
Abstract
Background
While physical activity is widely recommended for many long-term conditions, it may be difficult to achieve for patients managing multiple conditions. We aimed to determine the feasibility of an inter-agency exercise and education programme for patients with multimorbidity in primary care.
Methods
We conducted an uncontrolled pilot study with adults with multimorbidity, recruited in two community healthcare organisations in an urban area in Ireland. The six-week pilot intervention combined an individually tailored gym-based exercise programme and education to support self-management. Feasibility of the Activ8 programme was assessed using a mixed methods process evaluation. Outcome measures at baseline and at 6 weeks included recruitment and retention, gait speed, grip strength, quality of life and self-efficacy. Focus groups and interviews explored participants and facilitators’ perceptions of the programme.
Results
19 participants with ≥2 chronic conditions were recruited over three-weeks with similar attrition at both sites (≤40%). Overall, the results indicate that Activ8 was feasible and acceptable to patients and practitioners. Quantitative outcome measures suggested improvements in most outcomes. Qualitative data analysis indicated that Activ8 addressed an overarching concept of patient-centeredness among participants. Three key themes included perceived personal programme impact, the personalised composition of the programme and the evolving nature of primary care practice.
Conclusion
While further definitive evidence is needed and attrition from the programme needs to be considered, the Activ8 Programme was acceptable to both patients and professionals in two different primary care areas with the potential for positive impacts for adults living with multimorbidity.
Background
Average life expectancy is increasing worldwide and so too are the numbers of people living with multiple chronic medical conditions. Multimorbidity is commonly defined as the co-occurrence of two or more long-term health conditions in an individual. 1 The prevalence of multimorbidity depends on the definition used and the population studied and has been reported from 17–98 %.2–5 Multimorbidity is associated with reduced quality of life, increased healthcare utilisation and an increased risk of mental health difficulties.6–9 National data from Scotland highlighted that higher prevalence is associated with deprivation and ageing. 6 This study also reported that 30% of 45–64 year olds presented with multimorbidity and given the higher numbers of people in this age range, in absolute terms there are more middle-aged people with multimorbidity despite the perception that is predominantly an issue for older adults. 6 We previously conducted a systematic review of 37 studies, which demonstrated that multimorbidity is associated with poorer function and with future functional decline. The review indicated that there is greater functional decline in patients with higher numbers of conditions and greater disease severity. 10 Patients with poorer physical function may be less able to engage in physical activity, which may then worsen health through weight gain or other negative effects on well-being.
Results from systematic reviews of interventions for improving outcomes in patients with multimorbidity in primary care and community settings suggested that while further research is needed, future research should focus on functional ability and that consideration should be given to targeting patient health behaviours such as exercise.11,9 In addition, The National Institute for Health and Care Excellence (NICE) Guidance on Multimorbidity recommended non-pharmacological treatments as possible treatment options including dietary interventions, psychological treatments and physical activity programmes. 1 A focus on physical activity and function is also supported by our previous observational study which used data from The Irish Longitudinal Study of Ageing (n = 4,823) to demonstrate that physical function is associated with the development and worsening of multimorbidity over time. 12 It has been reported in the literature that exercising in one’s own community can lead to positive outcomes such as enhanced health and well-being across the lifespan, reduced social isolation and alleviate the harms caused by poverty. 13 Furthermore, research has illustrated that linking health service programmes to existing structures in the community may enhance adoption, implementation, and sustainability. 14 While physical activity is recommended for many long-term conditions, it may be difficult to achieve if patients have multiple conditions to manage particularly if they have co-morbid depression and consequent low energy.15,16 There is mixed evidence for education programmes for patients with chronic conditions. However, there are reports of programmes having significant improvements in quality of life, frequency of activity participation, self-efficacy along with reduced health-care utilisation.17–19 The overall aim of this research study is to describe the development of an inter-agency exercise and lifestyle education programme for patients with multimorbidity. We also aim to examine the feasibility of the intervention for patients with multimorbidity in the community/primary care.
Methods
The methods are reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement: extension to randomised pilot and feasibility trials [Supplemental Appendix I]. 20 In addition to the CONSORT checklist we have also included the TIDieR, Template for Intervention Description and Replication [Supplemental Appendix II] and CERT Consensus on Exercise Reporting Template [Supplemental Appendix III] checklists as additional appendices.
Ethics approval was sought and obtained from the Research Ethics Committee of the Royal College of Surgeons in Ireland prior to conducting this study (REC1285). Approval was also granted from the Health Service Executive (HSE) Primary Care Research Committee.
Design
Intervention Development
Details of the back on track and Activ8 programme.

Four Bandura practices to enhance self-efficacy in the Activ8 programme.

The six-week pilot Activ8 intervention was co-delivered by a physiotherapist and a publicly funded City Council fitness instructor (facilitators) in two leisure centres in urban areas in Dublin, Ireland. In Ireland healthcare is provided by both private and public systems /sectors. The public health care system is government funded and overseen by a single national body, the Health Service Executive (HSE). Primary care in Ireland is multi-disciplinary team-based. Services are provided by General Practitioners, public health and practice nurses, allied health professionals and pharmacists. The government supports this model of care. The City Council is the authority responsible for local government in the city and provide public gym facilities to the public. Each session consisted of forty-five minutes of supervised exercise, which were targeted towards patient’s needs and preferences. This was followed by an education talk led by the physiotherapist and themes were informed by those used for the ‘Back on Track’ programme, which had been based on the widely implemented Chronic Disease Self-Management Support Programme. 18 Overlapping themes were education on pain management, exercise and nutrition with five further key themes were included in the six education sessions (Table 1). Sign posting to additional supports such as relevant websites, local public services and community events e.g. Park Run occurred throughout the programme. A dietician reviewed and advised on the nutrition session content and a clinical psychologist reviewed and advised on the sleep and stress sessions. Participants in the programme were offered supported warm up on gym equipment (this became self-directed at week 4) and optional group stretches. This was followed by circuit style programme led by the fitness instructor, with input from the physiotherapist as needed. The options on the circuit were stationary bike; treadmill; cross trainer; mat exercises; step ups; sit to stand exercises; squat exercises; arm weights and lower limb exercise machines.
Uncontrolled Pilot Study setting
The feasibility testing and piloting of the Activ8 programme took place in two sport and leisure centres in Dublin city and county. To note, the sites where the intervention was carried out had populations with different socioeconomic levels with Site A being classified as a very disadvantaged area and Site B classified as an affluent area. 25
Participants
Potentially eligible participants were identified by primary care physiotherapists in two community healthcare organisations (comprising of ten primary care centres), known as Site A and Site B. Participants were considered eligible if they were aged over 18 years, presented with multimorbidity i.e. at least two chronic medical conditions, had been referred for community physiotherapy and had the ability to provide fully informed consent. Treating primary care physiotherapists acted as gatekeepers and approached potential participants to assess their interest in participating in the intervention instead of receiving usual physiotherapy care, which is largely given on an individual basis. Interested participants were provided with information leaflets and the treating physiotherapist obtained informed consent. Participants were excluded if they had a severe communication disability, behavioural disorder or cognitive deficit that would compromise their ability to participate in the intervention or complete the questionnaires or if they presented with an uncontrolled condition that would compromise the participant’s ability to undertake physical exercise as judged by the physiotherapist. The Physical Activity Readiness Questionnaire (PAR-Q) was also completed by the participating physiotherapist with the potential participant and was used to assess whether the patient needed to check with their doctor before becoming physically active [Supplemental Appendix IV].
Quantitative Outcomes
The primary outcome for this pilot study was feasibility therefore a range of outcome measures based on the aims and objectives of the study were included, to explore feasibility of their use and potential impact of the intervention.
At baseline participants in the programme were asked to complete two self-report questionnaires, the EuroQol five dimensions Visual Analogue Scale (EQ-5D-3L VAS) and the Stanford Self-efficacy Questionnaire (SSE).26,27 The EQ-5D-3L was selected as a valid and reliable self-report questionnaire for describing health related quality of life. 27 It was also chosen in order to enable comparison with other studies and to explore its use in relation to a future cost-effectiveness analysis, however, but given pressures on time to complete questionnaires, only the VAS was included. The Stanford Self-Efficacy Questionnaire was chosen as a validated measure of patient’s self-efficacy levels and the proposed theoretical understanding of the study was based around self-efficacy. 26 In addition, participants completed a grip strength test using a calibrated dynamometer 28 along with a Six Minute Walk Test. 29 Grip strength and gait speed have been shown to be reliable measures of physical function. 30 All participants in the programme were also asked if they currently met the WHO guidelines for physical activity (moderate intensity for ≥150 minutes per week). The research physiotherapist (AR) administered these outcome measures pre and post completion of the intervention and was not blinded to the results, however, she was not involved in the delivery of the Activ8 intervention. The participating physiotherapists and Fitness instructors were blinded to the pre and post completion results.
Qualitative evaluation
Following the Activ8 intervention, focus groups were organised with participants in the programme to explore their experience of participation in the programme. Interviews were also conducted with each facilitator individually. A research physiotherapist (AR) not involved in the delivery of the programme completed the semi-structured interviews and the focus groups. Prior to, during, and after data collection, the researcher reflected on her role in the study using a hand-written diary and also in discussions with colleagues not involved in the study. This process of reflexivity served to identify any preconceived notions and perceptions of the research and thus to identify and address potential sources of bias. The interview questions were derived from the existing literature together with components that were considered relevant to the Activ8 programme. Supplemental Appendix V contains details of the questions that were used to guide the focus groups with the individuals with multimorbidity and the semi-structured interviews with the facilitators of the programme.
Qualitative data analysis
The researcher (AR) transcribed the focus groups and interviews verbatim. Each participant was assigned a code to safeguard anonymity in the transcript. The transcripts were examined separately by two researchers (AR and RG) using a process of thematic analysis as described by Braun and Clark (2006). 31 This form of analysis provides six methodical stages to the analysis process and while the overall approach is inductive, it enables the inclusion of a priori as well as emerging concepts when coding. 31 Stages 1-2 involved reading the transcripts in their entirety to get a sense of the whole and, then using line-by-line analysis; initial codes were identified and noted. The codes were intended to be logical descriptions, which could be easily understood and used by other independent coders. Stages 3-4 consisted of coding the responses to enable the identification of recurring patterns and themes. Stages 5-6 focused on refining these themes and generating evidence from the data to support the themes. 31
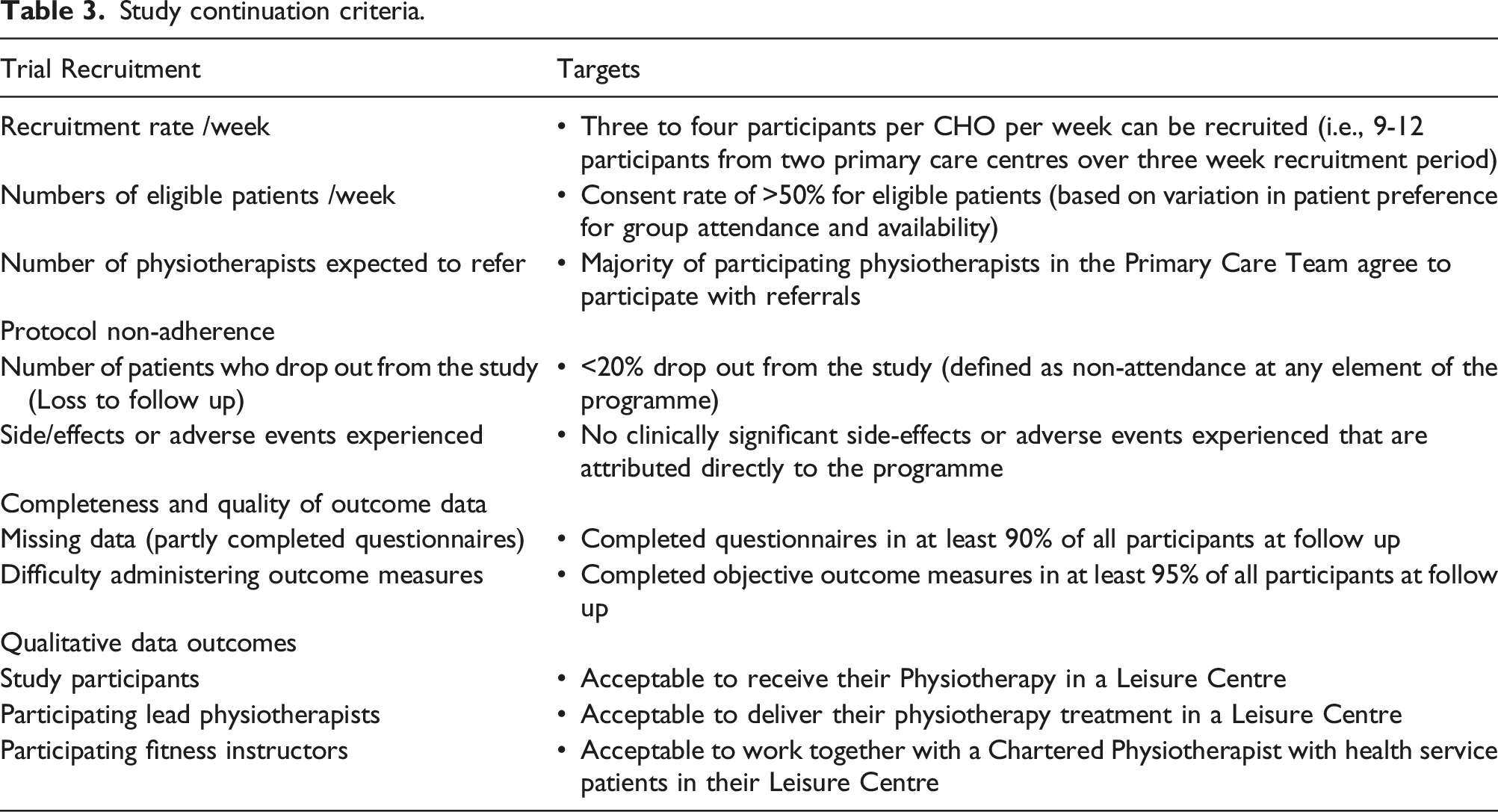
Continuation criteria
Study continuation criteria.
Sample size and data analysis
The main purpose of our study was to assess the feasibility of our methods therefore a defined sample size was not required 20 however, we aimed to recruit 9-12 subjects from two primary care centres over three week recruitment period. The aim was to test feasibility across a range of participants in different settings. Descriptive statistics were used to represent the quantitative data including percentages, proportions, means and standard deviations, medians and interquartile ranges. As per the CONSORT Guideline extension for pilot studies and feasibility trials, inferential statistical analysis was not carried out on the quantitative results secondary to the small numbers included in the study. 20
Results
Continuation Criteria
Recruitment, attendance and attrition
All practicing physiotherapists in each site agreed to participate and make referrals to the study (n = 19). Site A recruited 10 participants and Site B recruited 9 participants, which met the expected number of 18 to 24 participants to be recruited within the three-week period. Another recruitment criterion was to identify the number of eligible patients per week in each CHO. It was difficult to assess this specifically as there was poor compliance with the Daily Recruitment Forms with four out of twenty-one participating physiotherapists returning completed forms. The information requested on this form included; number of patients seen each day; number of patients suitable for recruitment to study; number of patients who consented to participate in the study and reason for declining to participate. To note, the participating physiotherapists gave feedback that the PAR-Q+ form, the physical activity readiness questionnaire of preference, was too long to complete in the allotted appointment time. All participants in the research had been seen at least once by a primary care physiotherapist.
Demographic details of patients referred to the Activ8 programme.

Completeness and quality of outcome data
95% of all recruited participants completed their questionnaires. Some assistance was needed with the SSE questionnaire in both intervention sites in terms of literacy (n = 1) and comprehension (n = 1).
Quantitative outcomes
Quantitative results.

Qualitative findings
Ten of the twelve participants participated in the focus groups and the four programme facilitators took part in the semi-structured interviews. Following data analysis, an overarching concept of patient-centeredness emerged across the study participants. Patient-centeredness can be interpreted in different ways and has been defined as care which is ‘congruent with, and responsive to patients' wants, needs and preferences’. 33 Three key themes that illustrated this concept of patient-centeredness were derived including perceived impact of the Activ8 programme, the composition of the programme and the evolving nature of primary care practice. Each key theme is supported by relevant quotations to reflect the extent to which the Activ8 programme was viewed as a positive experience. For the purposes of the data presentation, the responses from the individuals with multimorbidity are identified as Participants 1-10, the responses from the physiotherapists and fitness instructors are identified as Facilitators 1-4.
Perceived programme impact
Both the facilitators (physiotherapists and fitness instructors) and study participants identified significant benefits to the Activ8 programme both physically and psychologically. In terms of physical improvements participants noted that their improvements ranged from increases in range of movement and strength to improvements in energy levels and participation in social activities.
‘I don’t feel as tired as I used to, y’know…. I feel I got more energy, y’know I feel because of my problem y’know with my leg as well I feel that my muscles, my body is stronger’ (Participant 7)
‘The emphasis is just on movement and it’s in an environment that a lot of them are like ‘oh my goodness I, I actually came to a eh eh a leisure centre and I was on a bike or’ so it’s really empowering for them amm’ (Facilitator 1)
In particular, participants across the two focus groups noted an improvement in their confidence. All four facilitators also highlighted this.
‘But when you come into a place like this, you don’t really think about your health or about your problem you’re just focusing on getting stronger and then you see people that are maybe a lot older than yourself and they’re pushing themselves…I think it’s great for confidence’ (Participant 7)
‘so, it’s great, their, their confidence is up even just to go and do that… you know it’s brilliant, even to see that people are coming once the programme’s finished you know’ (Facilitator 3)
Composition of the Activ8 programme
Several study participants commented on the composition of the programme in terms of the group structure, and the timing, frequency, duration, intensity and variety in the content of the intervention.
‘I think it’s very good to have a group situation… Where you have other people feel the same, you don’t feel on your own… So in a social type of thing, it’s very good’ (Participant 2)
‘And we had the commitment for the six weeks, so that was a reason I am going to get this. And then it went along, you got more progressive and you did all the different machines… And then you get them little talks and maybe you knew all those things before but really you don’t bring them to mind all the time’ (Participant 2)
In addition, participants valued the supervision from the facilitators on site.
‘You wouldn’t know what to do unless you had somebody like there helping you’ (Participant 1)
Facilitators also noted that the heterogeneity of the population included enhanced the generalisability of the programme.
‘I thought the fact that it was so broad, the fact it was multi, so, anything from depression to diabetes to that was very practical to the cohort of people that I see every day… Yet it meant that, you could easily find these people, y’know this covers a lots of people’ (Facilitator 2)
Evolving nature of primary care practice
The Activ8 intervention represented a change in the delivery of primary care physiotherapy for several reasons including the inter-agency approach, the setting of the intervention and the management of the client group. The non-traditional environment (leisure centre) and the accessibility of the leisure centre were identified as positive features of the Activ8 programme, noted by both participants and facilitators.
‘I think the environment is really important, that we’ve taken them out of a health centre, we’ve taken them out of a health, be it a hospital outpatients or in our case it’s a health centre, but they’re not coming because their sick y’know it’s, the emphasis is off that’ (Facilitator 1)
However, one participant noted that,
‘I don’t think I, I don’t think I’d use it, myself, I feel it’s a bit of a waste of time… cause the things you’re doing you can do by walking or y’know’ (Participant 5)
In particular, facilitators identified that the inter-agency approach to the delivery of the intervention overcame barriers associated with traditional service delivery in primary care. However, continued collaboration and support from management, in terms of time, human and physical resources, were identified as key criteria to ensure continuity and sustainability of the programme.
‘The lovely thing about it is that it’s so accessible to them they, if y’know it’s it’s, if they finish our programme [primary care physiotherapy] they can come, it’s open from seven in the morning till till ten at night… Seven days a week, it’s, it’s so accessible…. Amm whereas if we see them in the health centre and we finish, that’s it they can’t come back because they need an appointment and it’s a certain time at a certain date, whereas once they’ve got familiar with that environment they can go when they like’ (Facilitator 1)
The autonomy of practitioners was also highlighted as an important aspect of the inter-agency relationship. In addition, communication between practitioners and among client groups was also identified as a key feature to the success of the programme.
‘I think from….. a supervisory role I think that we, we both worked independently, the the, so I think from that perspective is was good because again it meant that I didn’t have to worry about the what else, what everybody else was doing and or that XX [physiotherapist] found the same, that she felt I was coming from a competence looking after the guys from my end as well’ (Facilitator 4)
Triangulation of the data.

Discussion
To our knowledge, this is the one of the first studies to explore the feasibility of an exercise and education programme for patients with multimorbidity in the community. The quantitative results suggested the intervention may have a positive outcome on patient reported measures like such as health related quality of life and self-efficacy and on objective measures of physical function such as grip strength and gait speed. The qualitative findings indicate that the Activ8 programme was acceptable to both patients and facilitators. However, some issues were identified in the areas of trial recruitment, protocol non-adherence and completeness of data, which may reflect the short time frame involved in this feasibility study. Both the qualitative and quantitative data illustrated areas of agreement and dissonance. There was some discord in the areas of recruitment and retention and administration of an outcome measure and these issues need to be addressed before proceeding to next steps. Overall, both types of data substantiate each other. The results of the triangulation were further compounded through the review of continuation criteria. However, in summary, the results suggest that the intervention was feasible and provide strong support for taking the Activ8 programme forward to the next phase of a pilot randomised controlled study.
Findings in the context of the current literature
Multimorbidity remains a developing area of research particularly in the area of potential interventions. Investigating exercise and education interventions for patients with multimorbidity is a growing area of research. The Cochrane review of interventions for improving outcomes in patients with multimorbidity in primary care and community settings included six studies which were predominantly patient orientated with educational or self-management type interventions delivered directly to participants. 9 Two studies included in the 2016 version of this review reported positive results with a focus on functional capacity and activity participation.37,38 Both of these studies had a self-management aspect to their interventions with a focus on self-efficacy, improved physical function and health related quality of life. One of these studies (OPTIMAL), was a parallel RCT that was similar to Activ8 in that it also tested feasibility and included participants with multimorbidity recruited from primary care settings. 17 It also had a group based professionally led (occupational-therapy) six-week self-management support format. The EQ-5D-3L questionnaire was the outcome measure used in common with the current study. OPTIMAL was found to be ineffective in improving health-related quality of life or activity participation at 6-month follow-up. 38 Numerous health benefits of physical activity participation interventions have been reported in the literature which aim to effectively promote the adoption and maintenance of active lifestyles. 39 It has also been reported that education alone is not sufficient to facilitate and enable behaviour change 24 and this is why the Activ8 programme took a different approach through incorporating an exercise participation intervention in its design. A more recent systematic review of multimorbidity interventions suggested that future research should consider targeting patient health behaviours such as exercise. 11
Gitlin (2006) developed a multicomponent intervention to reduce functional difficulties and enhance self-efficacy in older adults with chronic conditions. 37 The programme again was based on self-management techniques and education. This programme differed from Activ8 in that the participants were all aged 70 years or older and regarded as being at risk of falls. In addition, the intervention ran over a six-month period and the participants received five occupational therapy sessions and one visit from a physiotherapist in their own home. 37 There was no overlap between outcome measures used in Activ8 and this study therefore, it is difficult to make direct comparisons. However, the authors did report that their occupational therapy led home intervention was effective in reducing perceived functional difficulties and enhancing self-efficacy and fall-related concerns in their participants. 37 A systematic review of randomised controlled trials examined the benefits and harms of exercise therapy in patients with multimorbidity. 40 The authors reported that exercise therapy appears to be safe and to have a beneficial effect on physical and psychosocial health in patients with multimorbidity, however, they concluded that evidence supporting this was of low quality. Despite this the authors concluded that their research highlights the potential of exercise therapy in the management and care of this population. 40
The findings from our study fit well with qualitative research exploring patient-experienced burden of treatment of patients with multimorbidity. Patients with multimorbidity experience a range of symptoms, but in addition to this burden of illness, they are also affected by the burden of treatment. 41 It has been suggested that potentially unnecessary treatment burden can result in lack of adherence to prescribed medical treatment. 42 This non-adherence in turn could increase the risk of hospitalisation and mortality. 43 A systematic review published in 2017 identified that change of lifestyle is one of the first suggestions by healthcare providers. 41 One study included in the review reported that patients ranked exercise and altering their diet as the most burdensome component of having more than one condition along with frequent reminders of their health problems. 44 Our study addressed these issues by providing a supported exercise programme led by suitably qualified facilitators. The self-management component of the programme covered relevant topics with exercise, nutrition and goal-setting being covered in the education talks, in addition to this, sign posting to local supports was given throughout the programme. This design is supported by a Cochrane review on the effectiveness of activity promotion in primary care which reported that multimodal interventions with tailored information linking to existing exercise programs are more effective than short educational interventions during physician consultation. 45 Treatment burden was not specifically measured in the Activ8 feasibility study however the qualitative evaluation found the participants in the programme were aware that exercise was important in the management of their conditions.
Strengths and weaknesses of the study
We used the MRC framework for the development and evaluation of complex interventions to underpin the study. 21 To note, this framework has been updated since the conduct of our study with greater emphasis on the nonlinear nature of complex intervention development and enhanced PPI involvement. 46 In addition, the CONSORT Guideline extension for pilot studies and feasibility trials standardised reporting guidelines were followed to standardise the conduct and reporting of the research. 20 Our mixed methods approach maintained the integrity of both the qualitative and quantitative data while also taking advantage of the potential for enhanced understanding from combining the two sets of data and findings. 47 We aimed to improve the fidelity of the education programme by providing participating lead physiotherapists with a ‘Facilitators Guide’ to support with the education sessions [Supplemental Appendix VII]. Another strength of the study was that it had a real multimorbidity focus with the number of chronic conditions being reported and no one condition taking precedence. Outcomes used in this study are in keeping with recommendations from a consensus study on core outcome sets in multimorbidity, which involved a wide range of international multimorbidity experts. 48 They identified that quality of life is an essential core outcome in multimorbidity intervention research and that patient-reported impacts and behaviours (self-management behaviour, self-efficacy); physical activity and function are also important outcomes to consider when evaluating interventions. 48 The moderately successful recruitment and retention rates for the Activ8 programme likely reflect the time and resources put into the development and design of our pilot study that was perceived as acceptable to patients with multimorbidity, primary care physiotherapists and Dublin Council fitness instructors. Our results are reasonably aligned with results from a systematic review published in 2021, where the authors investigated recruitment and retention rates in exercise RCTs for people with multimorbidity. 49 They reported an average recruitment rate of 75% and a retention rate of 90% however, the included studies were deemed to be of low quality and therefore results must be interpreted with caution.
Given the uncontrolled design of the study and the small sample size it cannot be inferred that Activ8 programme caused the changes observed. Furthermore, as the results utilised data from two different intervention sites with different physiotherapists and fitness instructors, facilitator variation may have been present, though this is somewhat unavoidable in pragmatic studies set in real world clinical practice. Another limitation is the small number of outcomes considered, including use of the EQ5D VAS alone and a wider range of outcomes could be tested in further studies. The lack of a longer follow up period is also a limitation as longer follow up would have allowed a consideration of the sustainability of the intervention effects, a key consideration for exercise related behaviours. There has been some debate in the literature about the limitations of self-efficacy as a theory, the theory upon which the Activ8 intervention is based. It has been hypothesised that high self-efficacy beliefs do not always guarantee positive outcomes. 50 This is compounded by reports that self-efficacy can be associated with levels of skill and motivation however a model of how this process occurs requires further evidence. 51 Nevertheless, Bandura’s theory fits well with the aims and objectives of the study. A final limitation of the study was the relatively small number of patients with multimorbidity studied. However, the study adhered to guidelines outlined by Eldridge, which recommend that the size of a pilot depend on its aims and should not be powered to detect the effectiveness of the primary outcome. 52 In addition, it has been reported that pragmatic studies, taking into account their obvious disadvantages, have the potential to be an important source of information to inform clinical practice and health care delivery. 53
Clinical and policy implications
This study is in line with Irish national policy and international guidance on physical activity. Healthy Ireland (2013 -2025) encourages co-operation and collaboration between government agencies in order to implement evidenced based strategies at community and local levels. 54 The National Physical Activity Plan for Ireland (2019) promotes and supports new participation programmes with a special focus on disadvantaged communities. 55 In addition, the NICE Guidelines on Multimorbidity recommended exercise as a possible treatment option for patients with multimorbidity. 1 A scoping review published in 2018 reported that providing patient-centred approaches, self-management support interventions and developing training for healthcare providers were the most frequent categories of interventions with the potential to result in positive impact for patients with multimorbidity. 56 This study is in keeping with their recommendations and builds towards developing the evidence base for non-pharmacological interventions like exercise. Specific recommendations about implementing the Activ8 programme into clinical practice cannot be made without further research. However, primary care physiotherapists could consider group-based interventions, as their resources allow, for their patients with multimorbidity as this research demonstrated that a group-based intervention was acceptable and feasible for participants. Furthermore, primary care physiotherapists may also consider engagement with their local councils in order to provide services jointly in locations most accessible to patients.
Areas for further research
This study examined the feasibility of a pragmatic intervention for patients with multimorbidity in the community. In the context of future research studies examining complex multifaceted interventions with an exercise component for multimorbidity, it is important to acknowledge the dimensions of complexity in the intervention: the variability in study participants and organisations targeted, the number of outcomes included, the behaviours required by those delivering or receiving the intervention all are difficult to standardise. The intervention was based in publicly funded leisure centres, which are a non-traditional healthcare setting and the results suggest that their accessibility could encourage adherence to exercise in the long term. However, the continuation criteria results suggest that the study could move through to the next phase of a randomised controlled pilot study. As recommended in the literature when devising interventions for patients with multimorbidity there is a need to balance tailoring interventions to the needs of service users with delivering standardised interventions that are easier to coordinate, monitor, and evaluate.
22
This balance could be achieved by the Activ8 programme with ensuring that certain modifications were incorporated into further research. The next stage of this study should be a pilot randomised controlled trial include the following specific modifications: • To incorporate at least an eight-week recruitment period to ensure adequate numbers are recruited. • To review outcome measures and engage with public and patient participants to input on measures including consideration of using the shortened version of the SSE, inclusion of a treatment burden questionnaire.
57
Also, further consideration of the appropriate health related quality of life measure as evidence continues to evolve on the challenge of using HRQoL to determine effectiveness of interventions for multimorbidity.
11
• To incorporate an objective measure of physical activity such as accelerometers, depending on budget and patient preferences. • To consider sustainability of intervention effect which would involve longer follow up assessment at six or twelve months post programme completion effects. • Inclusion of a cost and health service utilisation measures to support health economic evaluation of the Activ8 programme.
Many participants in the study had complex multimorbidity (n = 14/16), defined as three or more chronic conditions affecting three or more body systems. It is important to include this group as they face particular challenges with higher healthcare utilization, polypharmacy and poorer health outcomes. 58
Conclusion
With the global escalation of chronic diseases and evidence consistently showing that its onset can be prevented or delayed by changing lifestyle behaviours, the Activ8 programme has been developed as a practical and acceptable intervention, designed for the real world. Considering the limited number of exercise and education studies for patients with multimorbidity in the community, this study has contributed to the existing weak evidence base in this area. This study has demonstrated that an interagency exercise and education programme in the community is feasible and acceptable to patients, primary care physiotherapists and publicly funded fitness instructors, though additional care needs to be taken in recruitment to ensure greater programme retention. A larger pilot randomised controlled trial, with the modifications suggested would add further understanding to our knowledge on the most effective approach to the management of the important issue of multimorbidity in primary care.
Supplemental Material
Supplemental Material - Development and feasibility of an inter-agency physical activity and education programme for adults with multimorbidity in primary care: Activ8
Supplemental Material for Development and feasibility of an inter-agency physical activity and education programme for adults with multimorbidity in primary care: Activ8 by Aine Ryan, Susan M Smith, Vanda Cummins, Catriona Murphy and Rose Galvin in Journal of Multimorbidity and Comorbidity
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Board (HRB) of Ireland as part of the HRB Structured PhD in Population Health and Health Services Research (SPHeRE) programme (SPHeRE/2013/01) to A.R.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.