
Abstract
Autism diagnostic assessment for children and young people tends to focus on within-individual ‘deficits’ and non-autistic interpretation of observable behaviours. In contrast, a neurodiversity-affirmative assessment involves centring autistic perspectives, focusing on strengths, differences and needs, and acknowledging the role of the environment. The present study was designed to focus on professionals’ perspectives on neurodiversity-affirmative autism diagnostic assessment. Autism community stakeholders were consulted on the design of the interview schedule. Semi-structured interviews were conducted with 19 professionals aged 30 to 73 years who work in a multidisciplinary team within the United Kingdom. Reflexive thematic analysis was used to identify themes. Professionals described a holistic, balanced assessment involving assessing individual and contextual strengths and needs. According to professionals, assessing strengths could be beneficial for autistic children and young people's long-term wellbeing. Professionals also highlighted an autistic person-centred assessment and a strengths-and-needs-led, rather than diagnosis-led approach. These findings highlight the importance of a holistic, person-centred, strengths-and-needs-led assessment that has the potential to support autistic thriving.
Lay abstract
Autism diagnostic assessments tend to focus on difficulties within an individual. They also tend to focus on how people who aren't autistic interpret observable behaviours. It is important to take a neurodiversity-affirmative assessment approach. This involves focusing on what autistic people say. It also involves looking at strengths and needs and thinking about how the context a person is in may influence their experiences. We wanted to find out what professionals involved in autism diagnostic services think about neurodiversity-affirmative autism diagnostic assessment. We focused on services for children and young people. We asked autistic adults and parents/carers of autistic children to help us design our interview questions. We then interviewed 19 professionals who work in the United Kingdom. We used a qualitative method called reflexive thematic analysis to analyse the data. The professionals we interviewed described a holistic assessment which involves assessing the strengths and needs of the individual and the context a person is in. According to professionals, assessing strengths could benefit autistic children and young people's wellbeing in the long run. Professionals also discussed valuing the child's views in an autistic person-centred assessment. Our findings also emphasise an approach that focuses on strengths and needs rather than diagnosis.
Introduction
Autism diagnostic assessment for children and young people is an important event in autistic children and young people's and their family's lives, as it frames their understanding of themselves or their child (e.g. Brown et al., 2021) and is often key for accessing and informing support (National Institute for Health and Care Excellence (NICE), 2017). Therefore, it is important that we consider carefully how autism is assessed. Typically, diagnostic assessments rely on professionals assessing observable behaviours in relation to diagnostic criteria (American Psychiatric Association (APA), 2013; NICE, 2017; World Health Organization (WHO), 2019). This usually involves conversations about and observations of social communication and interaction and ‘restricted and repetitive behaviours’. These behaviours tend to be viewed as ‘deficits’ that reside solely within the child or young person. Within the DSM-5 (APA, 2013) and ICD-11 (WHO, 2019), autism is described as a ‘disorder’. Deficit-focused language features heavily, including words or phrases like ‘deficits’, ‘abnormal’, ‘restricted, repetitive patterns of behavior’ and ‘symptoms’. Because these behaviours are different to what neurotypical people consider to be ‘normal’, they are often interpreted as deficits, even when autistic people perform better than non-autistic people (Pellicano & den Houting, 2022).
The reliance on comparisons to neurotypical behavioural norms also means that our understanding of autism, and hence how it is assessed, is based on non-autistic views of what it is like to be autistic. This is linked to the idea that autistic people's self-reports are inaccurate (Mazefsky et al., 2011) – which has received limited support (e.g. Kenworthy et al., 2022). Hence, autism diagnostic assessment prioritises outsider rather than insider perspectives of autistic experiences (Ratto et al., 2023). This neglects the double empathy problem (Milton, 2012), meaning that potential neurotypical misinterpretations of autistic experiences are overlooked, thus limiting the authenticity of information acquired within assessment.
The focus on deficits that reside within the autistic person and non-autistic interpretation of autistic behaviours reflects the dominance of the medical model of disability that underpins autism diagnostic assessment. In contrast, according to the neurodiversity paradigm, autism is viewed as a form of neurodivergence characterised by difficulties, differences and strengths (Dwyer, 2022; Kapp et al., 2013; Pellicano & den Houting, 2022; Walker, 2014). Proponents of this approach also advocate for the importance of centring autistic perspectives, for example, through adopting participatory research practices (e.g. Pickard et al., 2022) and focusing on autistic perspectives of their own experiences. According to the neurodiversity paradigm, autism is viewed as a different way of being, rather than a ‘disorder’. Research and support therefore focus on goals that matter to autistic people (e.g. quality of life/wellbeing) rather than attempting to ‘fix’ or ‘normalise’ autistic people (Dwyer, 2022; Pellicano & den Houting, 2022). Further, rather than focusing on deficits that reside solely within the child or young person, the neurodiversity paradigm aligns with an ecological or interactionist model of disability, which represents a middle ground between the strong social model of disability and the medical model (Dwyer, 2022; Mandy, 2023; Shakespeare, 2013; Shakespeare & Watson, 2001). Ecological/interactionist models of disability argue that disability results from the interaction between the individual and the environment. Thus, if there is a good fit between the person and the environment, autistic people may not have difficulties (Leadbitter et al., 2021; Mandy, 2023). Aligning with this approach, research and support focus on the role of the environment in shaping autistic experiences and environmental supports to improve the person-environment fit.
Adopting a neurodiversity-affirmative approach to autism diagnostic assessment would involve understanding an autistic child or young person in a more balanced, holistic way. This includes conducting a detailed assessment of neutral differences and strengths (as well as difficulties) and using more neutral or positive language (Abrahamson et al., 2021; Brown et al., 2021; Ratto et al., 2023; Rutherford et al., 2021). Adopting a more balanced perspective may benefit autistic people's wellbeing, as deficit-focused, ableist language that discriminates against disabled people is related to stigma, marginalisation, and poor mental health for autistic people (Bottema-Beutel et al., 2021; Pearson & Rose, 2021). Generating more balanced understandings of autism within diagnostic contexts may feed into how members of wider society view autism, which may reduce the impact of stigma and marginalisation on autistic people. Within diagnostic contexts, adopting a more balanced perspective could also promote more positive experiences for autistic children and young people and their parents/caregivers (Abbott et al., 2013; Anderberg & South, 2021; Crane et al., 2018; Makino et al., 2021; Mulligan et al., 2012; Nissenbaum et al., 2002). For example, documenting strengths and feeding this information back to children and young people and their parents/caregivers may result in enhanced self-esteem and greater trust between parents/caregivers and professionals (Crane et al., 2018).
A neurodiversity-affirmative assessment would also acknowledge the role of the environment in shaping autistic experiences, for example, by conducting a detailed assessment of contextual strengths and needs. This could allow a more holistic understanding of the child or young person to be gained. A neurodiversity-affirmative autism diagnostic assessment would also involve focusing on children and young people's perspectives as part of a person-centred assessment. This could involve focusing on obtaining the child or young person's views on their strengths and needs and involving the child or young person in decision making concerning the services they use. The approach taken to obtain children and young people's perspectives may depend on their age and communication ability. For example, creative or play-based methods (Lewis et al., 2024) or other approaches could be used to capture the views of younger children (e.g. infants/toddlers) or those with communication support needs. Focusing on children and young people's perspectives allows more authentic understandings to be gained based on insider perspectives of autistic experiences (Ratto et al., 2023), which is also respectful as it acknowledges children and young people as experts of their own experiences. Involving autistic people in decision making in particular can improve the relevance and quality of diagnostic services (e.g. see Curnow et al., 2023; Maciver et al., 2023; Rutherford et al., 2021).
Researchers have discussed the importance of neurodiversity-affirmative diagnostic assessments. For example, Brown et al. (2021) offer suggestions for how diagnosticians can share a diagnosis with families in line with a neurodiversity-affirmative perspective. Examples include using more neurodiversity-affirmative language and discussing a balance of strengths and needs. However, as far as we are aware, there is no published research focusing specifically on the autism community's perspectives relating to neurodiversity-affirmative autism diagnostic assessment. This represents a unique opportunity to research this unexplored area, which has the potential to inform how professionals can improve the way they carry out diagnostic assessments in ways that support autistic people to thrive. We decided to focus on healthcare professionals’ views as they play a key role in diagnostic assessment (Crane et al., 2018; Rogers et al., 2016).
Present study
This study aimed to explore the perspectives of professionals working as part of a multidisciplinary autism team on neurodiversity-affirmative autism diagnostic assessment. We focused on assessments for children and young people (from birth up to age 19 years; NICE, 2017). The research question was: what are the perspectives of professionals working as part of a multidisciplinary autism team on neurodiversity-affirmative autism diagnostic assessment? Our study was guided by a ‘neurodiversity-affirmative autism diagnostic assessment’ framework which was developed as part of the first author's doctoral study (Pritchard-Rowe, 2024). This framework includes two interrelated concepts that capture the previously discussed key ideas: ‘holistic’ (with two interrelated subconcepts: ‘balanced’, ‘acknowledging the role of the environment’) and ‘person-centred’. ‘Balanced’ involves understanding autism in terms of difficulties, differences and strengths. In terms of autism diagnostic assessment, a neurodiversity-affirmative approach could involve detailed assessment of neutral differences and strengths as well as difficulties, and using more neutral or positive language (Abrahamson et al., 2021; Brown et al., 2021; Ratto et al., 2023; Rutherford et al., 2021). ‘Acknowledging the role of the environment’ involves understanding that autistic experiences (strengths and needs) arise from the interaction between the environment and the person, in line with an ecological/interactionist perspective. Within a neurodiversity-affirmative diagnostic assessment, this could involve a detailed assessment of how the context shapes autistic experiences, such as assessing contextual strengths and needs. The second key concept in the framework, ‘person-centred’, refers to centring autistic perspectives within assessment in various ways. The key aim is to put the person and what is important to them at the centre of the process. This could involve focusing on obtaining the person's views, for example, about their strengths and needs. It could also include involving the person in decision making around the diagnostic services they access. The age and communication ability of the person would determine the approach taken to obtain their perspectives. According to this framework, for autism diagnostic assessment to be neurodiversity-affirmative, it must be both holistic and person-centred.
We conceptualise this study as neurodiversity-informed, with a view to informing neurodiversity-affirmative practice. Whilst this article focuses on children and young people, we believe that the core principles of neurodiversity-affirmative diagnostic assessment could apply to assessing adults.
Methodology
This study adopted a qualitative design using semi-structured interviews that were analysed using reflexive thematic analysis (Braun & Clarke, 2021). Ethical approval was awarded by the Faculty of Education Research Ethics Committee. Prior to data collection, participants (healthcare professionals) provided written and verbal informed consent. We use pseudonyms in this article to protect participants’ anonymity. We pre-registered (and recorded changes to) the study on the Open Science Framework (OSF; https://doi.org/10.17605/OSF.IO/AJPV3).
Participants
We recruited 19 healthcare professionals (including medical doctor, allied health, and psychological professionals) working as part of multidisciplinary autism teams within the United Kingdom aged 30 to 73 years (M = 42.79, SD = 13.31) using purposive and snowball sampling (see Table 1 for participant demographics). We recruited via advertising on X (formerly Twitter), through use of existing contacts and via participants who were asked to pass on details of the study to other professionals. We focused on professionals who contribute to the diagnostic assessment of children and young people (NICE, 2017). According to NICE (2017) guidelines, the core members of a multidisciplinary autism team comprise of a paediatrician/child and adolescent psychiatrist, speech and language therapist and psychologist. Other professionals may also contribute to the diagnostic assessment, such as occupational therapists, specialist health visitors or specialist nurses. We sought and obtained data from professionals with a range of professional roles. We did not ask participants for information on their socioeconomic status and so this was not recorded.
Participant demographics.

Note. Percentages may not total 100 due to rounding.
Participants could select more than one category.
CAMHS: Child and Adolescent Mental Health Services.
Interview design, methods and community involvement
The first author (EP-R) conducted semi-structured interviews with participants. These were primarily carried out via video (Zoom or Microsoft Teams) or telephone call, depending on each participant's preference. Interview length ranged from approximately 44 to 65 min. We included in the final sample of participants one person who originally completed a pilot interview. This interview was completed in-person. We recorded the audio interviews. The interview schedule was informed by the ‘neurodiversity-affirmative autism diagnostic assessment’ framework adopted for this study (see Supplemental material 1/https://osf.io/qjrxt/ for interview schedule). We consulted four autistic adults and parents/carers of autistic children on the design of the interview schedule. Consultants were emailed the interview schedule document and gave feedback verbally and/or in written form. Consultants were emailed a document with the summary of the feedback and changes made (see https://osf.io/qjrxt/). Changes included combining two questions into a single question, editing questions for clarity and adding follow-up questions (e.g. ‘How should professionals interact and communicate with autistic people and their families?’). The interview schedule was further refined following piloting with professionals. Consultants were paid £25 per hour (for a maximum of 2 hours). The interview questions related to views on what a strengths-based autism diagnostic assessment could look like and benefits and limitations of this type of assessment. We used the term ‘strengths-based’ when recruiting and talking to consultants and participants as we felt that this would be a more descriptive, familiar term than ‘neurodiversity-affirmative’. However, the interview questions related to the concepts of the ‘neurodiversity-affirmative autism diagnostic assessment’ framework. For example, the question ‘How should the child or young person's family and wider social contexts be considered in assessment?’ was designed to relate to the ‘acknowledging the role of the environment’ subconcept of the ‘holistic’ concept. Professionals received a £25 gift voucher for participating. The first author transcribed the interviews verbatim using Otter.ai and NVivo 12 and anonymised them. Transcription was based on guidelines by Braun and Clarke (2013).
Data analysis
EP-R led the analysis with support from the second author (JG). We used reflexive thematic analysis because it allows patterns to be identified across a relatively large dataset and its theoretical flexibility allows for analysis to be shaped by a ‘neurodiversity-affirmative autism diagnostic assessment’ framework. We followed Braun and Clarke's (2021) iterative six-phase process: (1) familiarising yourself with the dataset, (2) coding, (3) generating initial themes, (4) developing and reviewing themes, (5) refining, defining and naming themes and (6) writing up. We adopted a critical realist/contextualist framework to recognise the context-dependent nature of participant's descriptions and the role we have as researchers in constructing the data produced (Braun & Clarke, 2021). After becoming familiarised with the data, EP-R coded all the transcripts inductively, to reflect the data content explicitly. EP-R then generated and refined the themes using a deductive approach, in which the ‘neurodiversity-affirmative autism diagnostic assessment’ framework was used as a guide to shape the final list of themes and subthemes. We used NVivo 12, excel and Miro software to aid analysis. For example, Miro was used to generate thematic maps to help review themes. To maximise the quality of the research (Braun & Clarke, 2021), EP-R kept a reflexive journal throughout the research process, which included reflecting on how her positioning and research practices influence data interpretation. We have also reflected on our positionality (Supplemental material 2). To clarify and validate analytical insights, we presented the analysis to other researchers at the institution (Braun & Clarke, 2021).
Results
Figure 1 shows the themes and associated subthemes. We discuss and illustrate these with supporting quotations.

Themes and subthemes.
Both strengths and needs are important
This theme explores participants’ views relating to the importance of assessing both strengths and needs within diagnostic assessment.
‘Balanced assessment’
Participants expressed that diagnostic assessment should not be based solely on strengths or needs but should be a ‘balanced assessment’ (Emily). This involves a shift from current deficit-focused practices towards those that involve assessment of both strengths and needs: ‘I think you need balance, but I definitely think that focusing – yeah, highlighting the strengths more than we currently do, I think would be a good thing to do’ (Faith). Evelyn highlighted how it is ‘unrealistic’ to conduct a solely strengths-based assessment, and further reflected on how the current diagnostic model presents a barrier to conducting a balanced assessment: ‘at the moment we exclude it [strengths] totally because we are so, the DSM on which we base our diagnosis is so deficit-based really’.
Moving away from deficit language
As a way of shifting from a deficit-focused to a balanced assessment, participants emphasised a reframing of deficit-based language to more neutral or positive terminology, for example relating to reports or diagnostic criteria. In relation to this, ideas consistent with the neurodiversity paradigm, including ‘difference rather than deficit’ (Nicola) and rejection of autism as a disorder or disease were commonly expressed. For example, Samantha emphasised that ‘absolutely, first and foremost … I would not be using ASD [autism spectrum disorder], disorder would be absolutely removed from the vocabulary of my team’. A few participants explicitly referred to terminology consistent with the neurodiversity paradigm, for instance, Sophia mentioned that ‘within kind of the service I work in, lots of us are trying to write diagnostic reports using more kind of neuroaffirmative language’. Sophia clarified that this included using phrases like ‘differences in approach’, ‘preferences in’, and ‘different communication styles’. Lucy also described how their team were changing their terminology towards a ‘neurodiversity slant’: ‘instead of where previously we would have talked of, you know, restricted interests and specialist interests, we’re trying to move towards terms like, you know, their focused interests or their passions’.
Strengths important for mental health and wellbeing
Relating to why diagnostic assessment should include an assessment of strengths, participants highlighted how assessing strengths, and consequently communicating this information, is key for children and young people's and parents/caregivers’ mental health and wellbeing. In particular, participants emphasised that assessing strengths is central for children and young people's self-esteem or sense of self: …thinking about some of the clients that I would have, or would have had over the years, you know, it (has) sort of stuck with me that, we have picked apart what they couldn’t do, and that there needs to be a way that actually doesn’t rip someone's self-esteem to shreds. (Lucy)
Some reflected on the longer term, post-assessment benefits of assessing strengths, particularly for children and young people's mental health and wellbeing. For example, Grace articulated that …for the course of the lifespan of that- that young person starting off thinking about actually what they can do, rather than what they can’t and what their strengths are, rather than what they can’t do. I think that sets somebody up to lead a fulfilling, well balanced, mentally healthy kind of life.
Participants also emphasised how assessing strengths could result in more positive assessment experiences, particularly for parents/caregivers: ‘If they come in, and it is a strengths-based assessment, that would help the parents look back on that day as being a positive moment for them as a family, rather than a negative experience’ (Brittany).
Assessing needs important for support
Relating to why diagnostic assessment should include an assessment of needs, participants emphasised that parents/caregivers and young people tend to seek an assessment because their children/they have needs that they require support with. For example, Joe articulated that I think the risk potentially is that, that I guess you focus almost solely on those strengths. And then kind of you’re then perhaps left with the young person or family kind of going ‘well, that's great. But, I still feel like there's these areas that I need help with. And actually, they’ve not been captured as part of this process as well’.
Participants also highlighted how, under the current system, access to support is dependent on assessing needs or receiving a diagnosis (which is based on assessing needs): ‘obviously, it's important for their EHCP [Education, Health and Care Plan] … to be clear on their needs as well’ (Linda). Similarly, Diane stated that ‘… in order to get – particularly to get the help you need you – at the moment a diagnosis is – appears to be needed’.
(Strengths-and-) needs-led not diagnosis-led
In contrast to current assessment practices that are diagnosis-led, some participants suggested that assessment should be (strengths-and-) needs-led: ‘… we should be moving from a more, as I said, from the focusing purely on diagnosis to looking at the child's needs. And I guess that's really their strengths and needs’ (Isaac). Instead of access to support being dependent on diagnosis (see ‘assessing needs important for support’), participants emphasised a support-oriented approach that prioritises providing support based on assessment of needs, sometimes with support provided during assessment or before diagnosis. For example, Joe described an assessment where ‘we’ve recognised the strengths and needs, let's do this [support] now’. Similarly, Sharon described ‘that should be part of the assessment process, (is) that we’re actually identifying some key strategies or tools that will – the child responds really well to, and actually trying them within your assessment process’. Participants also articulated that a (strengths-and-) needs-led assessment is more informative than a diagnosis-led assessment: ‘where the outcome is, a better description of somebody's strengths, preferences and support needs’ (Sophia).
Considering the context
Participants emphasised the need to consider the context within assessment: ‘a person can never be considered outside of their context, because so much [of] what we do and feel and think is context-related’ (Evelyn). Participants reflected on how children and young people behave differently in different contexts, with some highlighting the context-dependent nature of strengths and needs: ‘whether that [a] difference is a strength or a weakness or a challenge or a difficulty depends on the, like, the context and environment’ (Jason). As such, participants highlighted an assessment process involving the various settings that children and young people spend their everyday lives in, particularly relating to family and education. For example, Samantha reflected on how ‘…it's vital to include them [family and school]’. This approach included conducting assessments, such as observations, in different settings or gaining family or educational reports regarding a child or young person's strengths and/or needs. Participants also discussed the importance of assessing a variety of contextual strengths and needs, such as those relating to ‘what the relationships are within the family’ (Dominic).
Autistic person-centred
This theme explores participants’ views around an autistic person-centred assessment, involving ‘putting the person at the centre of everything we’re doing’ (Samantha). The next two subthemes exemplify in more detail what constitutes an autistic person-centred assessment. Although participants discussed a family-centred process too, this theme prioritises autistic views because historically, these have tended to be neglected.
Importance of autistic voices
Participants highlighted the need to focus on autistic views as part of assessment, including asking the child or young person for their views and valuing the information they share. For example, Nicola described how it is important to obtain the persons’ opinions ‘on their strength[s] and what they want from the assessment’, including asking questions such as ‘What do you think you do well?’ and ‘Why do you like that?’. Sophia similarly argued that it is important to ‘[hear] about the things that they [the child or young person] feel that they’re good at, as well as kind of, what their preferences and their internal experiences are’. Related to this, participants emphasised a collaborative or equal relationship with the child or young person. For example, Rebecca articulated how this involves a real shift away from thinking we are the clinicians, we’re the professionals, we have all the answers. We’re here to help. We’re here to kind of tell you what we think. It's more about helping people find the answers together for themselves and seeing … what I guess, to a certain extent, what the child or the young person brings to the table and their knowledge and understanding of themselves.
As hinted at by Rebecca and suggested by some others, this relationship depends somewhat on the child or young person's age, ‘insight’, or ‘communication skills’: ‘the majority of children we see are probably too, maybe too young or do not have the capacity to enter into … conversations like that because of the age groups that we see. But the older ones definitely are’ (Alexandra). Participants also reflected on how autistic voices are central in informing services. For example, relating to terminology that should be used in assessment, Charlotte argued that ‘you need to include autistic individuals in these conversations’.
Accessible assessments
Participants emphasised adapting assessment environments to make them accessible for children and young people. They discussed a variety of ways to do so. This includes the professional adopting a communicative approach that involves using accessible, clear language (‘we don’t use jargon’ (Emily); using ‘plain English’ (Lucy)) and being transparent about the assessment process. For example, Joe articulated that ‘we want to be absolutely transparent about where we are, what our next steps are, what we’re doing, kind of the reason we’ve reached any outcome we’ve reached, the information we’ve used’. Similarly, Linda argued that ‘the focus should be on… good communication, explaining to the child, being really clear on why they’re there’. Participants emphasised the need for a low-stress environment: ‘if they’re [children] feeling comfortable then they can, you know, relax and,-rather than coming into a… horrible environment where they might start to feel distressed or dysregulated’ (Brittany). Likewise, Nicola emphasised how ‘you want to get to see the child or young person in an environment that's comfortable for them’, rather than a setting that ‘might be feeding into anxiety’. Some highlighted how the clinic environment typically used for assessments is stressful, linking this to sensory aspects: ‘we’ve got a clock on the clinic wall that ticks loudly… and it's like… on a sensory level, like, is this the best idea?’ (Emily). Along similar lines, Isaac linked the example of a fire alarm going off with the importance of having ‘a setting that's not overstimulating …you don’t want too much sensory stuff going on in the room’.
Discussion
Our study generates new insights into professionals’ perspectives on neurodiversity-affirmative autism diagnostic assessment. We identified four themes that overall capture a holistic, balanced, person-centred assessment that is not diagnosis-led.
Based on participants’ perspectives, our findings highlight the importance of a holistic assessment process, involving a balanced assessment of both strengths and needs. These findings support the importance of moving away from a deficit-focussed assessment to one that also includes assessing strengths (Abrahamson et al., 2021; Brown et al., 2021; Ratto et al., 2023; Rutherford et al., 2021). Our study suggests that assessing strengths, and consequently communicating this information may be beneficial in improving wellbeing within the diagnostic process itself, particularly for parents/caregivers. This supports previous research suggesting that highlighting strengths is important for parents/caregivers to have positive diagnostic assessment experiences (e.g. Crane et al., 2018; Makino et al., 2021).
As part of this balanced assessment, participants also highlighted using neutral or positive terminology that is consistent with the neurodiversity paradigm (Brown et al., 2021). This supports wider calls to shift away from deficit-focused, ableist language in describing autistic experiences (e.g. Bottema-Beutel et al., 2021). Language is performative, and so using more positive language may benefit autistic people's wellbeing (Bottema-Beutel et al., 2021; Pearson & Rose, 2021). Our findings support this as participants highlighted that assessing strengths (and consequently communicating this information) could be particularly beneficial for autistic children and young people's wellbeing beyond the assessment process. This finding regarding these long-term benefits is particularly notable and reinforces the importance of assessing strengths within diagnostic assessment.
Our findings also suggest that another key part of a holistic assessment process involves acknowledging the role of the environment, as participants reflected on the context-dependent nature of strengths and needs and relatedly, the importance of obtaining information from multiple settings, as well as the importance of assessing contextual strengths and needs within assessment. This contrasts with the current diagnostic model which focuses on deficits that reside solely within the person (APA, 2013; WHO, 2019). Whilst previous research has highlighted the context-dependent nature of autistic strengths (Russell et al., 2019), our findings suggest that this is important within the context of diagnostic assessment. Furthermore, our study highlights that assessments across multiple settings should focus on both (context-related) strengths and needs, rather than deficits as is the case within the current diagnostic model.
Broadly, as the way we conceptualise and assess autism is interlinked, our findings relating to the importance of a balanced assessment align with one of the core tenets of the neurodiversity paradigm that autism is a form of neurodivergence characterised by difficulties, differences and strengths (Dwyer, 2022; Kapp et al., 2013; Pellicano & den Houting, 2022; Walker, 2014). Along similar lines, our findings regarding the importance of considering the role of the environment align with the ecological/interactionist model of disability (Dwyer, 2022; Mandy, 2023; Shakespeare, 2013; Shakespeare & Watson, 2001) in terms of acknowledging how the environment shapes autistic experiences. As professionals highlighted the importance of both assessing strengths and needs and acknowledging the role of the environment, our findings are also consistent with the International Classification of Functioning, Disability and Health (ICF) framework, which captures a holistic understanding of individual strengths and needs related to functioning and health, as well as the role of the environment (Bölte, 2023).
Providing further support for the neurodiversity paradigm, in terms of the centrality of the autistic voice, our findings highlight the importance of an autistic person-centred assessment. According to professionals, this involves a collaborative relationship between the child or young person and professional, where the autistic voice is valued. Whilst most of the literature emphasises the importance of valuing parents as experts on their children during the diagnostic process (Abrahamson et al., 2021; Crane et al., 2018; Makino et al., 2021), our study suggests it is important to recognise children and young people as experts of their own experiences (Ratto et al., 2023). Our findings also suggest that professionals believe that seeking children and young people's perspectives, and the collaborative relationship, may be less appropriate with, for example, younger children. This is notable given that the voices of younger children or those with communication support needs tend to be excluded (den Houting, 2019; Lewis et al., 2024). Within diagnostic assessment, creative or play-based methods (Lewis et al., 2024) or other accommodations (e.g. use of augmentative and alternative communication (AAC); Doherty et al., 2023) could be made to support younger autistic people and/or those with communication support needs to take part in conversations. This is important in obtaining authentic understandings based on children and young people's experiences.
Our findings also suggest that it is important to ask autistic people what they want diagnostic assessment services to look like, as participants reflected on how central autistic voices are in informing services. This echoes much of the literature arguing for the value of participatory research (Pickard et al., 2022). It is difficult to determine from examining existing clinical guidelines exactly how much power autistic people have in decision making related to autism diagnostic service design and delivery. For example, it is unclear how well represented autistic people are in consultations conducted as part of developing or reviewing NICE guidelines (NICE, 2021b). It would be beneficial if, as standard, details are available about how each service meaningfully involves autistic people in service development, and how they respond to feedback. Our study suggests that participatory service development and research, using approaches such as co-production with autistic people, is warranted (NHS England, 2023; Rutherford et al., 2021). Our findings could also apply to involving children and young people in decision making around the assessment process itself. For example, a professional could describe different assessment options and offer choice to the child or young person (Pritchard-Rowe et al., 2024).
Aligning with a person-centred approach, participants also emphasised the importance of providing accessible environments. This included professionals adopting an accessible, clear communicative approach and the provision of a comfortable, low-stress physical environment, including one that caters to sensory needs. Our findings echo prior research that has highlighted the importance of professionals providing transparency, clarity and accessible physical environments within diagnostic assessment (Crane et al., 2018; Murphy et al., 2023) and healthcare environments more generally (e.g. Doherty et al., 2022, 2023; Shaw et al., 2024). Our study suggests that these are important within a holistic, balanced diagnostic assessment for children and young people.
Our findings suggest that diagnostic assessment may benefit from a move away from a diagnosis-led model to one that is strengths-and-needs-led. Whilst participants highlighted that parents/caregivers and young people want support with needs, they discussed how accessing support is often dependent on assessing needs or obtaining a diagnosis. Some participants discussed an alternative, more support-oriented, strengths-and-needs-led assessment approach, supporting the importance of needs-based support that is not dependent on a diagnosis (Abrahamson et al., 2021; Rutherford et al., 2021). Whilst much of the literature highlights the importance of post-diagnostic support (e.g. Crane et al., 2018), our findings suggest that more attention should be focused on providing within-assessment or pre-diagnostic support. This could be important for ensuring that autistic children and young people receive timely support. Alternatively, a strengths-and-needs-led approach may result in more positive experiences, which in turn makes it more likely that children and young people or parents/caregivers seek support.
Although participants emphasised how support should be based on needs, assessing strengths could be useful for informing support. According to NICE guidelines (2021a), psychosocial interventions that address ‘the core features of autism’ include play-based approaches to increase communication skills. In line with neurodiversity-affirmative practice, strengths could be maximised and embedded in intervention goals and processes (Murthi et al., 2023), in ways that do not attempt to ‘fix’ or ‘normalise’ autistic people (Dwyer, 2022; Pellicano & den Houting, 2022).
Strengths and limitations
One key strength of our study is that it is novel in exploring professionals’ views on how neurodiversity-affirmative approaches relate to diagnostic assessment. Another key strength is the involvement of autistic adults and parents/carers of autistic children in designing the interview schedule. However, given the importance of the autistic voice, this study would have been considerably strengthened by the inclusion of autistic people throughout all stages of the research. Relatedly, this study did not explore autistic views on this topic. Such research is important for ensuring that diagnostic services are informed by what autistic people think is important. Relatedly, asking the professionals who took part in our study whether they were autistic or not may have enriched the analysis. Furthermore, most of the professionals in our study worked within Community Paediatrics/Child Development Clinic services. It is unclear whether professionals who work in other services, such as Child and Adolescent Mental Health Services (CAMHS), would share similar views. Additionally, the sample is predominantly White. Thus, we lack an understanding of how professionals from ethnic minority groups view neurodiversity-affirmative autism diagnostic assessments.
Implications and conclusion
Overall, our findings contrast with the frequently deficit-focused approach of autism diagnostic assessment, which tends to view deficits as residing within individuals and prioritises outsider rather than autistic perspectives of autistic experiences. Instead, our findings align with key tenets of the neurodiversity paradigm that emphasise conceptualising autism in terms of difficulties, differences and strengths, the role of the environment in shaping autistic experiences, and the importance of centring autistic perspectives.
We now highlight key implications for future research and clinical practice. Future research could explore perspectives concerning neurodiversity-affirmative diagnostic assessments for adults. This is pertinent given that adults are increasingly seeking diagnosis and/or being diagnosed (Huang et al., 2020). Future research could also explore the perspectives of educational professionals, as they play a key role in assessing children and young people.
Our findings have clinical implications for conducting neurodiversity-affirmative diagnostic assessments. To create and implement a holistic, balanced, person-centred assessment that is strengths-and-needs-led, we acknowledge that more research (including larger scale, mixed methods or quantitative research) is required to substantiate our findings, as well as the need for resource-intensive system-level changes. For example, changes in pathway setups would be required for services to become needs-led, and changes to diagnostic criteria would be required so that formal assessment of strengths is included as part of regular clinical practice. Careful consideration is required over how these changes could be implemented, given that clinicians already face institutional pressures in the form of long waiting lists, stretched resources and time pressures (e.g. Hayes et al., 2022). However, there are some small initial steps that could be taken. A relatively low-resource change could be for professionals to use more neurodiversity-affirmative language when they talk about/to a child or young person and their families, including within written reports (see Bottema-Beutel et al., 2021; Brown et al., 2021). More accessible language could be used, including being transparent about what the diagnostic process entails. As diagnostic tools tend to focus on interpretating behaviour in relation to deficit-based criteria, informal assessments of strengths could be undertaken, and professionals could more often seek children and young people's perspectives relating to their strengths and needs. Where possible, changes to the assessment environment could take place to minimise stress (e.g. minimise use of bright lighting). Indeed, it would be prudent to adapt the Sensory needs, Predictability, Acceptance, Communication and Empathy (SPACE) framework for diagnostic settings (see Doherty et al., 2023).
In the longer term, the implementation of an ICF-based tool could be explored, as it is at an advanced stage of development, is strengths-and needs-led (rather than diagnostic), examines strengths and needs of the individual and considers the environment (Bölte, 2023). The United Kingdom could learn from other countries, such as Australia, which have diagnostic guidelines that include an assessment of functioning, including using the ICF (Whitehouse et al., 2018). However, it would be useful to explore the use of tools that have been developed (primarily) by autistic people and that prioritise autistic perspectives of their own experiences. One such example is the Self-Assessment of Autistic Traits (SAAT; Ratto et al., 2023), which includes assessment of strengths and needs and acknowledges the impact of environmental factors, such as stigma, on autistic people. Although the SAAT has not been designed as a diagnostic tool and is aimed at people aged 16 years or older, it may be worth exploring whether this could be adapted for use with children and young people within clinical contexts.
Our findings also have implications beyond autism, relating to other forms of neurodivergence, such as ADHD. Adopting a strengths-and-needs-led rather than diagnosis-led approach raises the question of whether diagnostic pathways would benefit from moving away from an autism-specific pathway, towards a broader neurodevelopmental pathway which focuses on creating a profile of each child or young person's strengths and needs (Male et al., 2023). Along these lines, professionals could adopt neurodiversity-affirmative practices, as outlined in this article, when assessing neurodivergent people, regardless of their diagnosis.
We have summarised our key recommendations for conducting neurodiversity-affirmative autism diagnostic assessments in Table 2.
Key recommendations for conducting neurodiversity-affirmative autism diagnostic assessments.
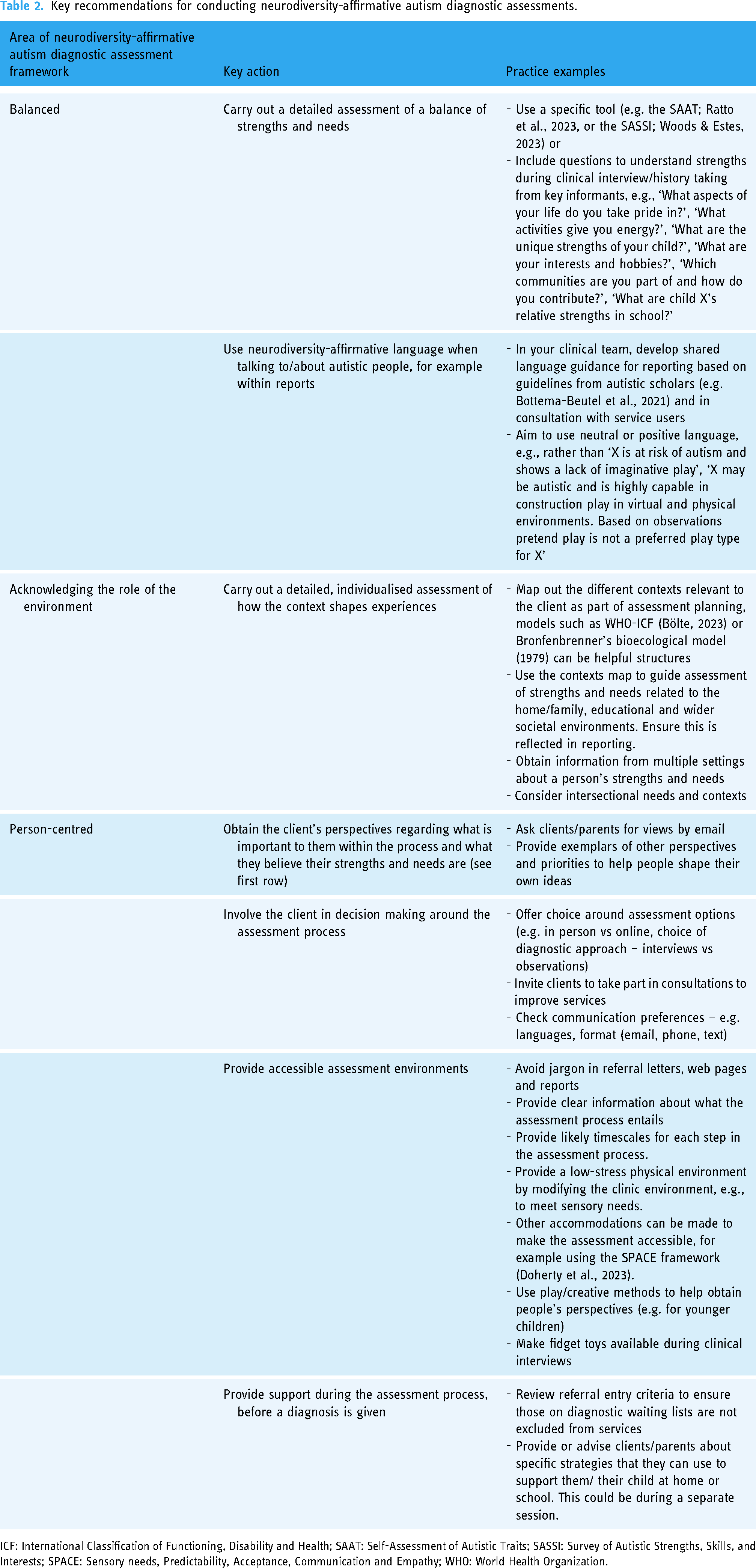
ICF: International Classification of Functioning, Disability and Health; SAAT: Self-Assessment of Autistic Traits; SASSI: Survey of Autistic Strengths, Skills, and Interests; SPACE: Sensory needs, Predictability, Acceptance, Communication and Empathy; WHO: World Health Organization.
Overall, changes toward neurodiversity-affirmative diagnostic practices, such as those outlined in this article, have the potential to result in more holistic understandings of children and young people, more positive assessment experiences and improved long-term wellbeing.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330241274674 - Supplemental material for Professionals’ perspectives on neurodiversity-affirmative autism diagnostic assessment
Supplemental material, sj-docx-1-ndy-10.1177_27546330241274674 for Professionals’ perspectives on neurodiversity-affirmative autism diagnostic assessment by Emma Pritchard-Rowe and Jenny Gibson in Neurodiversity
Supplemental Material
sj-docx-2-ndy-10.1177_27546330241274674 - Supplemental material for Professionals’ perspectives on neurodiversity-affirmative autism diagnostic assessment
Supplemental material, sj-docx-2-ndy-10.1177_27546330241274674 for Professionals’ perspectives on neurodiversity-affirmative autism diagnostic assessment by Emma Pritchard-Rowe and Jenny Gibson in Neurodiversity
Footnotes
Acknowledgments
We thank the consultants, those who were involved in piloting, and participants for giving their time to share their views.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cambridge Trust and the LEGO Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.