
Abstract
Purpose
Developing a positive neurodivergent identity is increasingly recognised as crucial for individuals’ well-being. As part of service improvement, we completed a qualitative investigation of the experiences of clinicians in a Child and Adolescent Mental Health Service Neurodevelopmental Conditions team providing support for autistic children's developing positive neurodivergent identity.
Methods
Nine semi-structured interviews with clinicians were held to explore their experiences of supporting children and young people's positive identity development. Interpretative Phenomenological Analysis was used to explore and understand clinicians’ experiences.
Results
Four superordinate themes were identified: (1) A flexible neuroaffirmative concept of positive autistic identity; (2) Being honest and balanced: acknowledging challenges for young autistic people; (3) Developing an identity through relationships with others; and (4) Professional vulnerability in navigating neurodivergent identities: The importance of self-reflexivity.
Conclusion
In line with our theoretical understanding of identity development, the child's network and environment was seen as crucial for their developing identity. In line with research into assimilating an identity as part of a neurominority, a flexible but neuroaffirmative approach was seen as vital. Novel clinical experiences included the need for staff support and reflective spaces to consider their own relationship to neurodiversity.
Lay Abstract
Research shows that viewing yourself positively (your identity) helps neurodivergent people to have better well-being overall. We wanted to understand what the professionals working with children and teenagers in an NHS child and adolescent mental health service think about supporting young autistic people to think positively about their identity as neurodivergent people, so that we could learn about what is helpful and what is challenging.
We interviewed nine people from different professions (such as doctors, psychologists and social workers) who worked in a team for autistic children and teenagers, asking the professionals about their experience of supporting the children and teenagers to develop positive beliefs about being autistic. We analysed the interviews using a method that helps us understand different people's experiences.
We found four main themes in the interviews: (1) Understanding and explaining autism and neurodivergence in flexible, positive ways; (2) Understanding how challenging it can be to grow up as an autistic young person; (3) Understanding the different people in a child's life who influence how they see themselves; and (4) Professionals needing to have time and support to think about their own relationship to neurodiversity.
Our findings fit with theories that explain how identity develops in childhood, with people around each child being important influences on how they see themselves. The findings fit with a need to hold positive views about autism and neurodivergence in society and in healthcare. We also found that staff may need more support and professional spaces to think about their own identity and relationship to neurodiversity.
Introduction
Neurodivergence is an umbrella term to refer to people whose neurodevelopment falls outside of (or ‘diverges’ from) the range usually considered to constitute ‘typical’ development, including being autistic (Pellicano & den Houting, 2022). Research concerning autistic identity development is relatively new, perhaps due to enduring misconceptions in wider narratives that autistic people have social ‘deficits’, thus denying experiences of autistic social awareness and consciousness. This may have led researchers to erroneously assume that forming a neurodivergent social identity is insignificant for autistic people, when it is quite the opposite (Botha & Gillespie-Lynch, 2022).
Social Identity Theory (SIT; Tajfel & Turner, 1979) suggests that individuals tend to categorise themselves and others into social groups, deriving a sense of identity and self-concept from group membership. This affiliation can contribute to well-being and self-esteem by providing a sense of belonging and shared meaning. Researchers have explored autistic identity development in relation to the stigma towards autism within society, demonstrating that experiences of discrimination, internalised stigma and masking one's autistic identity are associated with poorer mental health outcomes (Botha & Frost, 2020).
Nonetheless, individuals belonging to stigmatised groups can still develop a positive identity through collective self-esteem – a process of fostering positive views of their shared group identity and recognising the strengths and intrinsic value within that group (Cage et al., 2018). As has been soberingly highlighted by Botha and Cage (2022), professionals’ conceptualisations of autism significantly shape how autistic people are treated and understood – at worst, promoting cues for ableism, including dehumanisation and stigmatisation. The interactions that children have with professionals in diagnostic and support services, therefore, have important implications for identity development. Clinicians hold epistemic power via their language, assumptions and practice and can thus either reinforce stigma or support young people in forming a positive autistic identity.
The interface with clinicians and professionals is particularly relevant for children and young people (CYP), given how childhood and adolescence are periods of rapid development where an individual's environmental experiences can profoundly shape their developing perception of themselves, how they relate to others, and the world (Blakemore & Mills, 2014). Adolescence is a time of amplified cultural susceptibility and neurobiological change (Choudhury, 2010), where teenagers in particular are more sensitive to social environments and the attitudes and beliefs of others.
Neurodivergent CYP may often find themselves navigating multiple, and at times conflicting, socio-cultural discourses around neurodiversity. These range from deficit-based medical models that pathologise difference, to neuroaffirmative frameworks such as the neurodiversity movement, which frames autism, ADHD, dyslexia and other neurodivergence as valid and valuable forms of human diversity (Kapp et al., 2013). The neurodiversity perspective resists narratives of cure or correction, instead calling for societal acceptance and accessible environments (Kapp et al., 2013). Within this landscape, clinicians cannot remain neutral; their beliefs, language and practices inevitably influence how young people come to understand themselves (Miranda-Ojeda et al., 2025).
It is vital to consider intersectionality as well as solely autism, as overlapping identities influence how individuals experience marginalisation, access support and develop a sense of identity (Botha & Gillespie-Lynch, 2022). While learning that one is neurodivergent earlier and thus having earlier access to support and understanding is associated with better outcomes (Ashworth et al., 2025), intersectional factors including gender (specifically females and where there is gender diversity), not having a cognitive delay, people of the Global Majority, early life trauma and being from a lower socio-economic background can all lead to ‘later’ diagnosis of neurodivergence in adolescence where earlier identification opportunities were missed (Hosozawa et al., 2020; Kilmer et al., 2023; McQuaid et al., 2024; Pham & Charles, 2023).
Recognising intersectionality invites us to attend to the broader systemic and social contexts in which autistic identity is shaped – contexts where power, knowledge and cultural narratives intersect. Within these networks, identity is not formed in isolation but emerges through ongoing interactions with significant others and dominant discourses. A complementary theory to SIT suggests that identities develop over time through exchanges with salient social partners, including family members and professionals (Harter, 1999). The attitudes and beliefs held by those in a child's immediate environment play a key role in shaping how information about diagnosis is received and understood and can support well-being, self-acceptance and reduced self-stigma (Gillespie-Lynch et al., 2017).
Childhood and adolescence are also sensitive period for the onset and development of mental health challenges (Kessler et al., 2005). Neurodivergent CYP tends to have lower self-esteem and higher levels of depression and anxiety than CYP without neurodivergence (Strang et al., 2012; van der Cruijsen & Boyer, 2021). However, social identification with autism in CYP is positively associated with increased self-esteem, and this relationship is mediated by collective self-esteem – a perception of positivity associated with being autistic (Cooper et al., 2017). Developing a positive autistic identity can act as a protective factor for self-esteem and well-being (Davies et al., 2024). As such, being attuned to identity development is crucial for CYP mental health services, with important implications for clinical practice and support (Wilson et al., 2023).
Taken together, these findings highlight the importance of clinicians actively supporting the development of positive identities that include neurodivergence as a valued aspect of the self (Cooper et al., 2017). Emerging research has begun to explore professionals’ perspectives within UK multidisciplinary autism teams, suggesting that neuroaffirmative, holistic and strengths-based practices can foster autistic flourishing and support identity development (Pritchard-Rowe & Gibson, 2024). However, there remains a limited understanding of how clinicians themselves experience and makes sense of their role in shaping young people's emerging identities. Gaining insight into these perspectives is vital to enhancing clinical practice and improving the quality and impact of services.
Aims and Questions
Clinicians in the Oxfordshire Child and Adolescent Mental Health Service (CAMHS) Neurodevelopmental Conditions (NDC) service recognised the importance of supporting positive identity development for the CYP they work with. However, the service had not yet formally explored how well its current provision meets this need, or where service improvements could be made. Given the limited service-focused literature and absence of established standards in this area, this service improvement project aimed to explore clinicians’ lived experiences of facilitating positive identity development using semi-structured interviews and Interpretative Phenomenological Analysis (IPA). The study aimed to focus primarily on autistic young people, who represent the largest group seen in the service, though many of the young people discussed had multiple neurodivergent diagnoses and intersections of identities.
This project aimed to explore how clinicians made sense of their experiences supporting identity development, what they perceived as enabling or constraining within current service provision and how their reflections might inform a deeper understanding of clinical judgement and expertise in fostering positive identity development within neurodevelopmental services (Anderson et al., 2019).
Methods
Design
As an NHS service improvement initiative, our design was informed by the Institute for Healthcare Model for Improvement (IHI, 2020), matching the discovery phase: gathering information to understand the system and inform a future ‘Plan, Do, Study, Act’ cycle to implement and evaluate improvements.
We used a qualitative interview-based design, completing nine semi-structured interviews to explore the experiences of staff supporting positive identity development in CYP. We analysed transcribed data using IPA: an apt analytic approach when wishing to use a psychological perspective to explore how individuals may be ‘making sense’ of personal and social worlds from their particular position of power (Smith et al., 2009).
The service improvement project was conducted in the UK and was approved by Oxfordshire CAMHS Quality Improvement Hub, in accordance with NHS and Trust policies around ethics, audit and service improvement projects.
Service Context
The Oxfordshire CAMHS NDC Service is part of the Oxfordshire integrated CAMHS. The NDC service offers assessment for autism, ADHD and other NDC for children aged 5–18. If required, further support is offered to those requiring interventions for significant distress, such as psychological therapy, medication and/or contextual intervention (e.g., multi-agency liaison and advocacy). The service provides consultation to wider CAMHS teams and actively conducts research into optimising assessment/diagnostic/therapeutic practices in neurodivergent CYP.
The service serves a population of approximately 750,000 people, a fifth of whom are children, with just under 25% of residents from non-White British backgrounds (Office for National Statistics, 2022). The area is within the top 10% least deprived local authorities in England, marked by low unemployment and high educational attainment (Ministry of Housing Communities and Local Government, 2019). The area has a high proportion of young people with complex neurodevelopmental needs, and diagnostic assessment waiting lists exceeding national averages at present. The service is not commissioned to provide post-diagnostic support, so most CYP will receive a single feedback session from a clinician following assessment, while a minority of CYP will receive ongoing support – either psychological/contextual or for medication – where specialist neurodevelopmental support is indicated.
Participants
Interpretative Phenomenological Analysis is committed to an idiographic focus and suggests smaller, concentrated samples of 4–10 (Smith, 2004). The project was presented to the clinical team during a team meeting, and participants were asked to express interest via email. To meet the inclusion criteria, clinicians must have had experience of direct clinical work within the service for at least six months.
Measures
A semi-structured interview schedule was developed by the researchers, informed by lived experience of neurodivergence within the research team and building on existing research literature and accounting for different elements of service provision. The interview schedule comprised open, non-directive questions to facilitate and guide participant responses, allowing for an exploratory approach to be taken in line with IPA methodology. Beginning with a brief orientation to the key concepts – identity development and autistic identity development, we then asked questions about clinicians’ experience of working with neurodivergent CYP, and what is enjoyable and more difficult about the work. We asked clinicians what they noticed about developing identity for CYP, reflecting on specific clinical experiences and how they adapted their practice accordingly. We ended by asking about areas they felt less able to influence, influential team factors and barriers.
Some participants requested adaptations to be able to fully respond to questions, including seeing the questions in written form, which was facilitated. All interviews resulted in data that were useful to answer the research question.
Procedure
Participating clinicians were asked to meet for up to 60 min, through videoconferencing or in-person (depending on individual participant's preferences), to proceed through the semi-structured interview schedule. Informed consent was collected verbally and recorded at the interview. All interviews were conducted by the lead researcher. Two clinicians chose to be interviewed in person at their clinical base, and the remaining seven participants preferred to be interviewed online via videoconferencing. Interviews were audio recorded and lasted between 35 and 65 min.
Data Analysis
Initial questionnaire data was analysed using descriptive statistics, while verbatim transcripts from the semi-structured interviews were transcribed in line with IPA protocol, with all identifying information removed to ensure anonymity. The transcripts were then analysed using IPA to uncover latent themes in the data based upon participant accounts of their clinical experiences (Smith et al., 2009). Interpretative Phenomenological Analysis analytic processes were followed, using a close, line-by-line analysis of the transcripts, whilst analysing clinicians’ comments at the descriptive, linguistic and conceptual levels.
Following familiarisation with the data, initial observations and reflections were noted via ‘free coding’. Subsequently, close, line-by-line coding of the transcripts for objects of concern (what matters to the participant) and experiential claims (potential meanings of these objects) was completed. These codes were arranged into case-level summaries of emergent themes, with the researchers remaining open to adjusting these as the analysis progressed. The emergent themes at the case level were organised and reorganised into a structure of themes and sub-themes, representing patterns of meaning within the data and offering an interpretive view of these meanings. Themes were reviewed regularly to ensure they remained sufficiently grounded in the data.
To ensure quality and reflexivity, the lead researcher completed bracketing interviews prior to beginning data collection, and following completion, to explore preconceptions and blind spots. The lead researcher also kept a reflexive log throughout to continue to monitor assumptions and areas of interest, alongside regular supervision from co-researchers throughout the analysis, with an emphasis on ensuring the analysis remained grounded in the data. The lead researcher also conducted credibility checks for initial codes on several transcripts with co-researchers. Transcripts were coded independently, and any discrepancies in coding were discussed, and agreement reached.
Results
Nine participants took part in semi-structured interviews. The clinical profession of participants for the interview study included: Child and Adolescent Psychiatrist, Clinical Psychologist, Social Worker, Non-Medical Prescriber, Speech and Language Therapist and Mental Health Nurse. All participants had worked in the service for a minimum of 3 years. We do not report further demographic characteristics to maintain confidentiality.
Four superordinate themes were developed from analysis of the data, with between 4 and 13 subordinate themes each (Table 1). Between four and eight participants contributed to each superordinate theme (Appendix 3 and Table 2). Themes are discussed in detail below with illustrative quotes that ground them in participant experiences.
Structure of Superordinate and Subordinate Themes.
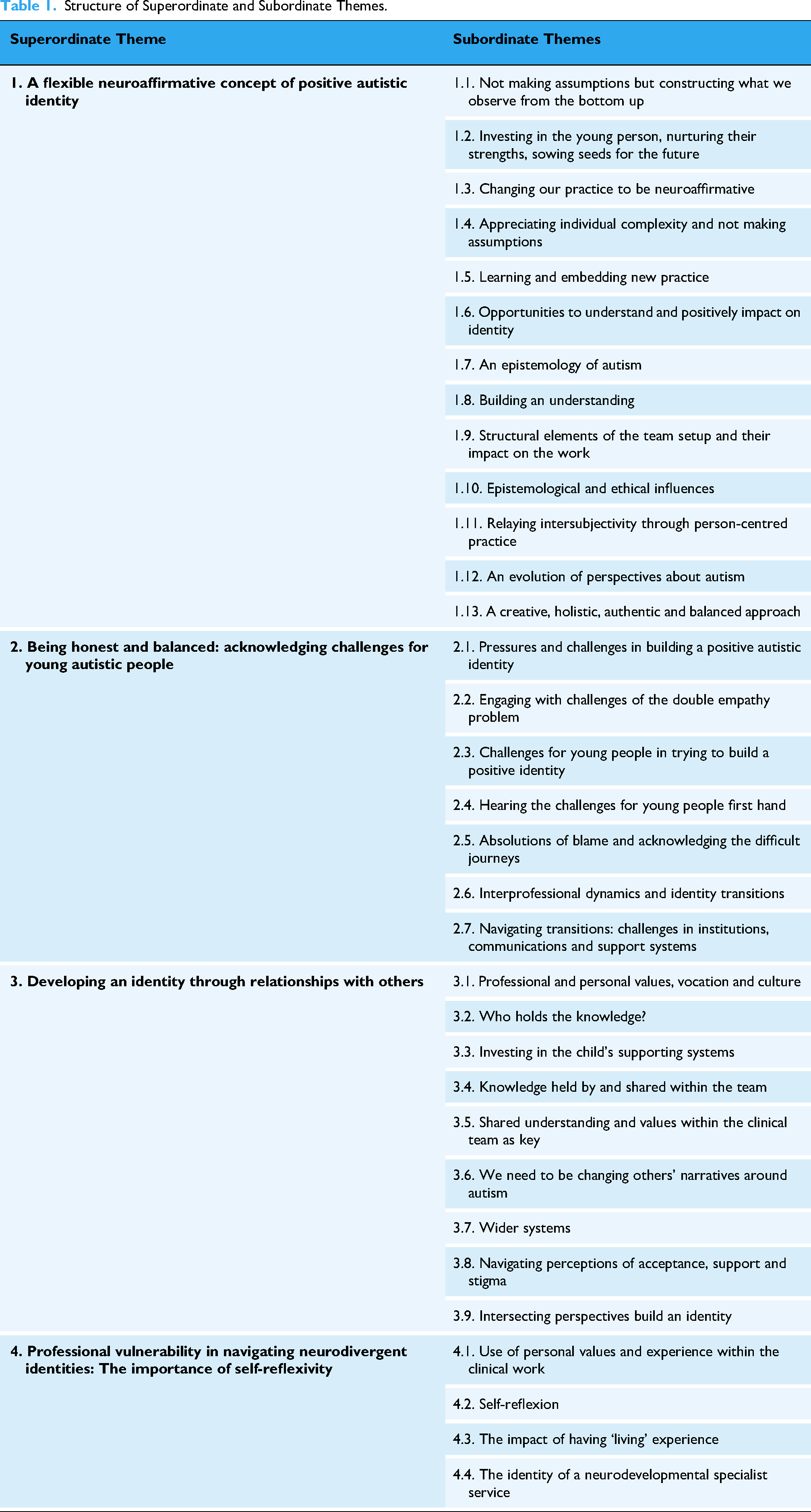
Theme 1: A Flexible Neuroaffirmative Concept of Positive Autistic Identity
This theme conveys how clinicians make sense of their role in nurturing positive autistic identity in CYP by holding a view of neurodivergence that is both flexible and neuroaffirmative. Clinicians described moving away from deficit-based, medical understandings towards a more nuanced appreciation and acceptance of neurodivergent ways of being – one that foregrounds strengths, validates difference and allows for a diversity of experiences. Clinicians’ accounts reflect a dynamic process of trying to hold space for positive identity to develop within systems and a society that often remains steeped in pathologising narratives. In this sense, clinicians positioned themselves not only as supporters of identity but as part of a cultural shift towards recognising and valuing neurodivergent experiences.
All participants spoke of their approach towards developing and holding a collective concept of positive autistic identity. There was a common recognition that our societal understanding of autism has rapidly expanded: ‘the thinking is always changing, isn't it still? If I think back ten years ago there was such a different kind of understanding of neurodiversity’ and that as clinicians, it has been important to them to keep up with change and reflect this with seeing the vast strengths within autism, using respectful language: I talk a lot about how I don’t want autism to be seen as anything negative and I talk about how everyone's got different brains. Then everyone's got, you know, everyone's got different strengths and skill sets. And just even the vocabulary and the language used around it – I think being in the team, it's so nice that people will sort of pull other people up and say, well, actually now it's this way instead. It's not in a bad way of pulling them up, you know, not shaming you and it's a way of saying, actually, this is the latest way now, it's helpful to say this instead. What I really enjoy the fact that it's so varied. That, you know, autistic people are just so different. And we can have a bit of an idea about what that might mean for them, but actually, part of what I enjoy is actually finding out what that does mean for them. I don't know whether all our knowledge is the same so I’m trying to be aware of the double empathy theory and not put everything from my perspective - the onus is two way. I like to get in there, in it with them, and be alongside them in the work. We do really care and that makes a huge difference. And through caring and kindness and really fighting the young person's corner, you end up getting more experience and understanding other people's points of view and we work together. It might not be explicit, it might be that I’m sowing kind of the seeds of how to think about yourself in that way – having that positive focus and moving away from problem-oriented talk. I feel very passionately about us trying to shift that narrative that is in wider society, particularly about pathologising these differences – that drives me insane when it happens for young people. It's like, these young people aren’t intentionally doing these things or avoiding this, this is the symptom of the world around them, and for me, that's my flag that I'm waving. I think is about trying not to pathologise these young people because ultimately that has such a negative impact on their identity because they start to think that they're unworthy, unlovable, you know, all of those really difficult, deep-rooted issues that then become mental health problems. And actually they aren't those things at all.
Theme 2: Being Honest and Balanced: Acknowledging Challenges for Young Autistic People
This theme reflects how clinicians made sense of the tensions between holding a positive, neuroaffirmative stance and witnessing the reality of significant challenges faced by autistic young people in today's society. These included the psychological impact of adversity, stigma and living in a world designed for neuronormative brains, as well as structural barriers within services. Clinicians described the emotional and ethical discomfort of wanting to do more to support identity development, while operating in and with systems that often constrained them to do so. This theme thus highlights the complexity of supporting identity in practice, the importance of validating negative influences upon identity and the need to hold both hope and realism.
Alongside holding a neuroaffirmative autistic concept, clinicians described the very real challenges for young autistic people in developing a positive identity. There was a shared acknowledgement of how many children who come to the service has low self-esteem, feel shame around feeling different from others and how many may see neurodivergence as ‘othering’. One clinician commented on how CYP can find it challenging to accept a diagnosis initially: ‘Quite sadly, I'd say the majority of the children that I've seen have been quite negative about their diagnosis or not wanting to accept it’. One clinician spoke of how the medicalisation of diagnostic processes can feel like it reduces epistemic agency and the ability for young people to define their own accepted, neurodivergent ways of being.
Clinicians also acknowledged how growing up feeling different without an understanding and acceptance of neurodivergence can be incredibly challenging: The young person said, ‘I feel like I'm the oil and all the other children are the water’, and so she just felt like she was really different but didn't know why. Her life had been really hard. The parents often come with their main concerns, and so we hear a lot about how school aren't meeting their needs or how they're really struggling to leave the house… so I guess I don't get a whole picture of that child, I only get to hear the really difficult bits that they're stuck on. If they are, you know, using drugs, in trouble with the police, excluded from school, hiding in their bedroom, then it's a very different situation to if they are actually in the classroom managing school, have one friend or two friends, then it's a very different way that you're then going to introduce the diagnosis. They want to fit in and they've got their group and so there's a sense they don't want to be different or stand out. I've had a handful of teenage boys that haven't wanted to relate to autism necessarily. We know that girls maybe mimic or copy others more. So, I think girls in particular have a more fragmented sense of who they are because they're copying bits from lots of others.
Clinicians reflected on how hard it can feel when working with other professionals who do not share a neuroaffirmative, inclusive understanding of autism: ‘I've come across other people, professionals, who are very resistant to understanding our own understanding of autism, and that's hard’. Clinicians spoke about wanting to advocate for young people within the systems around them, such as schools, by sharing personalised neuroaffirmative understandings of a child, but then finding it ‘hard to shift’ the prevailing views held there.
Concerning the NDC service, there were concerns raised about structural constraints due to high volumes of work for clinicians and a very long wait for diagnostic assessment for CYP (>4 years at present). Clinicians unanimously reflected on the tension they feel between wanting to see more children and potentially facilitate earlier understanding of their identities, while also being acutely aware of how current service constraints leave little room for increased efficiency to reduce the waiting lists that are growing by the day at faster rates. Clinicians hoped that commissioning of services nationally and locally could better appreciate the impact of long waiting lists on the well-being and education of children and families. Many of the young people who are waiting that feel a bit lost… don't quite know what's going on for them and are maybe not being well supported or well understood by those around them. I think that's probably where they're at higher risk of having mental health problems or being affected in a negative way. It's really important to try and get the service barriers down around waiting list times. [The one feedback session] can work for some young people, but I think for some, it's really tricky… they’ve waited for a long time and they might still have a million questions that people can't really answer. That's definitely a barrier to potentially then coming away and being confused and thinking badly of themselves or misunderstanding something that might feel negative.
Theme 3: Developing an Identity Through Relationships with Others
This theme explores how clinicians understand identity development as something that is not shaped in isolation but emerges through how others perceive, respond to and make meaning of their differences in relationships with family, peers, school environments and professionals. Clinicians spoke about witnessing identity being either supported or constrained by these relational dynamics. While feeling accepted by peers or at school can be an enabler, significant harm may be caused by misunderstanding, exclusion or invalidation. The conceptualisation of identity formation as a co-constructed process, shaped within interpersonal and systemic contexts, highlights the importance of fostering environments that affirm neurodivergence and allow young people to see themselves reflected positively in the eyes of others. I feel like identity is often shaped by the people around you. How people perceive you, and treat you, and what they tell you.
There were unanimous reflections from clinicians on the importance of feeling understood and accepted by other people: If you're understood, it makes a difference, doesn't it?
Diverse perspectives and the ability to challenge one another in the team were seen as positive qualities of the team's relationships: ‘There's some very thoughtful people in the team who will and can challenge each other. It's not a groupthink situation. So, we do debate, and we might have different points of view, which is good’. However, there were instances discussed where different perspectives within a CYP's family (e.g., between parents) can create additional challenges for a young person trying to build a coherent positive identity, and several clinicians saw their role as trying to navigate these multiple perspectives to try and see the young person authentically: What can be really difficult is if a young person is diagnosed as autistic and their parents are very resistant to that. And often I've had the scenario where one of the parents says ‘I've always known, absolutely, that they are autistic’ and then you get the other parent saying, ‘oh, don't be ridiculous, everyone has a label these days’, and then you get that repeated at home, which makes things really difficult. So in order to build a positive identity, I think those closest to you need to support you. That's part of our job, to tease it apart. If you've got one system saying I don't see any of that and then another one [seeing it], you know it's our job to really get to the bottom of that I think the biggest barrier is schools… we probably need to be a little bit more joined up… I know parents come to us and moan about schools and we join with them in moaning … I’m sure school staff will have their perspective as well and they will have their reasons as to why things are what they are … [we need to work towards] understanding each other a little bit and learning together, and providing more holistic thinking around the child. I've had a lot of young people saying, well, you know, I couldn't stim near my parents. Now that they know I'm autistic. And I know I'm autistic. That's what I do. And my parents accept it and it's fine.
Theme 4: Professional Vulnerability in Navigating Neurodivergent Identities: The Importance of Self-Reflexivity
This theme highlights clinicians’ vulnerability in navigating autistic identity alongside their own beliefs and experiences of neurodivergence. Participants emphasised the importance of ongoing self-reflexivity to remain aware, open and responsive. They recognised that their own perspectives may shape how they support young people's identities, making reflective practice vital for ethical and effective work. This theme was endorsed by fewer participants, but interpreted as significant within the experiences of this minority.
Clinicians spoke of being drawn to work in neurodevelopmental services based on their personal experience: At times, I guess I feel like it's not just a job for me. And I haven't stumbled into it by accident. My personal experience really drew me to this work. As I think that helps sustain me through the difficult bits. Just to note the positive impact that this work has on me, both as a clinician and a person, I think I've just learned so much from working with autistic people that I would never have thought about before. And I feel very privileged that I get to do that and that's what I want other people to feel. You know, when there's some fear or trepidation about autistic people. I want people to feel as I do, which is joyful and excited and hopeful. Does my lived experience make it more difficult? To do the work – I don't think it does. Not in any way that I can identify, I guess. I mean, I'm definitely more passionate about the work so maybe there is that kind of risk of, perhaps, of it feeling more personal or, you know, maybe I'm more invested in the things going well, compared to somebody else. We've got the external risks of othering mental illness or neurodiversity within the team. And, I mean, we've got some internal risks for those involved in facing their own neurodiversity at a point when they may not be ready. Maybe the next day I may reflect on it… Why didn't I pick this up when my child was younger? I do always say that if I had some help like this when I was younger, it would have been brilliant. And if I'd known all of this then. So I guess I do feel a bit guilty. And yeah, I do feel a bit vulnerable. …autistic identity is no different to me thinking about my identity as a woman or as a clinician or, you know, all of those layers that we have, and I guess they have different levels of importance to different people. And I think I'm more aware of that now than I might have been a few years ago. And how it actually changes as well. I go through phases where being a clinician is really important to me. And there's other times where I'm bit like, oh, you know, I'm a clinician, so what? And I think it might be similar to helping young people think about their autistic identity is trying to attune to where they're at in their journey with that and not being prescriptive, not trying to enforce them to reframe their identity if actually they're not in a place where they want to do that or are able to do that for some reason.
One participant spoke of the capacity for professional self-reflexivity as key for engendering professional humility, which they defined as ‘doesn't mean not being confident. It means holding a position of there being things that you don't know, and things that you still need to learn, and things that you can keep reflecting on’. It was a common experience for clinicians to be actively exploring their own identities, regardless of their number of years of clinical experience, perhaps demonstrating the iterative and continuous nature of understanding oneself.
Discussion
This service improvement project sought to explore how clinicians within the Oxfordshire CAMHS NDC service make sense of their role in supporting positive identity development in autistic young people. The findings offer rich, situated accounts that illuminate both the potential and the tensions within current clinical practice. In line with the idiographic and interpretative focus of IPA, the analysis highlights meaning-making processes of individual clinicians, while also raising important questions about how services conceptualise and respond to neurodivergent identities, including for clinicians themselves.
The findings support us in making sense of clinicians’ experiences in relation to the broader literature on autistic identity development, the role of professionals in shaping identity narratives and the wider systemic and cultural influences that frame this work. Through this interpretative engagement, we aim to deepen understanding of how our study contributes to neurodiversity-affirmative approaches, while also identifying areas for further research and service development.
Clinicians’ narratives offered rich insights into how they make sense of their role in supporting identity development in autistic CYP. Their accounts illuminated the layered complexities they encounter within clinical work: personally, professionally and systemically. Four themes were developed: (1) A flexible neuroaffirmative concept of positive autistic identity; (2) Being honest and balanced: acknowledging challenges for young autistic people; (3) Developing an identity through relationships with others; and (4) Professional vulnerability in navigating neurodivergent identities: The importance of self-reflexivity.
Our findings resonate strongly with theoretical models of identity development, and how clinicians have an important role in supporting collective autistic identity and belonging. The experiential evidence supports the view that identity formation is iterative and socially embedded (Harter, 1999), with clinicians highlighting the ongoing influence of family, peers, educators and healthcare professionals in reinforcing – or undermining – understanding of oneself over time. Clinicians described how a sense of shared understanding across a CYP's system – particularly when it embraced both the reality of challenges and joy in autistic strengths – could promote acceptance and belonging. This aligns with findings on the power of social affirmation in shaping identity (Cooper et al., 2017) and with SIT's emphasis on belonging to a valued in-group as a source of collective self-esteem (Cage et al., 2018).
The themes point to several significant implications, not only for how clinicians understand and engage with identity in neurodivergent young people but also for broader considerations on how neurodiversity is recognised, valued and meaningfully supported within and across services. Practices such as using neuroaffirmative language, becoming aware of and challenging stigmatising assumptions, validating and advocating for acceptance of autistic ways of being across multiple contexts such as family and school, emphasising neurodivergent strengths and facilitating autistic community connectedness (Cage et al., 2022) could all be strategies for clinicians to use when thinking of how CYP can internalise more positive self-concepts.
The findings highlight the powerful role clinicians can play as narrators of identity. While the clinicians unanimously displayed active resistance to deficit-based framings, there was also recognition that clinical settings can inadvertently reproduce reductionist and/or pathologising narratives of neurodivergence. This mirrors recent work maintaining that professionals must attend to how they construct and transmit meaning about autism and other neurotypes (Botha & Cage, 2022). Our findings extend this by showing how clinicians experience tension between their commitment to neuroaffirmative, individualised approaches and the demands of diagnostic language, service constraints and historical practices.
To manage this tension, clinicians may benefit from opportunities for active reflection and skills in raising awareness of our assumptions and biases. Clinicians spoke of the need for a flexible, values-based model of neuroaffirmative practice that can evolve alongside emerging language, community preferences and knowledge borne from autistic living experience. Reflective tools such as pre-hypothesising (Cecchin, 1987) have been adopted by the team since the service improvement project as ways of remaining open to prior assumptions and new meaning-making possibilities. This may support recognition of, and support for, autistic identities in CYP where there are less recognised intersections of identity, such as gender, culture and ethnicity and cognition.
Despite clinicians’ best intentions, systemic constraints were frequently described as limiting their capacity to support positive identity development. Long waiting lists, lack of post-diagnostic support and fragmented service provision were seen as significant barriers. This reflects wider critiques of CAMHS and other UK NHS services as often under-resourced and reactive (McGreevy et al., 2024). Clinicians expressed concern that without visible inclusion and sustained commitment from services, even the most neuroaffirming relational practices risk being undermined.
The findings call for policy-level changes that address not only access and resource gaps but also embed neurodiversity-informed frameworks across healthcare, education and public health. While individual clinicians may have limited power to influence systemic structures, they can contribute by collecting data on service inequities, advocating with and alongside families and resisting narratives that locate problems solely within the individual. Zooming out to effect wider systemic change while simultaneously staying zoomed in to take a personalised, neuroinclusive approach that adapts practice to uniqueness is vital (McGreevy et al., 2024).
Finally, our analysis accentuates the need for clinicians to consider identity not as a fixed trait but as a socially and structurally shaped experience. Clinicians repeatedly highlighted the importance of holding intersectionality in mind – recognising how autism may intersect with race, gender, socio-economic status, experiences of trauma and more – and how these complexities must be addressed to avoid simplistic or exclusionary narratives. This aligns with applications of the Minority Stress model to autistic health disparities (Botha & Frost, 2020), which emphasise how marginalised individuals face cumulative psychological burdens from stigma, discrimination and epistemic invisibility. Clinicians who held trauma-informed and compassion-focused perspectives described feeling better equipped to create space for young people to explore their identity on their own terms, suggesting that both of these lenses could be key in clinical practice, if appropriately adapted (Mason, Acland, Stark, Happé & Spain, 2023; Memmott, 2024).
These findings have implications beyond autism alone. A shared understanding that embraces both strengths and challenges of neurodivergence and the full diversity of intersections can help foster environments where all individuals feel accepted and supported, deconstructing the social construction that suggests a false dichotomy between ‘normal’ and ‘different’. To echo the sentiments of Botha and Gillespie-Lynch (2022), while dominant stereotypes frame autism as a condition of social withdrawal or isolation, the reality – and the future – lies in autistic people and their allies building communities across all domains of society in pursuit of acceptance, connection and inclusion.
We believe that drawing upon the phenomenology of experienced clinicians to understand their perceived impact on developing positive autistic identity in CYP accessing neurodevelopmental services is a crucial first step in discovering and gathering information to understand the system and inform future work. Interpretative Phenomenological Analysis focuses on exploring the individual experiences, personal meaning-making and subjective perspectives of clinicians and can thus allow for theoretical generalisability where readers can consider how the insights generated might resonate with or inform practice in other contexts (Smith et al., 2009). A limitation of methodology in this context is that we could not deeply explore the processes, tools and approaches used in diagnostic and support services, despite clinicians mentioning a need to examine practice around ‘gold standard’ tools and modalities such as PBS. Future service improvement work would benefit from critical appraisal of service-level tools, practices and processes, and the intersectionality within populations served.
Despite the value in clinician experience, a key limitation of this service improvement project was not hearing directly from autistic CYP, although clinicians spoke compassionately and thoughtfully of the experiences of children they have worked with, and the research team brought lived experience of neurodivergence to the work. Further investigation in this area should now focus on the experiences of additional key stakeholders, namely autistic CYP but also their parents and caregivers, siblings and practitioners in education and social care. Future service improvement initiatives would benefit from participatory approaches such as coproduction with young autistic people when designing and implementing service changes (Fletcher-Watson et al., 2019; Stark et al., 2021).
Footnotes
Acknowledgements
The authors would like to thank the clinicians within the Oxfordshire CAMHS NDC team who gave their time, passion and reflections for this service improvement project. The authors are especially grateful to the neurodivergent children and young people, and their parents and caregivers, whose everyday experiences guide and motivate our ongoing commitment to growth, change and meaningful practice.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.