraception and unintended pregnancy, and identify other factors contributing for unintended pregnancy in Ethiopia.
Methods:
Data were obtained from the 2016 Ethiopian Demographic and Health Survey. A total of 7590 mothers were included. The planning status of the last pregnancy was the main outcome variable, and the unmet need for contraception was the primary explanatory variable. Bivariate and multiple logistic regressions were carried out. SPSS version 20.0 was used for data analysis. Statistical significance was declared at p < 0.05.
Results:
More than one-fourth of mothers (26.6%) gave either mistimed or unwanted birth. The rate of unmet need for contraception was 26.5%. Women with unmet need for contraception had (adjusted odds ratio (AOR) = 10.29, 95% confidence interval (CI) = 8.70–12.10) higher odds of experiencing unintended pregnancy than those who met their contraception need. Age, history of pregnancy termination, parity, women’s autonomy, and fertility preference were factors associated with unintended pregnancy.
Conclusion:
An unintended pregnancy and the unmet need for contraception remain a major public health issue in Ethiopia. A strong positive association between the unmet need for contraception and unintended pregnancy suggests that interventions targeting the unmet need for contraception could reduce unintended pregnancy. Furthermore, empowering women, promoting a clear fertility goal, and improving men’s involvement would reduce unintended pregnancy.
Introduction
Unintended pregnancy is a pregnancy that is either mistimed (occurred earlier than desired) or unwanted (occurred when no children or no more children were desired) at the time of conception. 1 Globally, 44% of pregnancies and 23% of births were unintended between 2010 and 2014. The Caribbean and eastern Africa region reported the highest rate of unintended pregnancy with 116 and 112 per 1000 reproductive-aged women, respectively. 2 Therefore, it remains an important public health issue globally, 3 as it is a major contributor to maternal and child morbidity and mortality. 4
Evidence shows that preventing unintended pregnancy would result in 26 million fewer induced abortions, 600,000 fewer neonatal deaths, and 104,000 fewer pregnancy-related deaths worldwide. 5 Furthermore, a quarter of unintended pregnancies end in unsafe abortions, one of the leading causes of maternal mortality globally. 6 In addition, unintended pregnancies might end in an unplanned birth associated with adverse outcomes like higher infant mortality and morbidity. 7 Therefore, many interventions on maternal and neonatal mortality reduction rely on preventing unintended pregnancy. 8
Generally, the global community agrees that unintended pregnancies mainly result from the unmet need for contraception, but it is not always true.9,10 Indeed, one-third of unintended pregnancies occur among women using family planning (FP) or have a met need. 11 Therefore, for effective prevention of unintended pregnancy identifying the major causes of unintended pregnancy becomes a priority.12,13 However, the major causes of unintended pregnancy are not clearly understood and multifarious, which vary in different areas and situations.9,10 Despite it merits further investigations, yet a compelling argument can be made by stating higher contraceptive discontinuation, unclear fertility goal, gender-based violence, less access to reproductive health services,9,10 and women’s fecundity may contribute for unintended pregnancy. 2
Fertility trends in developing regions saw a decline in the unintended birth rate, which indicates that a growing proportion of women and couples have realized their fertility goals due to an increase in the prevalence of contraception. 2 However, because a growing proportion of women wish to avoid pregnancy, the percentage of an unmet need for contraception fell by only 4 percentage points, from 16% in 1990 to 12% in 2014. 14 Therefore, the substantial decline in the unintended pregnancy rate in developing regions is noteworthy; this decline’s potential causes merit further investigations. 2
Ethiopia is characterized by a high maternal mortality rate (412 per 100,000 live births) with the lowest maternal health service utilization in the world. 15 Despite the met need for FP has shown a 32% improvement, rising from 8% in 2000 to 36% in 2016. However, the decrement in the rate of unmet need (from 37% in 2000 to 22% in 2016) and unintended pregnancy (from 37% in 2000 to 25% in 2016) is not equivalent to the improvement shown in contraceptive use. 15 This substantial improvement in contraceptive use with a slow decrement in the rate of unmet need and unintended pregnancy, and a higher rate of contraceptive discontinuation (35%) with the most common reason of method-related health concerns or side effects, 15 implies that the actual rate of unintended pregnancy depends not only on the rate of contraception in Ethiopia.
Considering the classification of unintended pregnancy in Ethiopia, a substantial decline in the rate of unwanted births (from 17% in 2000 to 8% in 2016) with a stagnant proportion of mistimed births (from 20% in 2000 to 17% in 2016), 15 questioned the unmet need for contraception as a major cause of unintended pregnancy in Ethiopia. Moreover, a decline in the rate of total wanted fertility rate (from 4.9 children in 2000 to 3.6 children in 2016) with a constant gap between wanted and actual fertility (women have one child more than they wanted) 15 calls for investigating factors (beyond unmet need) contributing for unintended pregnancy and investigating the relationship between these important public health issue becomes crucial. This will reveal the gap between women’s reproductive intentions and their contraceptive behavior, enabling the design of appropriate strategies and policies toward reducing their consequences. Hence, this study investigates the association between unmet needs for contraception and unintended pregnancy and identifies other factors contributing to unintended pregnancy based on the latest nationally representative data in Ethiopia.
Methods
Data source
This study used data from 2016 Ethiopian Demographic and Health Survey (EDHS), a community-based cross-sectional survey collected from January 18 to June 25, 2016. The 2016 EDHS is the fourth survey conducted in Ethiopia which was designed to provide representative data on an overview of population, maternal, and child health issues for the country. 15
Sampling and sample size
Administratively, Ethiopia is divided into nine geographical regions and two administrative cities. The 2016 EDHS sample was stratified and selected in two stages. In the first stage, a total of 645 enumeration areas (EAs; 202 in urban areas and 443 in rural areas) were selected with probability proportional to EA size based on the Ethiopia Population and Housing Census (PHC) conducted in 2007 which created a complete list of 84,915 EAs. An EA is a geographic area covering, on average, 181 households. In the second stage of selection, a fixed number of 28 households per cluster were selected with an equal probability systematic selection. 15
A total of 16,650 households were interviewed. In the interviewed households, 16,583 women aged 15–49 who were either permanent residents of the selected households or visitors who stayed in the household the night before the survey were interviewed. Interviewer administered questionnaire was used to collect data, and a total of 15,683 reproductive-age women completed the interview. 15 From these, 7590 (weighted) women who had at least one birth in the 5 years before the survey were included in the analysis.
Data collection
The 2016 EDHS used a questionnaire based on the Demographic and Health Survey (DHS) program’s standard DHS questionnaires, which were adapted to reflect Ethiopia’s population and health issues:
The input was solicited from various stakeholders representing government ministries and agencies, nongovernmental organizations, and international donors. After all the questionnaire was finalized in English, it was translated into Amarigna, Tigrigna, and Oromiffa. Next, a pre-test was conducted in clusters surrounding Bishoftu that were not included in the 2016 EDHS sample. (S1 File, p. 36)
15
A debriefing session was held with the pre-test field staff, and modifications to the questionnaires were made based on lessons drawn from the exercise. 15 The methodology details, sampling technique, data collection, and data quality assurance are available from the EDHS report.
Measurement
Outcome variable: Mother who had at least one birth in the 5 years before the survey reported whether their most recent birth was wanted at the time (planned birth), at a later time (mistimed birth), or not at all (unwanted birth). Unintended pregnancy: was coded as “yes” if the mother reported that her last birth was wanted at a later time (mistimed birth) or not at all (unwanted birth); otherwise, it was coded as “no.”
Independent variables: Unmet need for contraception was the main exposure variable in this study. It was derived by merging a variable in the data set labeled as “unmet need for spacing” and “unmet need for limiting” and coded “yes” for unmet need. The rest options provided for unmet contraception need were coded “no”; and considered met need (i.e. using contraceptives for spacing or limiting).
Based on the literature review and data availability in the EDHS data set, the following independent variables were selected for this study. Socio-demographic: Age, age at first birth, residence, education, religion, household wealth index, working status of the woman, and sex of household. Reproductive health-related variables: parity, history of pregnancy termination, current contraceptive use, desire for another child, deciding where to go and how much spending on respondents’ health care, and decision on contraceptive use.
Data analysis
Before analysis, data were weighted by SPSS complex samples procedure. Next, descriptive analysis (frequency and percentage distribution) was performed across all variables. Next, bi- and multivariate logistic regression analyses were fitted to see the effect of an independent variable on the dependent variable. Variables that showed statistically significant association (p < 0.2) in the bivariate analysis were selected as candidates for multivariate regression analysis. Before multivariate regression analysis, variables were checked for multicollinearity to ensure model adequacy for further analysis using variance inflation factor (VIF). In the first stage of multivariate regression analysis, the unmet need for contraception was entered into the model to assess their relationship with unintended pregnancy. In the second model, significant variables obtained from bivariate analysis were included. A p-value of < 0.05 was used to declare a statistical significance. All analyses were carried out with the IBM SPSS Statistics version 20.0.
Ethics approval and consent to participate
The original survey was conducted after being ethically approved by the National Research Ethics Review Committee (NRERC; Ref. No. 3.10/114/2016). The interview continued only if participants’ written consent to participate, and privacy was certain. Before analysis, the authorization for using the data in this study was granted from the DHS program upon submitting the study’s aims and the research plan.
Results
Socio-demographic and reproductive health characteristics
Out of a total of 7590 (weighted) women who had at least one birth in the 5 years before the survey, the majority of them (69.7%) were between the age of 20 and 34 years. About 39.1% of respondents gave the first birth before the age of 18 years. The majority of women were rural residents (87.2%) and did not attend formal education (63.1%; Table 1).
Socio-demographic and reproductive health characteristics of women who had at least one birth in the 5 years preceding the survey, 2016 EHDS (n = 7590).
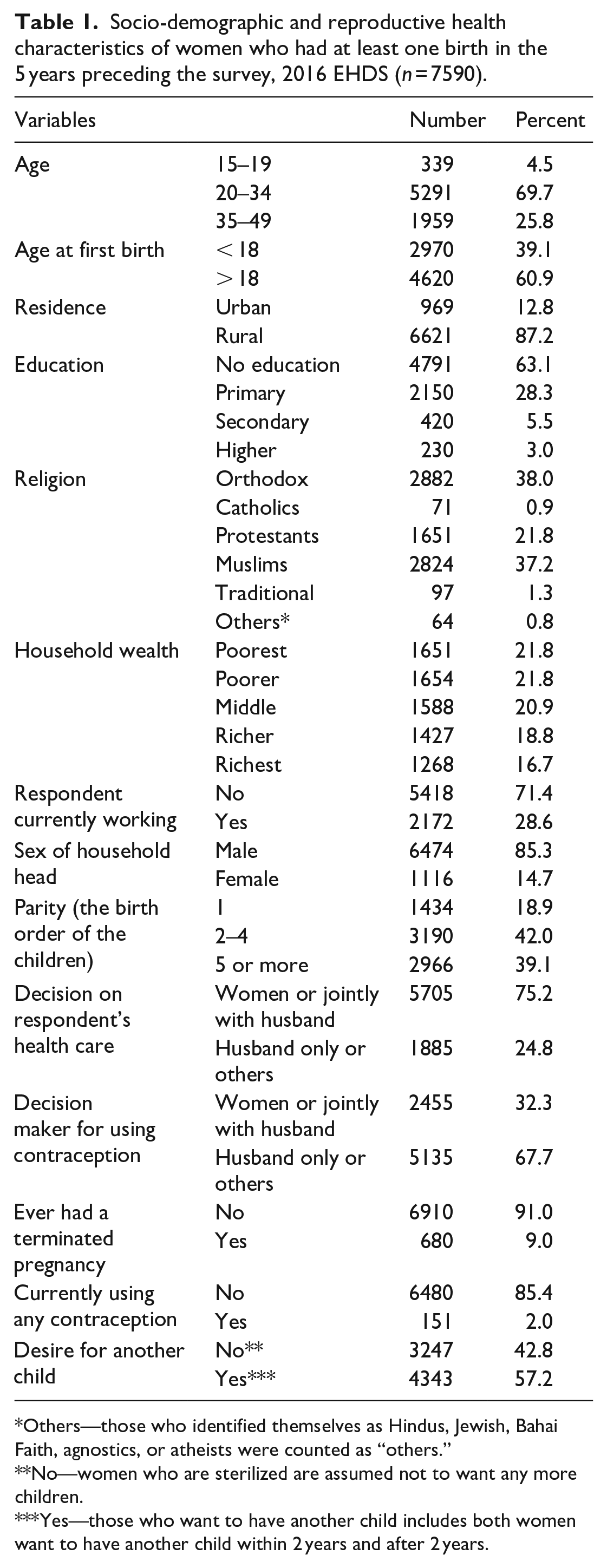
Others—those who identified themselves as Hindus, Jewish, Bahai Faith, agnostics, or atheists were counted as “others.”
No—women who are sterilized are assumed not to want any more children.
Yes—those who want to have another child includes both women want to have another child within 2 years and after 2 years.
Unintended pregnancy and unmet need for contraception
In Ethiopia, many births were wanted at the time of conception (73.4%), while 26.6% were unintended births (either mistimed or unwanted births). Similarly, 26.5% of respondents reported an unmet need for contraception in Ethiopia (Table 2).
Unintended pregnancy and unmet need for contraception among women who had at least one birth in the 5 years preceding the survey, 2016 EDHS (n = 7590).

The association between unmet need and unintended pregnancy
In the first stage of analysis, the unmet need for contraception was entered into the model to assess their relationship with unintended pregnancy. It shows that mothers who reported an unmet need for contraception (adjusted odds ratio (AOR) = 1.12, 95% confidence interval (CI) = 1.01–1.22) were more likely to have unintended pregnancies for their most recent birth. In the second model, significant variables obtained from bivariate analysis were added to examine their association with the outcome variable. The association between unmet need and unintended birth becomes strong after adjusting for socio-demographic and reproductive variables. Unintended pregnancy among mothers with unmet need for contraception was (AOR = 10.29, 95% CI = 8.70–12.10) ten times higher than mothers who met their contraception need (Table 3).
Factors associated with unintended pregnancy among mothers who had at least one birth in the 5 years preceding the survey, 2016 EDHS.

CI: confidence interval; AOR: adjusted odds ratio.
AOR = adjusted for age, age at first birth, wealth, education, residence, religion, parity, employment status, history of pregnancy termination, desire for more children, and women decision-making.
Factors associated with unintended pregnancy
Age, religion, parity, history of pregnancy termination, fertility preference, and women’s autonomy were other factors significantly associated with unintended pregnancy in the final analysis model. Table 3 presented the result of both bi- and multivariate levels of analysis.
The age of respondents at the time of the survey was significantly associated with unintended pregnancy. Young age women (15–19 years; AOR = 2.06, 95% CI = 1.40–3.04) were more likely to have an unintended pregnancy than older women (35–49 years). In addition, women in specific categories of religion (i.e. Orthodox, Catholic, Protestant, Muslim, or Traditional) were less likely to experience unintended pregnancy than those in the “Other” category of religion.
Parity was found to significantly affect the occurrence of unintended pregnancy, which becomes higher among grand multiparous women. For example, a mother who had one child (AOR = 0.66, 95% CI = 0.51–0.85) and two to four children (AOR = 0.83, 95% CI = 0.70–0.98) were less likely to have an unintended pregnancy as compared with those who had five or more children after controlling for socio-demographic and reproductive variables.
Having a say in own health care decision was positively associated with unintended pregnancy. Women who can decide where to go and how much spending on health care alone or jointly with their husband (AOR = 0.42, 95% CI = 0.36–0.49) were less likely to have an unintended pregnancy than mothers for whom husband only or others make a decision.
Women with no history of pregnancy termination ever (AOR = 0.63, 95% CI = 0.52–0.77) had lower odds of experiencing unintended pregnancy than those who terminated a pregnancy at least once. Furthermore, women who did not desire another child had a 1.73 (95% CI = 1.51–1.98) times higher chance of having unintended pregnancy than those who wish to have another child (Table 3).
Discussion
This study investigates the association between unmet needs for contraception and unintended pregnancy and identifies other factors associated with unintended pregnancy in Ethiopia. Despite the impressive, increasing trend of contraceptive use in Ethiopia, in this study, a higher rate of unintended pregnancy (26.6%) and unmet need for contraception (26.5%) were reported. These findings suggest that both unintended pregnancy and the unmet need for contraception remain important public health concerns in Ethiopia. Almost similar prevalence of unintended pregnancy was reported by a study conducted in Addis Zemen and Gelemso General Hospital, Ethiopia.16,17 However, it was lower18–21 and higher than other studies22–25 conducted in different parts of Ethiopia. On the other hand, the rate of unmet need for contraception in this study was higher than a study conducted in Sidama Zone, Ethiopia (19.1%), 26 and much lower as compared with Angola (51.7%). 18 These disparities could relate to the difference in the availability and accessibility of reproductive health services, including access to modern contraceptives in the study areas.
In this study, unmet need for contraception was significantly associated with unintended pregnancy. Women with an unmet need for contraception had more than ten times higher odds of experiencing unintended pregnancy than those who met their contraceptive need. This association becomes strong in multivariate analysis after the addition of covariates, including age, parity, fertility desire, and autonomy. Suggesting that the higher rate of unmet need for contraception among young age (15–19 years), multiparous women, and women who meet their fertility goal (did not have a desire for another child) drives this strong relation between unmet need and unintended pregnancy, which resembles EDHS and other study reports in Ethiopia. This finding suggested that unmet need or contraception is the major cause of unintended pregnancy, which was in line with other studies conducted in Angola and Bangladesh.18,21 This could be related to a general explanation that the unmet need for contraception exposed women to the risks of unwanted pregnancy. Therefore, these findings reveal that addressing the unmet need among young, multiparous, and want no more children is a good opportunity to reduce unintended pregnancy in the country.
Young age women (15–19 years) were more likely to have an unintended pregnancy than older women (35–49 years), which was not similar to a study conducted in Jimma and Arsi Negele Woreda, Ethiopia.27,28 This could be attributed to inadequate access to contraceptive services due to stigma and discrimination and risky sexual behavior, such as multiple sexual partnership and early sexual debut. Moreover, most adolescents in Sub-Saharan African countries have low knowledge on contraceptives, inadequate access to information on sex due to socio-cultural norms and practices of society, and lack the ability to negotiate for safer sex in sexual unions. 18
In this study, unintended pregnancy was higher among multiparous women, consistent with a study done in Addis Zemen and Gelemso General Hospital.16,17 Another similar result was found in Arsi Negele Woreda, where pregnant women with a parity of 3 and above were more likely to experience unintended pregnancy. 28 This could be explained by the proportion of women who want no more children increases with the number of living children. Therefore, the pregnancy among multiparous women is more likely to be unintended.
Mothers who decide alone or jointly with their husbands on respondent’s health care were less likely to have unintended pregnancy for their most recent birth, which implies that women’s participation in household decision-making is a protective factor for unintended pregnancy. This was consistent with studies conducted in Arsi Negele and West Belessa Woreda, Ethiopia.25,28 This shows that being autonomous or participating in the respondent’s health care decision encourages planning for future fertility desires and helps manage problems of unwanted pregnancy.
In this study, women who had no history of pregnancy termination ever had lower odds of experiencing an unintended pregnancy. Thus, in most instances, women with no history of pregnancy termination met their need for contraception and became less likely to experience unintended pregnancy and birth. On the contrary, a study done in Arsi Negele, Ethiopia, reported similar findings, 28 which might be due to the differences in the proportion of unintended pregnancies that end in abortion.
Regarding fertility preference, women who did not desire another child had higher odds of experiencing unintended pregnancy than those who wish to have another child. This was similar to a study done in Jimma which reported that the lower number of children desired, the higher the risk of unintended pregnancy. 27 This could be attributable to the fact that any event of pregnancy among mothers who desired no more children would be unintended.
Previous studies have focused mostly on the adverse health consequences and associated factors of the unmet need for contraception and unintended pregnancy. In contrast, this study presents the relationship between the unmet need for contraception and unintended pregnancy. The findings of this study confirmed that the unmet need for contraception is a major contributing factor for unintended pregnancy. This study also reinforces the findings on the growing body of knowledge by showing that age, history of pregnancy termination, parity, women’s autonomy, and fertility preference were other factors associated with unintended pregnancy.
The findings of this study need to be interpreted in light of some limitations. It was difficult to determine the direct relationship between unmet need for and unintended pregnancy due to the cross-sectional nature of the data used for analysis. In addition, unintended pregnancy may have been under-reported after a child is born because of the joy of having a child.
Conclusion
Unintended pregnancy and the unmet need for contraception remain a major public health concern in Ethiopia. A strong positive association between the unmet need for contraception and unintended pregnancy suggests that unmet need is a missed opportunity to address unintended pregnancy. Therefore, an intervention targeting unintended pregnancy would be benefited more by addressing and considering the issue of the unmet need for contraception. Age, religion, parity, pregnancy termination, fertility preference, and women’s autonomy were other factors significantly associated with unintended pregnancy. Therefore, empowering women, promoting a clear fertility goal, and improving male involvement would reduce unintended pregnancy.
Supplemental Material
sj-pdf-1-map-10.1177_23992026211033436 – Supplemental material for The association between unmet need for contraception and unintended pregnancy among reproductive-age women in Ethiopia
Supplemental material, sj-pdf-1-map-10.1177_23992026211033436 for The association between unmet need for contraception and unintended pregnancy among reproductive-age women in Ethiopia by Awoke Giletew Wondie in Medicine Access @ Point of Care
Footnotes
Acknowledgements
The author would like to thank the DHS program for conducting this comprehensive population and health survey and allowing us to use the data.
Contributorship
The author declares that he has participated fully in data acquisition, further analysis and interpretation of data, drafting the article and revising it critically for important intellectual content, and final approval of the version to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.