
Abstract
Aim
To provide detailed descriptions of the amount of daily physical activity (PA) performed by people with multimorbidity and investigate the association between the number of conditions, multimorbidity profiles, and PA.
Methods
All adults (≥18 years) from The Lolland-Falster Health Study, conducted from 2016 to 2020, who had PA measured with accelerometers and reported medical conditions were included (n=2,158). Sedentary behavior and daily PA at light, moderate, vigorous, and moderate to vigorous intensity and number of steps were measured with two accelerometers. Associations were investigated using multivariable and quantile regression analyses.
Results
Adults with multimorbidity spent nearly half their day sedentary, and the majority did not adhere to the World Health Organization’s (WHO) PA recommendations (two conditions: 63%, three conditions: 74%, ≥four conditions: 81%). Number of conditions was inversely associated with both PA for all intensity levels except sedentary time and daily number of steps. Participants with multimorbidity and presence of mental disorders (somatic/mental multimorbidity) had significantly lower levels of PA at all intensity levels, except sedentary time, and number of daily steps, compared to participants with multimorbidity combinations of exclusively somatic conditions.
Conclusion
Levels of sedentary behavior and non-adherence to PA recommendations in adults with multimorbidity were high. Inverse associations between PA and the number of conditions and mental multimorbidity profiles suggest that physical inactivity increases as multimorbidity becomes more complex.
Introduction
The global burden of physical inactivity is substantial, with an annual global health-care cost of $53.8 billion, and disability-adjusted life-years attributable to physical inactivity of 13.4 million. 1 In contrast to this, regular engagement in physical activity (PA) is associated with numerous positive health outcomes, such as reduced risk of mortality 2 and prevention of a range of chronic conditions. 3 Furthermore, PA is effective as a treatment for 26 different chronic conditions 4 and is also safe and beneficial in people with multiple chronic conditions, commonly referred to as multimorbidity. 5
To achieve significant health benefits, The World Health Organization (WHO) recommends that adults perform at least 150 minutes of aerobic PA at moderate intensity or at least 75 minutes of aerobic PA at a vigorous intensity (or an equivalent combination of moderate and vigorous intensity) during the week. 6 Unfortunately, a large proportion of adults are insufficiently physically active. 7
The level of PA is lower in people with multimorbidity compared to the general population. 8 This constitutes a serious global health problem since the overall prevalence of multimorbidity is 37% 9 and projected to grow substantially in the future, 10 placing further strains on both population health and the economy. 11 This makes multimorbidity a global research priority according to the Academy of Medical Sciences and WHO.12,13
Previous studies have found an association between low levels of PA and multimorbidity.14–16 However, PA has predominantly been measured using self-reported methods, which are suggested to be less accurate compared to objective methods, such as accelerometers or other types of activity trackers17,18 due to factors such as social desirability and recall bias. 19 A recent systematic review and meta-analysis found that few studies, of low quality, have investigated PA in populations with multimorbidity using objective measurement methods. 20 Furthermore, few aspects of physical activity were described in the included studies, and these were not consistently reported across the studies. Specifically, only a small number of studies included data on all levels of intensity (e.g., light, moderate, and vigorous) of physical activity. Additionally, the studied populations were not representative of adults with multimorbidity. 20 Population-based studies of PA using objective measurement methods capable of reporting more aspects of PA behavior in multimorbid populations are therefore warranted.
Evidence suggests that the presence of mental health conditions in individuals with multimorbidity is associated with negative health outcomes and an extended length of stay during hospital admission.21–24 However, important aspects of behavioral determinants, such as PA, in individuals with mental health conditions and multimorbidity remain underexplored. To date no studies have yet investigated the association between mental disorder in multimorbidity and PA levels using objective measurement methods. 20 To better target specific sub-populations of people with multimorbidity when developing interventions with PA as a treatment component, valid PA data are warranted. In this study, we will describe the PA level at different intensities and the number of daily steps in adults with multimorbidity and investigate the association between the number of conditions and PA levels. Furthermore, we will investigate the difference in association between multimorbidity profiles with and without mental health conditions and PA levels.
Methods
Study design
This study used a cross-sectional design and was reported according to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines (Supplemental file 1). 25
Setting and study participants
Data used in the present study were derived from the Danish population-based study - The Lolland-Falster Health Study (LOFUS).26,27 LOFUS was designed to create a scientific research database from a disadvantaged mixed rural/provincial area consisting of the two municipalities of Guldborgsund and Lolland. 26 This area is disadvantaged, due to the relatively high prevalence of unemployment, low educational level and low income.
Inhabitants of all ages currently living in the municipality of Guldborgsund or Lolland were eligible for inclusion in LOFUS. Potential participants were identified by randomly selecting adults through the Danish Civil Registration System (CRS) and then sending them and their household members an invitation. The data collection in LOFUS was conducted from February 2016 to February 2020. In the present study, only adults who were 18 years or older were included.
Data collection
Data were collected through a self-administered questionnaire, a site visit where biological samples were collected, and a health examination. The questionnaire for adults (≥18 years) contained 299 items covering a vast variety of topics, e.g. mental health status, alcohol consumption, and work status. 27 In the present study, we used data from the health examination (weight and height) and the questionnaire (age, sex, socio-economic status (SES), civil status, employment status, mental well-being, chronic pain, and self-reported medical conditions). Furthermore, we used data from an add-on data collection of participants’ PA, which was measured with accelerometers. 28
Between February 2017 and November 2018, individuals who were able to walk and were part of families with at least one adult and one child were invited to participate in the accelerometer measurement as part of a cross-sectional study on physical activity resemblance in families. 28 From December 2018 to February 2020, recruitment was expanded to include all LOFUS participants who were able to walk, broadening the participant base to enhance inclusivity and generalizability.
Ethical permissions
Written informed consent was obtained from all participants, and LOFUS was approved by Region Zealand’s Ethical Committee on Health Research (SJ-421) and registered with the Danish Data Protection Agency (REG-024-2015) and Clinical Trials (NCT02482896). This study was registered with the Danish Data Protection Agency (REG-130-2020).
Variables
Definition of multimorbidity
Participants were defined as having multimorbidity if they reported having at least two conditions located in at least two different ‘body systems’. The body systems were formed by merging the original 18 condition response categories available in the LOFUS questionnaire into ten body system groups. Body systems were based on individual conditions’ similarities in treatment, clinical manifestation, or organization in the health-care system. This procedure has been used in previous studies,29,30 we, however, deviated slightly from this by including hypertension as a medical condition. In total, ten body systems were formed: 1) lung, 2) musculoskeletal, 3) endocrine, 4) mental, 5) cancer, 6) neurological, 7) gastrointestinal, 8) cardiovascular, 9) kidney, and 10) sensory organs (Supplemental file 2).
One of the response categories (response category 18) was a free text field entitled ‘others’. Here, participants could report condition(s) that were not already included among the response categories. Authors (LBJ and SRM), both with backgrounds in health science, individually assessed conditions and included them if they were clearly named and indicated as a medical condition, including the location. All conditions: 1) not defined as regular conditions (e.g., dizziness), 2) indicated as ‘former’ or 3) considered as risk factors were excluded. Disagreements between the two authors were discussed until consensus was reached, and conditions from the free text field could be placed in one of the ten body systems or be excluded.
Exposure variables
Number of conditions and mental multimorbidity profiles
The number of conditions and mental multimorbidity profile were used as exposure variables. The number of conditions was determined by the number of different body systems where a participant reported having a condition. One (or more) condition(s) from one body system was considered as one condition and one (or more) condition(s) from two body systems as multimorbidity.
The mental multimorbidity profile (somatic or somatic/mental multimorbidity) was determined by the presence/absence of a mental disorder in participants with multimorbidity. All participants who had reported a somatic medical condition from two body systems were classified as ‘somatic multimorbidity’. All participants who had reported mental disorders combined with somatic conditions were classified as ‘somatic/mental multimorbidity’. For example, a participant who reported both diabetes (a somatic condition from the endocrine system) and hypertension (a somatic condition from the cardiovascular system) would be classified as having ‘somatic multimorbidity’. On the other hand, a participant who reported both diabetes and depression (a mental disorder) would be classified as having ‘somatic/mental multimorbidity’
Outcome variables
Physical activity
The daily levels of PA were outcome variables. Levels were determined according to daily hours or minutes spent in sedentary behavior (SB), light (LPA), moderate (MPA), vigorous (VPA), and moderate-to-vigorous physical activity (MVPA) and daily number of steps. PA levels were assessed using two accelerometers (Axivity AX3, Newcastle, UK), which have earlier demonstrated to be valid when measuring PA in adults with and without functional impairments.31,32 The accelerometers were placed on the thigh and the lower back respectively, and worn 24 hours per day for seven consecutive days, including during sleep and water activities such as bathing or swimming. 33
The amount of time spent within each intensity domain was determined by generating ActiGraph counts from the accelerometer worn on the back using 10-second epochs, a procedure that has been validated in earlier studies.31,34 Measurements were considered valid for the present study if they included at least three valid weekdays and one valid weekend day (weighted by 5/7 for weekdays and 2/7 for weekends) with a ‘valid day’ being equivalent to a wear time of at least 22 out of 24 hours. Steps were determined from the raw acceleration (accelerometer worn on the back) using a similar method as described by Hickey et al. 35
Descriptive variables and co-variates
Participant characteristics were described using age, sex, Body Mass index (BMI), SES, civil status, employment status, mental well-being, chronic pain, and adherence to the WHO PA recommendations.
Data on age and sex were derived from CRS
BMI (kg/m2) was calculated using measures of height and weight obtained at the health examination. Height was measured with a SECA 216 wall-mounted height measure and weight with a Tanita Body Composition Analyzer (BC-420MA III) or electronic scales (Tanita WB 150 SMA). 26
Data on SES, civil status, employment status, mental well-being, and chronic pain (pain lasting for six months or more) were self-reported and derived from the LOFUS questionnaire.
Data on mental well-being were obtained using the World Health Organization Well-Being Index (WHO-5). 36 The WHO-5 consists of five items asking respondents to rate their emotional state over the past 14 days, including feelings of happiness, calmness, and overall well-being. Scores range from 0 to 100, with higher scores indicating better mental well-being.
Adherence to WHO PA recommendations was determined based on accelerometer data using the time spent in MPA and/or VPA. Adherence was defined as performing at least 150 minutes of MVPA per week (corresponding to a mean of ≥22 minutes per day) with MVPA being calculated using the formula: MPA+ (VPA*2) = MVPA.
Data management and analysis
Sample and transformation of data
All adults with valid accelerometer data were included. For the descriptive statistics and analysis of associations between the number of conditions and PA, participants were divided into four groups according to their number of conditions (body systems); 1) One, 2) Two, 3) Three, or 4) ≥Four conditions.
For the analysis of associations between multimorbidity profile and PA, participants with multimorbidity were divided into two groups, according to the absence or presence of a mental disorder in multimorbidity; 1) Somatic multimorbidity or 2) Somatic/mental multimorbidity.
Data on SES were divided into four categories: 1) Primary educational level (<10 years), 2) Upper secondary or vocational level (10-12 years), 3) Higher educational level (≥13 years), 4) Other. Data on civil status were split into two categories: 1) Married/living with a partner, 2) Living alone. Employment status was split into four categories: 1) ‘Employed’, 2) ‘Unemployed’, 3) ‘Retired’, and 4) ‘Other’.
The mental well-being score was split into two categories: 1) ‘Low’ (score <50) and 2) ‘Moderate to high’ (score ≥50).
Statistical analysis
Inspection of data, calculations, and analyses were done using the statistical software STATA/BE 17. Before conducting the analyses, a statistical analysis plan was drafted and made publicly available via Open Science Framework (OSF) (https://osf.io/aqmve/?view_only=c63cdcee33274dd49f45578a871465ce). QQ plots revealed a non-normal distribution of residuals for the PA levels MPA, VPA, and MVPA and the number of daily steps. We were therefore unable to perform multiple linear regression at these levels as described in the analysis plan. Multiple linear regression was therefore performed to estimate the associations between i) the number of conditions (with one condition as the reference) and ii) somatic/mental multimorbidity (with somatic multimorbidity as the reference) and PA at PA levels SB and LPA only. For the remaining PA levels (MPA, VPA, and MVPA) and number of steps, quantile regression analyses were performed.
Four analysis models were conducted: unadjusted (model 1), adjusted for sex and age (model 2), adjusted for sex, age, BMI, SES, and civil status (model 3) and adjusted for sex, age, and SES (model 4). The confounders used in the models were identified by drawing directed acyclic graphs (DAGs) (Supplemental file 3-4) using the web-based software DAGitty. 37
Results
Participant characteristics
In LOFUS, 7,208 adult participants were invited to wear accelerometers. Valid accelerometer data and data on conditions were available in 2,158 participants, of which 1,172 had multimorbidity (Figure 1). Shows the flow of participants.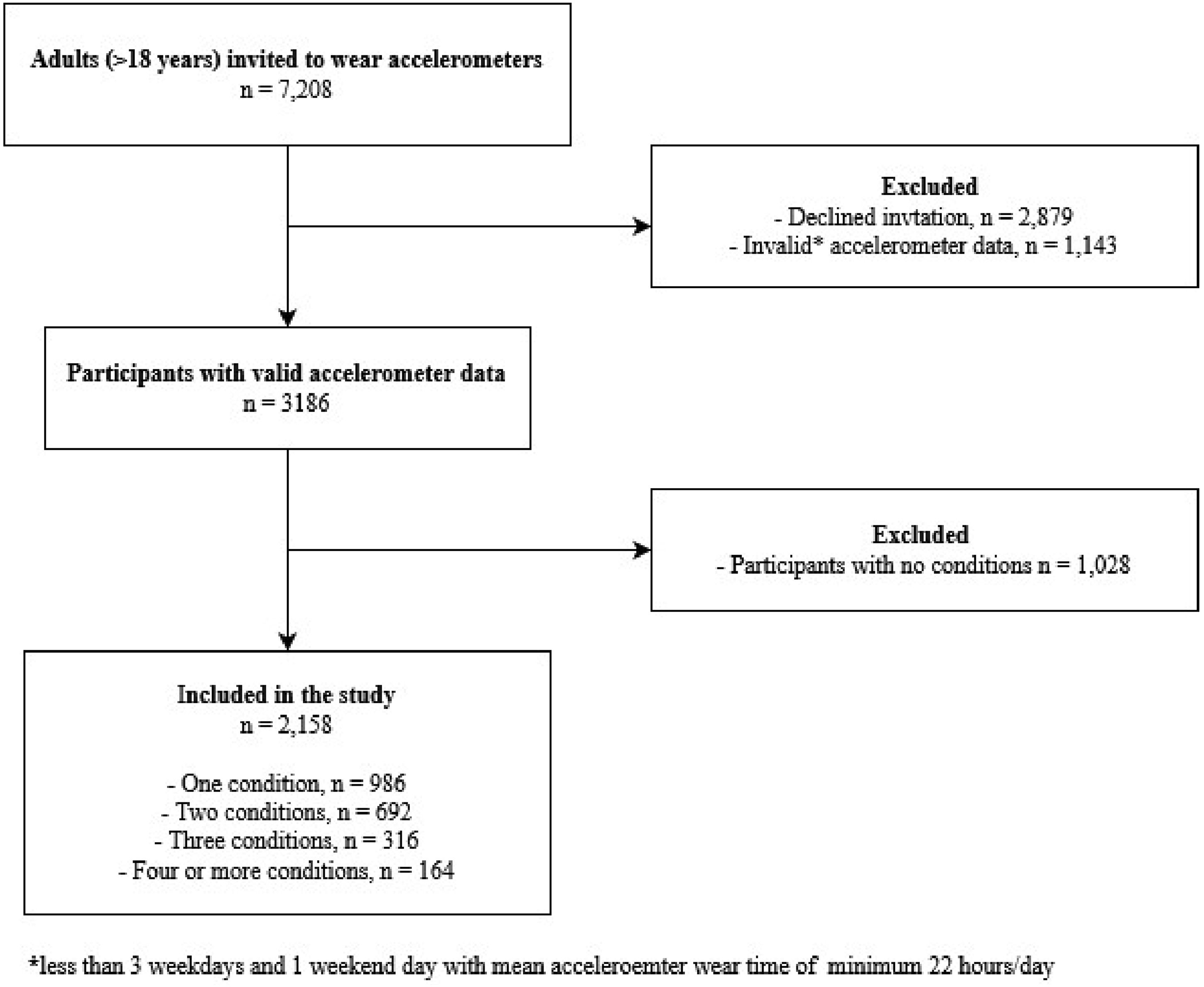
Demographic characteristics and adherence to the WHO recommendations for physical activity (PA) in all participants (n = 2158) and those with one condition or multimorbidity.

BMI: Body Mass Index, SES: Socio-economic status, WHO: World Health Organization, WHO-5: The 5-item World Health Organization Well-Being Index.
Associations between number of conditions and physical activity levels
Sedentary behavior
Physical activity (PA) level and unadjusted and adjusted multiple linear and quantile regression analyses of the association between the number of conditions and daily PA levels at the intensities SB, LPA, MPA, VPA, and MVPA and number of daily steps.

PA levels are presented with mean ± standard deviation for SB and LPA and median and interquartile range for MPA, VPA, MVPA and daily number of steps.
Regressions are presented with β coefficients and mean with 95% Confidence Interval (95% CI) for multivariable regressions and median with interquartile range (95% CI) for quantile regressions. Estimates are presented as the difference in; 1) minutes of LPA, MPA, VPA or MVPA per day, 2) hours of SB per day or 3) number of steps per day compared with the reference group (one condition). Significant results (p<0.05) are marked with *.
M: Multivariable regression, Q: Quantile regression, PA: Physical activity, SB: sedentary behavior, LPA: light physical activity, MPA: moderate physical activity, VPA: vigorous physical activity, MVPA: moderate to vigorous physical activity.
adjusted for sex and age, badjusted for sex, age, Body Mass Index, Socioeconomic status and civil status.
Light, moderate, vigorous, and moderate to vigorous physical activity
In the fully adjusted model for the PA levels LPA, MPA and MVPA, we found a significant inverse association between the number of conditions and PA in participants with multimorbidity (three or ≥four conditions) compared to those with one condition (mean difference in LPA min/day (95% CI): three conditions; −13.1 (−20.6; −5.5), ≥four conditions; −19.6 (- 29.6; −9.5)), (median MPA min/day (95% CI): three conditions; −3.8 (−5.8; −1.8), ≥four conditions; −4.0 (−6.0; −1.9)), (median MVPA min/day (95% CI): three conditions; −4.4 (−6.1; −2.7), ≥four conditions; −4.3 (−6.9; −1.8)).
For VPA, a significant inverse association was found for all participants with multimorbidity compared to those with one condition (median VPA min/day (95% CI): two conditions: −0.2 (−0.4; −0.0), three conditions; −0.4 (−0.6; −0.1), ≥four conditions; −0.4 (−0.6; −0.2)) (Table 2).
Steps
In the fully adjusted model, we found a significant inverse association between the number of conditions and steps in participants with multimorbidity compared to those with one condition (median steps/day (95% CI) two conditions; −365 (−679; −49), three conditions: −981 (−1352; −611), ≥four conditions: −915 (−1370; −459) steps/day)) (Table 2).
Associations between multimorbidity profile and physical activity levels
Sedentary behavior
Unadjusted and adjusted multiple linear regression and quantile regression analyses of the association between multimorbidity profiles with (n=228) and without (n=944) a mental disorder and daily physical activity (PA) levels at the intensities SB, LPA, MPA, VPA, MVPA, and the number of steps.

Regressions are presented with β coefficients and mean with a 95% confidence interval (95% CI) for multivariable regressions and median with median with interquartile range (95% CI) for quantile regressions. Estimates are presented as the difference in; 1) minutes of LPA, MPA, VPA, or MVPA per day, 2) hours of SB per day, or 3) the number of steps per day compared with the reference group (somatic multimorbidity). Significant results (p<0.05) are marked with *.M: Multivariable regression, Q: Quantile regression, SB: sedentary behavior, LPA: Light physical activity, MPA: moderate physical activity, VPA: vigorous physical activity, MVPA: moderate to vigorous physical activity.
adjusted for sex, age, and socioeconomic status
Light, moderate, vigorous, and moderate to vigorous physical activity
In the fully adjusted model, we found a significant inverse association between a somatic/mental multimorbidity profile and PA at intensity levels LPA, MPA, VPA, and MVPA compared to participants with a somatic multimorbidity profile (mean difference in LPA min/day (95% CI): −12.9 (−21.7; −4.2), (median MPA, VPA and MVPA min/day (95% CI): MPA: −2.1 (−4.2; −0.0), VPA: −0.1 (−0.3; 0.0), MVPA: −3.2 (−5.4; −1.1)) (Table 3).
Steps
In the fully adjusted model, we found a significant inverse association between a somatic/mental multimorbidity profile and steps compared to participants with a somatic multimorbidity profile (median steps/day (95% CI): −831 (−1139; −524)) (Table 3).
Discussion
We found that adults with multimorbidity were sedentary for more than 11 hours per day and that the majority (63% to 81%) did not adhere to the WHO PA recommendations. We also found that the number of conditions was inversely associated with PA levels at all intensities, except sedentary behavior. Finally, we found that the presence of a mental disorder in multimorbidity was associated with lower PA levels at all intensities, except sedentary behavior, as compared to not having a mental disorder.
Comparison to other studies
Adherence to PA recommendations
At least 63% of the participants with multimorbidity in our study did not adhere to the WHO PA recommendations (two conditions: 63%, three conditions: 74%, ≥four conditions: 81%). Other studies have reported similar and higher prevalence of non-adherence to PA recommendations in adults with multimorbidity (67% to 87%) across high-income western countries.38–40 These rates are notably higher than the general adult population in similar high-income western countries, where 36.8% of adults have been reported to be insufficiently physically active. 41 Our results confirm that non-adherence to PA recommendations is high in adults with multimorbidity, and that the number of conditions notably affects the prevalence of non-adherence.
Level of PA
The level of SB in our study exceeded 11 hours/day for adults with multimorbidity. This is notably more than what has been reported in previous studies, e.g. Loprinzi 42 reported about 8 hours of SB/day, and Kandoola et al. 43 reported 5 hours of SB/day. The level of LPA varied from 189.5 min/day in participants with two conditions to 165 min/day in participants with four or more conditions in our study. This is somewhat below previously reported estimates where LPA levels have varied from 273.5 min/day 44 to 440.2 min/day. 45 A systematic review and meta-analysis 20 recently reported MVPA in adults with multimorbidity (two conditions) to be 32.7 min/day and the number of steps/day to be 5,145. This exceeds the estimates found in our study for adults with two conditions (MVPA min/day: 13.3, steps/day: 4,630). The studies mentioned above all included adults with multimorbidity and measured PA levels with accelerometers. However, studies in multimorbidity are generally challenging to compare. 46 This is due to reasons such as the variable use of multimorbidity definitions 47 and different analytical approaches to handling accelerometer data, 48 factors that are likely to affect PA estimates.
Association between the number of conditions and PA
In this study, we found a clear, significant pattern of inverse associations between the number of conditions and PA across all PA levels for participants with three or four or more conditions compared to those with only one condition. Overall these results are similar to what has been reported earlier,49–51 demonstrating a relationship between an increased number of conditions and health outcomes. 52 This suggests that the presence of multiple conditions is linked with lower physical activity, potentially due to the compounded effect of various conditions on an individual’s ability to engage in physical activity. However, it is plausible that the increase in physical inactivity is not solely due to the number of conditions but also to the nature and severity of these conditions. For instance, individuals with multimorbidity may experience mobility impairments, pain, or other functional limitations that specifically contribute to reduced physical activity. While our study does not directly measure functional limitations or mobility impairments, these factors are known to affect physical activity levels. Future research should explore how specific conditions within multimorbidity, such as those affecting mobility or causing significant discomfort, impact physical activity levels. This would help clarify whether the increase in physical inactivity is more directly related to functional limitations or the overall burden of having multiple conditions.
We, however, found no difference in associations between participants having two conditions compared to one condition with: LPA, MPA, and MVPA. These results suggest that accumulated conditions need to reach a certain number before they become related to the level of PA.
Data describing the severity of the included conditions were not available in this study and might also have impacted the physical function of the individual participants. For example, the prevalence of chronic pain, which was notably higher in individuals with more conditions (one condition: 26%, two conditions: 40%, three conditions: 80%, ≥four conditions: 92%), may significantly affect physical function and, consequently, physical activity levels. This could have contributed to the findings of this study, which were in accordance with previous studies demonstrating differences in PA levels between people with and without chronic pain.53,54 Future studies should consider the severity and type of conditions as well as pain and mobility impairments to provide a clearer understanding of their specific impact on physical activity.
Interestingly, we did not find evidence of an association between the number of conditions and SB, which may suggest that factors beyond the mere count of health conditions are influencing SB. One possibility could be the high prevalence of SB within the broader population of Region Zealand, from which our sample was drawn. According to data from the Danish National Health Profile, 55 20.9% of the population in this region self-reports being sedentary during their leisure time. This widespread sedentary lifestyle may mask potential differences between individuals with varying numbers of conditions, as the baseline level of SB is already high across the population.
Associations between multimorbidity profile and PA
Previous studies have found that higher mental well-being is associated with higher PA levels in adult populations.56–58 As individuals with mental disorders have lower mental well-being than individuals without mental disorders, 30 we were not surprised to find that the presence of a mental disorder in multimorbidity was inversely associated to the level of PA in our study. However, our results also showed that the presence of a mental disorder in multimorbidity was associated with lower levels of SB compared to having somatic multimorbidity only. This finding is difficult to explain, but it could be related to specific physical activity patterns within the group of participants with a mental multimorbidity profile.
Strengths and limitations
The data used in this study was derived from a population-based study that applied very few exclusion criteria and included more than 2,150 participants. This increases the generalizability of our results. Additionally, the use of probability sampling reduced selection bias and enhanced sample representativeness, further strengthening the reliability of our findings. Another strength was the use of accelerometers, which have been suggested to produce more accurate estimates of PA behaviors compared to self-reported PA measurement methods. 18 Furthermore, in our study, the accelerometer wear time was very high (≥22 hours/day) and exceeded the wear time of 98% of the observational studies that have measured PA with accelerometers, according to a recent scoping review by Evenson et al. 59
However, our study also has limitations. First, the use of a cross-sectional design precludes any conclusions on causal inference. Second, all conditions in the present study were self-reported, which may have led to misclassification or inaccurate reporting of some conditions. Third, the definition of multimorbidity introduces a challenge when comparing results from our study to other studies. The definition of multimorbidity used in our study is the most commonly used and was based on previously published literature, 30 however, a wide variety of definitions of multimorbidity have been used in previous research. 47 Fourth, the included conditions in the LOFUS data collection did not include all 34 conditions recommended in a Delphi consensus study. 60 However, this was not published until after the LOFUS data collection ended. Furthermore, individuals who were unable to walk were excluded from the study, which limits the generalizability of our findings, particularly concerning populations with severe mobility impairments. Additionally, our study may be subject to selection bias, as approximately 56% of invited individuals either declined to participate or had invalid accelerometer data. Due to the lack of access to data on non-participants, we were unable to compare those who were included in the study with those who declined participation. This limitation may affect the generalizability of our findings, as the characteristics of non-participants could differ in ways that impact PA levels and health conditions. Furthermore, we did not have data on the proportion of participants with multimorbidity who declined the invitation to wear accelerometers, which may also influence the representativeness of our sample.
Clinical implications
PA has the potential to prevent and treat numerous chronic conditions4,61 and may provide part of the solution on how to minimize the projected burden of multimorbidity. Our findings indicate that there is an increased burden of physical inactivity when multimorbidity consists of three or more conditions or when a mental disorder is present in multimorbidity. Overall, these findings provide useful insight to health-care professionals and researchers involved in the development of treatment programs for people with multimorbidity.
Even though this study did not find evidence of an association between number of conditions and SB, high levels of SB were observed across all condition groups. Since health benefits can be obtained not only by adhering to the recommended level of weekly MVPA, but also by replacing SB with PA regardless of the intensity level, 6 our results highlight potentials for health benefits if addressed by the individual or society.
Conclusion
For participants with multimorbidity, the level of SB surpassed 11 hours per day, and the majority did not adhere to the WHO PA recommendations (two conditions: 63%, three conditions: 74%, ≥four conditions: 81%). The number of conditions was significantly inversely associated with all PA levels, except for SB, and number of daily steps. Furthermore, our study showed that the combination of somatic and mental conditions in multimorbidity is associated with lower levels of PA compared to somatic multimorbidity only. Overall, our findings suggest that physical inactivity increases as multimorbidity becomes more complex. Future research confirming our findings is needed. To enhance generalizability, such research would benefit from including large population-based samples representative of adults with multimorbidity and incorporating accurate measurement methods to investigate all aspects of PA behavior.
Supplemental Material
Supplemental Material - Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study
Supplemental Material for Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study by Lars Bo Jørgensen, Sofie Rath Mortensen, Lars Hermann Tang, Anders Grøntved, Jan Christian Brønd, Randi Jepsen, Therese Lockenwitz Petersen, and Søren T. Skou in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study
Supplemental Material for Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study by Lars Bo Jørgensen, Sofie Rath Mortensen, Lars Hermann Tang, Anders Grøntved, Jan Christian Brønd, Randi Jepsen, Therese Lockenwitz Petersen, and Søren T. Skou in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study
Supplemental Material for Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study by Lars Bo Jørgensen, Sofie Rath Mortensen, Lars Hermann Tang, Anders Grøntved, Jan Christian Brønd, Randi Jepsen, Therese Lockenwitz Petersen, and Søren T. Skou in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study
Supplemental Material for Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study by Lars Bo Jørgensen, Sofie Rath Mortensen, Lars Hermann Tang, Anders Grøntved, Jan Christian Brønd, Randi Jepsen, Therese Lockenwitz Petersen, and Søren T. Skou in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study
Supplemental Material for Associations between number and type of conditions and physical activity levels in adults with multimorbidity - a cross-sectional study from the Danish Lolland-Falster health study by Lars Bo Jørgensen, Sofie Rath Mortensen, Lars Hermann Tang, Anders Grøntved, Jan Christian Brønd, Randi Jepsen, Therese Lockenwitz Petersen, and Søren T. Skou in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
The Lolland-Falster Health Study (LOFUS), Nykøbing Falster Hospital, Denmark, is a collaboration between Region Zealand, Nykøbing Falster Hospital, and the municipalities of Lolland and Guldborgsund. The authors are grateful to LOFUS for making the LOFUS research data available. However, LOFUS bears no responsibility for the analysis or the interpretation conducted within this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Søren T. Skou is the associate editor of the Journal of Orthopaedic & Sports Physical Therapy and has received personal fees from Munksgaard, Nestlé Health Science and TrustMe-Ed. He is co-founder of Good Life with Osteoarthritis in Denmark (GLA:D®), a not-for-profit initiative hosted at the University of Southern Denmark aimed at implementing clinical guidelines for OA in clinical practice. None of the other authors have competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by The Næstved-Slagelse-Ringsted Hospitals Research Fund, Region Zealand [Program grant, Exercise First], and The Danish Health Confederation through the Development and Research Fund [Grant No 2703]. Furthermore, Professor Søren T. Skou has received two grants from the European Union’s Horizon 2020 research and innovation program [Grant agreement No 801790 (MOBILIZE) and 945377 (ESCAPE)].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.