
Abstract
Play is often included in autism diagnostic assessments. These tend to focus on ‘deficits’ and non-autistic interpretation of observable behaviours. In contrast, a neurodiversity-affirmative assessment approach involves centring autistic perspectives and focusing on strengths, differences and needs. Accordingly, this study was designed to focus on autistic perspectives of diagnostic assessments that incorporate play. Autism community stakeholders were consulted on the design of the study. Semi-structured interviews were conducted with 22 autistic adults aged 18–57 years who live in the United Kingdom. Interpretative phenomenological analysis was used to identify themes. Autistic adults highlighted the varying ways in which play was included in their diagnostic assessments, such as via the Autism Diagnostic Observation Schedule. Our findings highlight the importance of better adapting assessment to the heterogeneity of autism. For example, our findings question the extent to which play is useful for assessing autistic women and girls who mask. Our findings also suggest that holistic, neurodiversity-affirmative assessment practices should be adopted. Our findings support the importance of adopting a personalised approach to diagnostic assessments that use play, in addition to assessing strengths and differences as well as needs.
Lay abstract
Play is often included in autism diagnostic assessments. These assessments tend to focus on negatives and how people who are not autistic interpret observable behaviours. It is important to take a neurodiversity-affirmative assessment approach. This involves focusing on what autistic people say and looking at strengths and needs. We wanted to find out how autistic adults experience diagnostic assessments that include play. We asked autistic and non-autistic people to help us design our study and interview questions. We then interviewed 22 autistic adults to find out what they think about the use of play in assessments. We used a qualitative method called interpretative phenomenological analysis to analyse the data. Autistic adults told us about the different ways play was included in their diagnostic assessments. For example, some completed a diagnostic tool called the Autism Diagnostic Observation Schedule. Autistic adults also talked about the importance of considering how autistic people are different to each other. For example, we found that play may not be useful for assessing women or girls who mask. This suggests that professionals should adopt a personalised approach to diagnostic assessments that use play catering to each person’s needs. Our findings also suggested that professionals should assess strengths and differences as well as needs.
Introduction
Play is often included as part of autism-related assessments carried out by professionals. This tends to be based on the premise that play provides an insight into various aspects of child development, including social communication and interaction skills (Stagnitti, 2004). Furthermore, play experiences of autistic people may differ to those of non-autistic people (Pierucci et al., 2015; Pritchard-Rowe et al., 2023). The inclusion of play in diagnostic assessments generally reflects the centrality of play to childhood (Stagnitti, 2004) and how diagnostic assessments were developed predominantly for children, with adult diagnostic services only recently becoming more common (Russell et al., 2022). Furthermore, as autism is a lifelong way of being, adult diagnostic assessment involves examining both adult and childhood experiences (National Institute for Health and Care Excellence (NICE), 2021), meaning childhood play is likely to be included.
Current best practice guidelines for autism diagnostic assessment in the United Kingdom for children and young people detail a multidisciplinary assessment involving gathering various types of key information (NICE, 2017). Autism diagnostic assessment includes a detailed, conversation-based developmental history with parents/caregivers, and interaction- and observation-based assessment of the child’s behaviours that are considered in relation to diagnostic criteria (Lord et al., 2020). Similarly, autism diagnostic assessment for adults involves conversation- and observation-based assessment of behaviours in relation to diagnostic criteria, and a multidisciplinary autism team (NICE, 2021).
Within the context of autism diagnostic assessment for children or adults, observations and conversations about play (for example, via parental report) may be used (American Psychiatric Association (APA), 2013; NICE, 2017, 2021). For example, as a key assessment component, play is typically part of the Autism Diagnostic Observation Schedule (ADOS, Lord et al., 1999, 2012), which has been viewed as one of the ‘gold standard’ assessment tools (Falkmer et al., 2013; Hedley et al., 2016; Ozonoff et al., 2005). The ADOS, now in its second edition, is a semi-structured, standardised assessment, designed to elicit behaviour relevant to diagnostic criteria (APA, 2013). It contains both play and non-play activities, which are used as a basis to assess social communication and interaction and ‘restricted and repetitive behaviours’, as well as play activities that directly assess play skills themselves, such as functional and imaginative play (Lord et al., 2012). As such, it involves both the inclusion of play as a tool or context to identify autistic behaviours and assessment of autistic play skills. Examples of play-based activities in the ADOS-2 included in assessments for children and adults include the ‘Construction Task’, which involves completing a design using puzzle pieces and ‘Creating a Story’ using objects (Lord et al., 2012). There are also alternatives to the ADOS that include play items, such as The Diagnostic Interview for Social and Communication Disorders (DISCO, Wing et al., 2002), which is an interview-based diagnostic tool for children and adults. The DISCO includes items rated by clinicians after asking questions to informants which are related to social and pretend play. For example, the DISCO asks about delays in pretend play alone.
The inclusion of play within such assessments varies depending on age, with play being more central within childhood diagnostic assessments. This may reflect the common view that play is confined to, or at least primarily associated with childhood. However, increasingly it is recognised that play continues into adulthood (Van Vleet & Feeney, 2015). Relating to the ADOS, although ADOS module 4 (aimed at older adolescents and adults) contains play activities, these feature more heavily within modules 1–3 (primarily aimed at children or younger adolescents; Lord et al., 2012).
Although play often forms a key component of autism diagnostic assessment for children and adults, it tends to focus on identifying ‘deficits’, including the use of deficit-focused language. For example, the ADOS and childhood screening questionnaires such as the Social Communication Questionnaire (SCQ; Rutter et al., 2003) include items related to imaginary play and social play, where scores representing reduced frequency or absence of such behaviours indicate the presence or ‘severity’ of autistic ‘deficits’ or ‘symptoms’ (see Supplemental Material 1 for examples of deficit-based conceptualisations). These observable behaviours tend to be interpreted as deficits because they deviate from what neurotypical people consider to be ‘normal’ behaviours (Atherton et al., 2019; Gillespie-Lynch et al., 2017; Heasman & Gillespie, 2019; Jaswal & Akhtar, 2019). In addition to focusing on ‘deficits’, this means that in diagnostic assessment contexts, professionals focus on interpreting behaviours, including play, derived from non-autistic, rather than autistic views of what autistic behaviours are like. In doing so, such an approach also fails to address the double empathy problem (Milton, 2012) by overlooking possible neurotypical misinterpretations of autistic experiences. This approach reflects the dominance of the medical paradigm that underpins autism diagnostic assessment. According to this paradigm, autism is considered as a ‘disorder’ that is diagnosed based on meeting deficit-focussed diagnostic criteria (APA, 2013). These relate to ‘deficits’ in autistic traits, and diagnosis is dependent on ‘symptoms’ that lead to ‘impairment’ in areas of functioning related to daily life (APA, 2013).
In contrast to the frequently deficit-focused approach of the medical model, the neurodiversity paradigm argues for the importance of centring autistic perspectives and conceptualising autism as a form of neurodivergence characterised by difficulties, differences and strengths (Dwyer, 2022; Gillespie-Lynch et al., 2017; Kapp et al., 2013; Ne’eman, 2010; Robertson, 2010; Walker, 2014). In this sense, autism is not a ‘disorder’ that needs to be fixed or normalised but is conceptualised as a different way of being. As applied to childhood or adult autism diagnostic assessments, including assessments incorporating play, adopting a neurodiversity-affirmative approach would therefore involve understanding an autistic person and their play in a more holistic way by also considering neutral differences and strengths, and using more neutral or positive language. This is important given that ableist, deficit-focused language is linked to stigma, marginalisation and poorer mental health for autistic people (Bottema-Beutel et al., 2021; Pearson & Rose, 2021). Thus, adopting a more holistic perspective may be beneficial for autistic people’s wellbeing. Within diagnostic assessment contexts, avoiding focusing on ‘deficits’ could contribute to a more positive experience for autistic people and their families (Abbott et al., 2013; Anderberg & South, 2021; Crane et al., 2018; Makino et al., 2021; Mulligan et al., 2012; Nissenbaum et al., 2002).
However, it is worth noting that the current dominance of the medical paradigm presents significant barriers for professionals to provide positive, neurodiversity-affirmative assessment experiences for autistic people. Given that deficits are examined within the medical paradigm for diagnostic purposes, professionals may be limited to more informal assessments of differences and strengths. Future system-wide changes would be needed to replace the current deficit-focused diagnostic criteria with neurodiversity-affirmative criteria. Such changes are likely to be resource-intensive.
Key to improving diagnostic assessment experiences is to also focus on autistic perspectives, which is another aspect of a neurodiversity-affirmative approach. Focusing on autistic perspectives related to diagnostic assessments incorporating play can give useful insights, particularly as understandings of autistic behaviours, including play, that underpin assessment have tended to be based on non-autistic perspectives. Focusing on autistic views recognises that autistic people are experts of their own experiences and helps to shift existing power imbalances regarding knowledge creation that historically have been present in autism research (Botha, 2021; Howard et al., 2019; MacLeod, 2019). Furthermore, as autistic people have reported dissatisfaction with autism diagnostic assessment more generally (Crane et al., 2018; Jones et al., 2014), understanding autistic perspectives related to assessments incorporating play can give useful insights into how diagnostic services can be improved. As autistic adults have highlighted professionals’ tendency to focus solely on negatives as a barrier to satisfaction with the diagnostic process (Crane et al., 2018), this reinforces the need to adopt neurodiversity-affirmative assessment practices.
Research relating to diagnostic assessments incorporating play tends to focus on the diagnostic utility of tools like the ADOS (Falkmer et al., 2013; Mazefsky & Oswald, 2006). As far as the authors are aware, there is no published research focusing specifically on autistic perspectives and experiences relating to diagnostic assessments incorporating play. As discussed, this is an important topic area to investigate, which can help inform how professionals can better implement diagnostic assessments incorporating play in the future.
This study
This article reports on part of a neurodiversity-informed study that focused on exploring autistic perspectives and experiences of play and diagnostic assessments incorporating play administered by professionals (see https://osf.io/e8uvh). We focus on autistic experiences of diagnostic assessments incorporating play here (see Pritchard-Rowe et al., 2023 for experiences of play). We aimed to understand autistic adults’ experiences of diagnostic assessments incorporating play used by professionals. This study involved autistic adults who reflected on both their contemporary and childhood experiences. The research question was: What do autistic adults think about diagnostic assessments that incorporate play? We focused on commonly used assessments, which often involve comparisons to neurotypical norms. This study is conceptualised as neurodiversity-informed, with a view to informing neurodiversity-affirmative practice.
Methods
Methodology
This methods section is very similar to that of Pritchard-Rowe et al. (2023) because this study uses data from the same study. The focus of this article is to report on the results related to answering the research question: what do autistic adults think about diagnostic assessments that incorporate play? While the interview questions primarily focus on experiences of play, data were analysed across the whole interview, where relevant to the research question.
Ethical considerations
Ethical approval was awarded by the Faculty of Education Research Ethics Committee. Prior to data collection, participants provided written and verbal informed consent. Pseudonyms are used in this article to protect participants’ anonymity.
Methodological framework
We carried out a qualitative study using interpretative phenomenological analysis (IPA, Smith et al., 2009, 2021). With its emphasis on understanding individuals’ lived experiences, IPA is suited to the aims of this study. The suitability of this approach for experience-focused autism research has also been highlighted elsewhere (Howard et al., 2019; MacLeod, 2019). IPA aims to limit power imbalances through its emphasis on the individual as an expert of their own experiences. In addition, the researcher’s use of the ‘double hermeneutic’, in which researchers seek to make sense of participant’s own sense-making, promotes researcher reflexivity. We pre-registered the study on the Open Science Framework (OSF), and recorded changes to the pre-registration (https://osf.io/e8uvh).
Participants
Twenty-two autistic adults living in the United Kingdom aged 18–57 years (M = 39.00, SD = 11.39) were purposively recruited (see Table 1 for participant demographic information). Multiple strategies were adopted to recruit participants, including advertising via an autism research charity, advertisement on social media, and communication with autistic and non-autistic stakeholders that took part in a consultation (see ‘Community involvement’). Participants were not excluded if they had co-occurring conditions.
Participant demographic information.
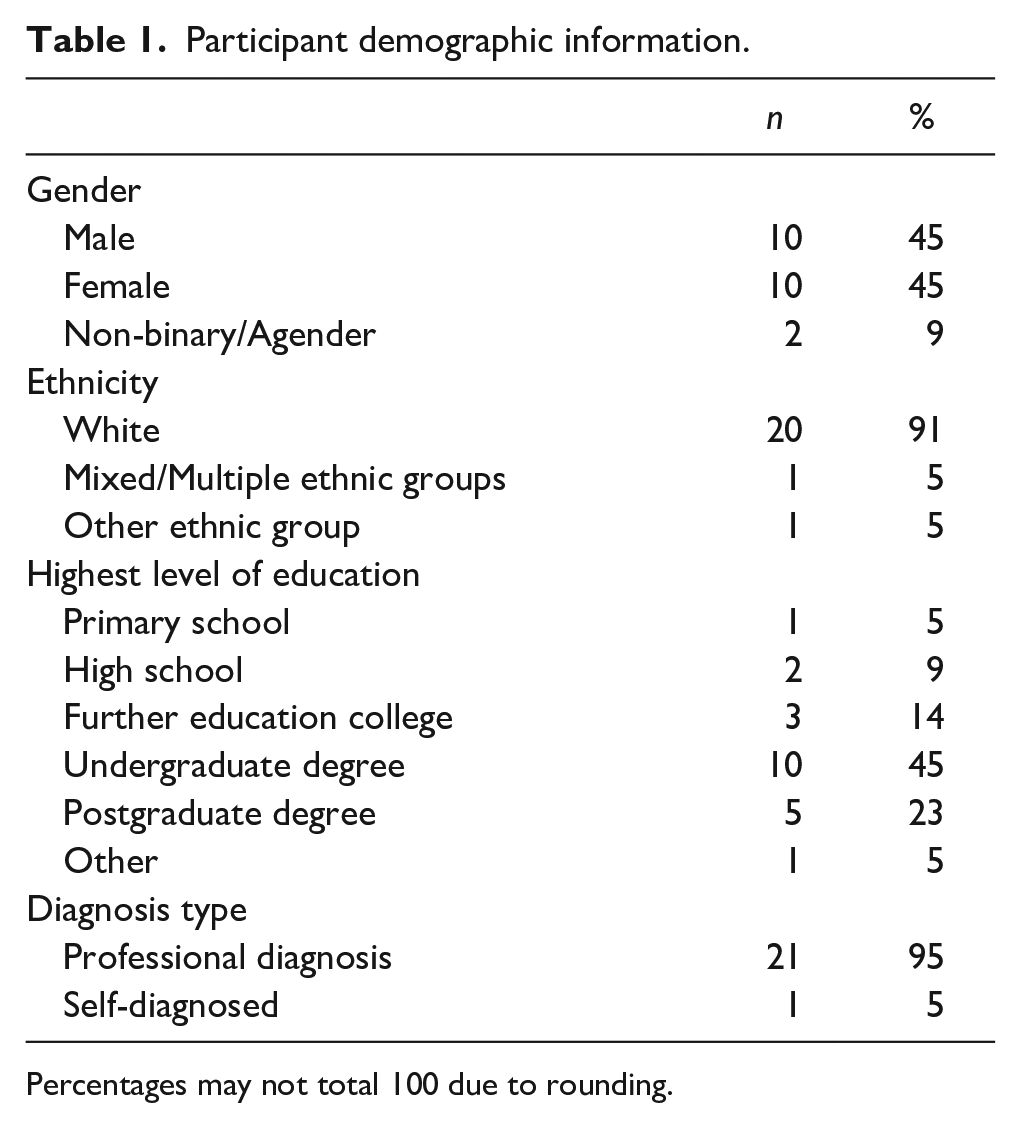
Percentages may not total 100 due to rounding.
Procedure
To investigate the aim and research question, participants took part in semi-structured interviews. These were conducted by the second author and, as per each participant’s preference, took place using either a written (email, Skype instant messenger) or verbal (phone, Zoom, Skype) format. Audio interviews were recorded. The interview procedures and design were informed by stakeholder consultation (see ‘Community involvement’). The interview questions related to experiences of play, comparisons between autistic and non-autistic play and experiences of assessment and supports using play (see Supplemental Material 2/https://osf.io/92gud/ for interview schedule). The participants were asked to consider both their contemporary and childhood experiences. Participants were emailed the interview guide in advance, which included a definition of play and examples. During the interviews, if required, participants were given further examples, including in relation to diagnostic assessment. The interviews were transcribed verbatim using NVivo 12 and transcripts were by the first author.
Data analysis
With the support of the other authors, the first author led the analysis. The analysis method was informed by team discussions and key IPA texts (Smith et al., 2009, 2021), particularly in relation to larger samples. An iterative analysis process involving the use of various software (NVivo 12, Miro, excel) was undertaken. An initial process of familiarisation took place, which involved making notes related to descriptive, linguistic and conceptual exploratory comments. These exploratory comments were subsequently summarised and developed into themes. After each transcript had been analysed following these steps, the analysis focused on identifying recurrent themes that were present across at least 50% of the transcripts. To create the master list of superordinate and subordinate themes, an iterative process of categorisation and reduction was undertaken. This involved identifying the most recurrent and ‘important’ superordinate themes, based on relevance to the research questions and to the wider context of the study as well as how frequently these themes occurred across participants’ experiences. However, in keeping with the idiographic nature of IPA, the authors sought to obtain a balance between convergence and divergence in participants’ accounts (Smith et al., 2009, 2021).
As part of the process, quality checks were conducted to maximise the trustworthiness (Lincoln & Guba, 1985) of the analysis. Similar themes were identified after independent analysis of one transcript by two of the researchers. Ongoing team discussions and revisions of the master list of themes took place. Transparency and reflexivity were enhanced by the first and second authors keeping a reflective diary, and the authors reflecting on their positionality (see Supplemental Material 3).
Community involvement
This study was informed by a consultation process involving autistic adults, parents of autistic people and professionals working with autistic people. Prior to data collection, a subset of this group was involved in a consultation focusing on the interview procedures and design. This took place using a private, online discussion forum. As part of the consultation, autistic adults and/or parents of autistic people were asked to comment on the suitability or understandability of pre-interview procedures relating to the demographic survey, information sheet and consent form. They were also asked to comment on the interview schedule, including specific questions and suitable supports or adjustments that could be made to support participants in sharing their experiences. More details can be found at https://osf.io/92gud/.
Results
Figure 1 shows the superordinate and subordinate themes, and based on the suggestions by Smith et al. (2009, 2021), the prevalence of the subordinate themes. The themes will be discussed and illustrated with supporting quotes. Exemplar quotes were selected to represent a range of different participants.
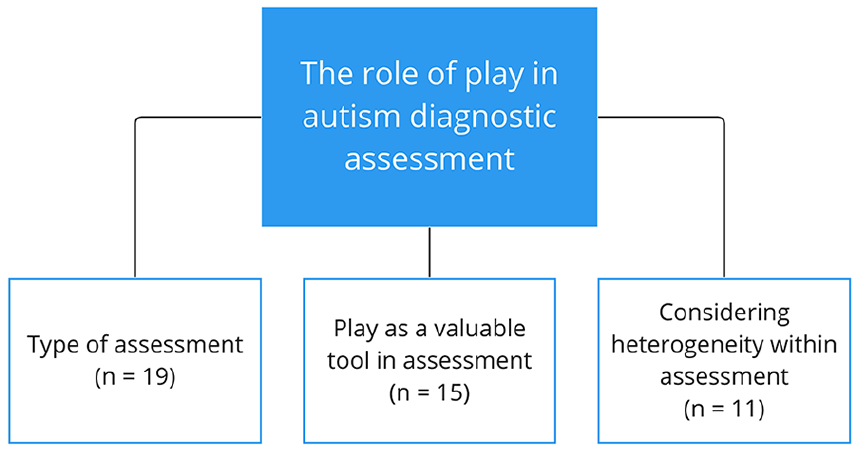
Overview of the superordinate theme, its subordinate themes and their prevalence.
Type of assessment
Most autistic adults described whether and how play was included in their experiences of diagnostic assessments administered by professionals and a variety of experiences emerged. Some had completed diagnostic assessments incorporating play including the ADOS or ADOS tasks. Kevin described one of the play-based tasks: ‘[it’s] got a different variety of objects so they might have like a toy car, a piece of string, a toy house for example . . . and they make you make a story out of them’. Kevin further articulated his understanding of the purpose of this story creation task: ‘I think they’re looking for your imagination’.
A few others described conversation-based diagnostic assessments that included discussions about their play. For Brianna and a few others, this involved professionals asking ‘questions about how I played as a child’.
There were also some autistic adults who had no experience of play in diagnostic assessment contexts, sometimes linking this to having been diagnosed as an adult: ‘obviously I was diagnosed aged ((late twenties)) so I haven’t had like assessment with a play aspect to it’ (Nathan). Interesting here is Nathan’s belief that ‘obviously’, play is only included in childhood assessments. Yet some others, such as Kevin, had experienced assessments incorporating play in adulthood.
Play as a valuable tool in assessment
Most participants discussed the value or potential value of using play in diagnostic assessments, particularly in differentiating between autistic and non-autistic people. Some autistic adults alluded to how play can give useful insights or information, relating to, for example, the autistic person’s play skills and thinking. For example, Matthew described how play is useful for ‘assessing how somebody’s brain is working’, and Amanda described how ‘people underestimate how much information they can gather from you’ in relation to the ADOS story creation task. Interestingly, these two participants referred to play as a context that promotes authenticity, with Matthew arguing that ‘play is actually quite a good way of determining how somebody reacts naturally to something’. In her description, Amanda suggests that play promotes authenticity in the sense of being herself, ‘spontaneous’ and ‘relaxed’: ‘it was an opportunity just to be totally myself because that’s exactly what they wanted to see, . . . this is you at your most spontaneous and relaxed really and I think they obviously find that useful, because if it wasn’t any use why would they get you to do that?’.
Here Amanda highlights that being authentic is beneficial for professionals as well as herself, and might be a useful tool in facilitating the assessment process, which can otherwise feel formal.
Demonstrating the potential value in using play in diagnostic assessments, many participants talked about play differences relative to non-autistic play that could be identified in this context. A variety of relevant differences were discussed, including those concerning the themes identified in relation to autistic adults’ play experiences (see Pritchard-Rowe et al., 2023 for more details). Some identified a flow state (Csikszentmihalyi, 2014), involving intense focus on the play, as a relevant difference. For example, Brianna described ‘how absorbed I get in something like when I’m playing . . . that might be a little clue that maybe an autistic brain was in here ((laughs))’. Here, Brianna indicates that flow could be an autistic play characteristic that may be useful diagnostically.
Some discussed differences in social play engagement as relevant, including being less social or more comfortable with solitary play. For example, Charles articulated that ‘if there would be any socialising, that would be a major identification factor’, particularly ‘if you have five, six, 10 play sessions in a group, and that kid is always doing stuff in his corner, then there is an issue’. For Charles, a child’s consistent preference for solitary play is important in identifying a child as autistic, supporting the use of play as a tool in assessment.
Some discussed imaginary play differences, such as preferring less creative or more literal forms of play. For example, Nathan described how he ‘enjoyed playing with LEGO sets but not really being creative with them’, further articulating how he ‘tended to enjoy assembling the kits following the instructions carefully, and reaching a final product there rather than you know using my own ingenuity’. Nathan reflected on the circumstance in which this difference could be useful: ‘maybe that’s something that could be used diagnostically if its common enough in autistic people’. Other play differences were described that might be of benefit to autism assessment, such as enjoyment of sensory aspects or sorting objects. For example, Amy highlighted, in relation to tactile play with sand, her expectation of an autistic child ‘enjoying the sensation of pouring it out or running it through fingers’. Amy also mentioned an autistic child’s LEGO play propensity to ‘sort the pieces into groups of colour or type’.
Some autistic adults pointed out the importance of assessing strengths or reframing ‘deficits’ as differences. This was discussed both generally and in relation to play more specifically. For example, Christine argued (in relation to play) ‘[it] would be really nice to kind of frame autistic difference rather than . . . deficit’. Similarly, Matthew articulated that ‘you just need to look at the strengths’ in (play) assessment, giving the example of his ‘focus on something . . . and not getting distracted’, or a flow state, as a strength that could be identified through play. This reinforces the use of play as a valuable tool, which professionals could use to identify autistic strengths. Lawrence argued that assessing for strengths in play-related ‘pattern recognition’ would be ‘something that an autistic child would take great pleasure in’, suggesting that assessing for strengths could contribute to a positive assessment experience.
Considering heterogeneity within assessment
Some participants alluded to autistic heterogeneity and its impact on whether and how play should be included in diagnostic assessment. For example, Fiona argued that variation between autistic people means it is ‘difficult to do a one size fits all’ approach and further articulated how play should be considered in assessment: I think it could be like when you’ve got a matrix of things that you’re judging, it could be [taken] into account but it certainly shouldn’t be a deciding factor because I think people’s experiences of autism are so different, that you can’t base a diagnosis solely on the play, certainly not the ability to socially play, because I’ve met autistic people who are fantastic socially, really terrible with sensory input, sensory overload.
Here, Fiona implies that it is important to consider heterogeneity and that (social) play should be one, but not the only component to consider in autism diagnosis.
As a dimension of heterogeneity, some discussed age as a relevant issue. For instance, Kevin suggested that the ADOS is inappropriate for assessing adults ‘because it’s so child-like and it’s not something that I would ever do and so it doesn’t assess my life if that makes sense, whereas for a child it might do’. Here Kevin suggests the ADOS is irrelevant. Along the lines of play being more appropriate for children, as implied by Nathan earlier (see ‘Type of assessment’), Matthew argued that play is useful ‘in particular with children, where they’re not necessarily able to analyse how they feel or events and how things have happened’. In contrast, Amanda argued that the ADOS is appropriate for adults: ‘to me, if something works, then it doesn’t matter whether it’s telling a story from a series of pictures, or something that might be more adult’ and described how she enjoyed how ‘it was like being a little kid again’. Overall, these quotations reveal the disparate views on whether play is appropriate for adult assessments.
Gender was also raised as a relevant issue. Susan pointed out difficulties in identifying ‘subtle differences’ that may be characteristic of some autistic women’s or girls’ play: Their play may look more similar to [neurotypical] play, e.g. they may still be interested in My Little Pony, or something stereotypically female, but the reasons for and the quality of their play may differ. So that’s harder to identify if you aren’t looking for it, especially in childhood when the service user may not be as self-aware as an adult, and able to specify the differences themselves.
Susan implies that a verbal component is important in assessing autistic women or girls, though she highlights that age is important to consider as it might be harder for children to verbalise these ‘subtle differences’. Susan further articulated that ‘I was assessed with the ADOS, but I know ((autism service)) uses the DISCO, so maybe that is better at identifying more subtle differences in play’, implying that the ADOS is insufficient in identifying such ‘subtle differences’.
Both Susan and Fiona also raised the issue of masking. Susan stated that, in relation to the aforementioned ‘subtle differences’, ‘masking can interfere with this identification of differences as well’. Fiona also recognised this as an issue that is particularly relevant to autistic women or girls and discussed how ‘masking to try and socially fit in’ resulted in a ‘huge disparity for me for how I feel inside and how I mask on the outside with play’. These quotations suggest that certain play observations may be misleading for professionals. As a result, Fiona recommended that professionals ‘take into account verbal responses from the child, from parent, from guardian, from teachers’. This supports Susan’s earlier implication regarding the importance of a verbal component.
Discussion
Through focusing on autistic perspectives, our findings generate new insight into what autistic adults think about diagnostic assessments that incorporate play.
Overall, our findings reveal the importance of considering heterogeneity of participant preferences in relation to diagnostic assessments incorporating play, in several ways.
Our findings demonstrate the diversity of experiences relating to the ways in which play was included in diagnostic assessments. Some autistic adults had no experience of assessments incorporating play, whereas others completed diagnostic assessments that include play, such as the ADOS, despite being diagnosed as an adult. Others discussed conversation-based assessments including conversations about their play. It is unsurprising that some participants completed (tasks from) the ADOS for diagnostic purposes, as it has often been cited as one of the ‘gold standard’ assessment tools, has been adapted for use in adults (Falkmer et al., 2013; Lord et al., 2012), and is one of the recommended tools for facilitating more complicated adult assessments within UK clinical guidelines (NICE, 2021). However, it is interesting to note the diversity in experiences. It is unclear why this may be the case; this might be due to variation between different services, such as in service pathways (Abrahamson et al., 2021). However, we did not collect this type of data so we cannot substantiate this. Our study supports other research documenting the diversity of experiences in diagnostic assessment, and reinforces the importance of providing clear, streamlined autism assessment pathways (Abrahamson et al., 2021; Crane et al., 2018; Evans et al., 2022; Jones et al., 2014; Wigham et al., 2022). This could involve adhering to best practice guidelines, in ways that allow tailoring for individual differences (Abrahamson et al., 2021; NICE, 2017, 2021; Whitehouse et al., 2018).
Our findings also give insight into the circumstances under which play may be useful in diagnostic assessments. While most autistic adults discussed the value of using play in diagnostic assessment, our findings suggest it is important to consider autistic heterogeneity and its impact on whether and how play should be included in diagnostic assessments.
One consideration relates to age. Participants in our study held disparate views on whether play, including the ADOS, was appropriate in the assessment of autism in adulthood. While some suggested that play was more suitable for use with children, one participant described their enjoyment of the child-like nature of the ADOS.
The suggestion of the ADOS as inappropriate for use in adults is somewhat reminiscent of the finding by Crane et al. (2018) that participants including autistic adults highlighted that some materials used as part of the diagnostic process were inappropriate to their level and patronising, as well as a barrier to satisfaction with the diagnostic process. Our study specifically highlights the contrasting views on the ADOS’s appropriateness for use in adults. Although play is not restricted to childhood (Van Vleet & Feeney, 2015), our study suggests that it is unclear what the exact role of play within adult assessments should be. Future research could explore this further, including whether ADOS activities or materials may be adapted, or whether it may be more appropriate to ask adults to reflect on their childhood play. This is particularly important given the key role of autism-friendly and positive diagnostic and healthcare experiences for autistic people (Crane et al., 2018; Nicolaidis et al., 2014, 2015). Regardless, our findings suggest that professionals should be aware that some adults may feel that using play within assessments such as the ADOS is inappropriate, and this may impact on their assessment experience.
Another consideration relates to gender. While our findings highlighted that play might be a useful tool as part of diagnostic assessments because it promotes authenticity, a couple of autistic adults described issues related to assessing women or girls and masking, involving suppressing natural behaviours (Pearson & Rose, 2021). Being authentic within the context of an assessment that includes play may mean that individuals are less likely to mask, which may aid diagnosis (Milner et al., 2023). However, our study suggests that for some autistic women or girls whose play may look more like non-autistic play and who mask, observations of play (such as via the ADOS) may be misleading for professionals. Thus, using play may not aid diagnosis for these individuals. This finding is in line with literature demonstrating that masking is a diagnostic barrier for women or girls (Lockwood Estrin et al., 2021; Murphy et al., 2023), and supports research showing that professionals consider the ADOS to lack sensitivity when diagnosing autistic women or girls, because of masking (Hayes et al., 2021, 2022).
Our findings reinforce the importance of assessing and understanding subjective experience as part of diagnosis, for example, by asking autistic people about their experiences, including of masking (Lai et al., 2021; Lockwood Estrin et al., 2021; Perry et al., 2022; Ratto et al., 2023). This is particularly important in the context of diagnostic assessments incorporating play, for those whom observations of play may not be appropriate. As suggested by one of the participants, the DISCO (Wing et al., 2002) might be appropriate for assessing women or girls whose play looks like non-autistic play and who mask. As highlighted by Carrington et al. (2019), the DISCO examines masking, and because it is an interview-based tool, adults themselves are likely able to discuss any masking strategies. Further reinforcing the importance of verbal accounts in relation to masking, one of the participants suggested that obtaining verbal accounts from different people involved in the process (e.g. child, parent/carer, teacher), would be useful for professionals to consider. This might be particularly useful when assessing children who find it harder to verbalise their experiences. This is largely in line with best practice guidelines for childhood and adult assessments, which refer to obtaining the views of family members and the child/adult during the diagnostic process (NICE, 2017, 2021). Therefore, the DISCO, or a similar interview-based tool, may be useful in these ways and further research exploring this would be fruitful. It is important to note however, that revealing masking strategies might result in women or girls feeling vulnerable (Harmens et al., 2022), and so care is needed during the diagnostic process to minimise harm.
The points raised in relation to age and gender align with one of our participant’s views that, because of autistic heterogeneity, play should not be the sole or determining component to consider in deciding a diagnosis. This is in keeping with current assessment practices for children and adults, whereby play can form one (albeit important) part of autism assessment and the diagnostic criteria also relate to non-play characteristics (APA, 2013; Falkmer et al., 2013; NICE, 2017 2021). Overall, as suggested by one of our participants, our findings support the importance of considering heterogeneity. Instead of adopting a ‘one size fits all’ approach, we argue that a personalised approach catering to the unique needs of each individual is important in determining how play is included in diagnostic assessment (Nicolaidis et al., 2014, 2015; Wigham et al., 2022; Zwaigenbaum et al., 2021). For instance, it may be useful to prioritise subjective experiences, particularly when assessing women or girls.
Our study also reveals diversity in terms of play preferences and differences that could be relevant diagnostically. Several autistic adults described specific play differences compared to non-autistic play that could be identified in a diagnostic context. A variety of differences were mentioned, though some identified differences relating to some of the themes established in relation to autistic adults’ experiences of play (Pritchard-Rowe et al., 2023). Specifically, these differences include engagement in flow, preferring less social or more solitary play, and preferring less creative or more literal play (i.e. less pretence). While this suggests the value of using play in differentiating between autistic and non-autistic people, it is important to note that Pritchard-Rowe et al. (2023) also identified a range of play experiences, some of which contrast with the differences participants identified as relevant to assessment. For example, although some identified a preference for more literal play as a difference to consider in assessment, many participants described their engagement in imaginary play and the type of imaginary play they prefer (Pritchard-Rowe et al., 2023). Furthermore, many autistic adults valued social play as well as solitary play. Therefore, it would be useful for future research to focus on mapping a framework for addressing the heterogeneity of play preferences in assessment contexts, for both child and adult assessments.
Furthermore, our study supports the importance of adopting holistic, neurodiversity-affirmative practices in relation to diagnostic assessments incorporating play. Some participants discussed the importance of reframing ‘deficits’ as differences or assessing strengths within diagnostic assessments. This was discussed both generally and in relation to play more specifically. Our findings suggest that play could be used to identify autistic strengths. In addition, our findings generally support the importance of assessing strengths or reframing ‘deficits’ as more neutral differences in diagnostic assessments, including those that use play (Abrahamson et al., 2021; Brown et al., 2021; Rutherford et al., 2021). It was suggested that this may contribute to a more positive assessment experience, supporting previous research focusing on autistic adults’, parental/caregivers’ and professionals’ views relating to autism diagnostic assessment (Abbott et al., 2013; Anderberg & South, 2021; Crane et al., 2018; Makino et al., 2021; Mulligan et al., 2012; Nissenbaum et al., 2002).
A neurodiversity-affirmative assessment could include using play to assess both play and non-play strengths, differences and needs. These could relate to the aforementioned play differences participants identified or our findings on play experiences (Pritchard-Rowe et al., 2023). Within current assessments like the ADOS and SCQ, preferences for solitary and literal play may be captured. However, these are conceptualised in a deficit-focused manner. Thus, it may be fruitful to reframe their inclusion in assessments in line with a neurodiversity-affirmative framework. This could involve more positive rephrasing within the tools and their manuals. However, a fundamental change in the underpinnings of diagnostic assessment relating to the deficit-focused diagnostic criteria may be required.
In addition, while flow is not explicitly assessed in current measures, there may be opportunities to assess flow during ADOS activities. However, this may vary on an individual basis, as engagement in flow may depend on several factors, such as level of interest in the activities, how challenging the task is perceived to be and level of comfort within the assessment environment. Thus, conversation-based assessments related to flow may be more appropriate for some people. Future research is warranted regarding how best to assess these preferences outside of a deficit model. Furthermore, it would be useful to explore whether neurodiversity-affirmative assessments may ‘look’ different depending on whether they take place in childhood or adulthood.
Strengths and limitations
Methodologically, the focus on autistic perspectives and involvement of autism community stakeholders in the study design are strengths of the study. The study is also innovative in exploring autistic views on how play relates to diagnostic assessment.
However, there are also limitations worthy of consideration. We did not collect specific background information relating to the assessments participants completed, such as the age at which participants completed assessments or were diagnosed, and relatedly, the assessments that participants completed. This is a limitation of our study as these may have influenced participants’ perspectives. Our participants were almost all professionally diagnosed. As there are many barriers to obtaining a professional diagnosis (Wilson et al., 2023), it is unclear whether self-diagnosed people share similar views. In addition, our study did not explore the views of non-speaking autistic people regarding diagnostic assessments incorporating play.
Implications and conclusion
This research highlights the varying perspectives autistic adults held concerning diagnostic assessments incorporating play. While play may provide useful insights in a diagnostic context, it is important to consider autistic heterogeneity, particularly in relation to age and gender. These findings suggest the importance of adopting a personalised approach to assessment, involving careful consideration regarding the circumstances under which play should be used and how it should be used. This is important for ensuring an accurate picture of an individual’s diagnostic profile and promoting a positive assessment experience.
Our findings also highlight the importance of countering the deficit-focused nature of diagnostic assessment by assessing strengths, differences and needs within diagnostic assessments incorporating play. Overall, through focusing on autistic perspectives, our study generates new insights into autistic views concerning assessments incorporating play, providing a useful platform for further research to build upon.
Future research exploring this topic involving a greater number of autistic people, including those of different ethnic and educational backgrounds, would be beneficial to substantiate our findings. In addition, research focusing on the circumstances under which assessments using play are appropriate or for whom such assessments are more appropriate, and the role of subjective experience in such assessments, would be valuable.
Our findings have implications for clinical practice. It is important for professionals to consider carefully how they include and assess play within diagnostic assessments, depending on the specific needs of each individual being assessed. Depending on the age and/or specific support needs of an individual, a personalised approach could involve collaborating with each individual to co-construct the assessment process, with the individual given choice around preferred assessment methods. For example, a plan of the proposed assessment procedures could be co-constructed in advance involving professionals providing detailed information about the different assessment options so the individual can make informed choices. For example, professionals could inform the individual in advance about the child-like nature of the ADOS and provide choice about whether to proceed with this method or choose an alternative, such as a conversation-based assessment. Furthermore, it is important for diagnostic assessments incorporating play to include assessment of strengths and differences as well as needs. For instance, professionals could include conversations around engagement in flow, and use more neutral or positive language within assessments. These changes could result in more holistic understandings of a person, including their play, and improve assessment experiences. A personalised, co-constructed approach could ensure that autistic voices are centred, and that diagnostic assessments incorporating play best cater to autistic people’s needs.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241257601 – Supplemental material for Autistic adults’ perspectives and experiences of diagnostic assessments that include play across the lifespan
Supplemental material, sj-docx-1-aut-10.1177_13623613241257601 for Autistic adults’ perspectives and experiences of diagnostic assessments that include play across the lifespan by Emma Pritchard-Rowe, Carmen de Lemos, Katie Howard and Jenny Gibson in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613241257601 – Supplemental material for Autistic adults’ perspectives and experiences of diagnostic assessments that include play across the lifespan
Supplemental material, sj-docx-2-aut-10.1177_13623613241257601 for Autistic adults’ perspectives and experiences of diagnostic assessments that include play across the lifespan by Emma Pritchard-Rowe, Carmen de Lemos, Katie Howard and Jenny Gibson in Autism
Supplemental Material
sj-docx-3-aut-10.1177_13623613241257601 – Supplemental material for Autistic adults’ perspectives and experiences of diagnostic assessments that include play across the lifespan
Supplemental material, sj-docx-3-aut-10.1177_13623613241257601 for Autistic adults’ perspectives and experiences of diagnostic assessments that include play across the lifespan by Emma Pritchard-Rowe, Carmen de Lemos, Katie Howard and Jenny Gibson in Autism
Footnotes
Acknowledgements
We thank all who were involved in the consultation(s) and participants for giving their time to share their views and experiences. We thank the Autistica Network for helping us to recruit consultants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cambridge Trust and the LEGO Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.